










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.100 n.9 Madrid Sep. 2008
Double pylorus with bleeding gastric ulcer - a rare event
Píloro doble con úlcera gástrica sangrante: un acontecimiento muy poco frecuente
Palabras clave: Píloro doble. Úlcera gástrica. Sangrado intestinal. Endoscopia intestinal.
Key words: Double pylorus. Gastric ulcer. Upper gastrointestinal bleeding. Upper gastrointestinal endoscopy.
Dear Editor,
Double-channel pylorus is a rare condition that has been reported in 0.001-0.4% of upper endoscopic procedures (1). It was first described in 1969 by Smith and Tuttle (2) and seventy cases had been reported in the literature until 2002 (3). Most cases are associated with chronic peptic ulceration but congenital cases and others resulting from gastric carcinoma have also been published (3,4).
Case report
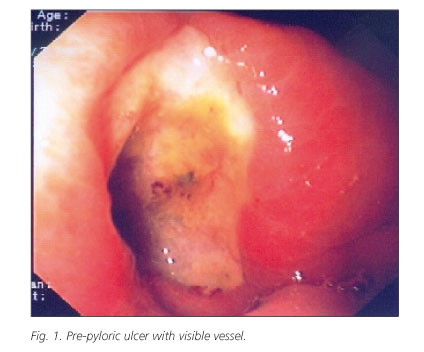
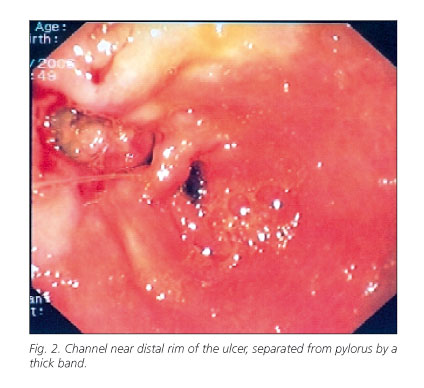
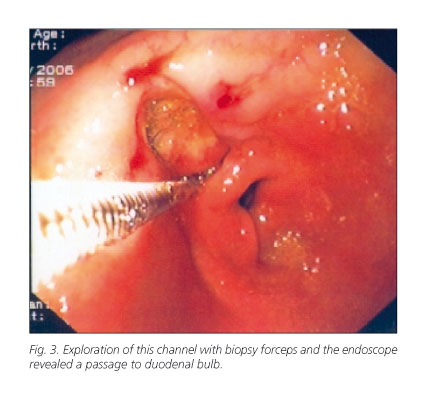
A 88-year-old woman was admitted for epigastric pain and melena that had occurred in the last 15 days, and culminated in an episode of syncope with fall and head injury. She had a history of ulcers and had taken nonsteroidal anti-inflammatory drugs (NSAIDs) intermittently for arthralgias. Blood pressure and pulse rate were within normal range, and once cranioencephalic CT excluded major lesions, an upper gastrointestinal endoscopy was performed. It revealed a large ulcer in the lesser curvature of the pre-pyloric antrum with a visible vessel in its center (Fig. 1) and an opening close to the distal rim of the ulcer (Fig. 2). Exploration of this channel with a biopsy forceps (Fig. 3) and, subsequently with the endoscope, revealed a tract leading to the duodenal bulb. It was separated from the true pylorus by a thick band and together they formed a double pylorus of peptic ulcer origin. Endoscopic haemostasis with adrenaline and absolute alcohol was performed and an intravenous perfusion of proton pump inhibitors was prescribed. Bleeding did not recur and there were no bleeding stigmata in the second-look endoscopy after 48 hours. Recovery was uneventful.
Discussion
Double pylorus is a rare anomaly found in less than 0.4% of upper endoscopies (1,5) with a male-female ratio of 2:1 (5). In most cases it is a complication of peptic ulcer disease, resulting from intramural penetration of the ulcer with adhesions between the stomach and duodenal bulb. Occasionally it may be congenital or secondary to gastroduodenal fistulization by gastric carcinoma (3,4). It is more common in the lesser curvature of the gastric antrum, near the pylorus.
This rare condition is not necessarily associated with dyspeptic symptoms, and most symptomatic cases probably result from a peptic ulcer, which is refractory to medical treatment in the majority of these patients (5-7). In our case, the presenting symptom was gastrointestinal bleeding from the peptic ulcer, a condition rarely reported in the literature (8). It was difficult to establish whether the pseudo-pylorus resulted from fistulization of the present ulcer to the duodenal bulb or whether it was a complication of the previous peptic ulcers reported by the patient. However, this second hypothesis seems more likely and ingestion of NSAIDs certainly contributed to persistence/recurrence of peptic ulcer disease in our patient.
The clinical course in these patients seems to be refractoriness but it is not known if this is due to the ulcer's failure to heal or to the unclosed fistula (5). Treatment with anti-ulcer medication must be rapidly instituted and biopsies from the ulcer and the pseudo-pylorus are essential to exclude malignancy. Although closing of the second channel or fusion of both channels (real pylorus and pseudo-pylorus) only occurs in a small percentage of patients, surgery is reserved for symptomatic patients with ulcer recurrence, who are on strong anti-ulcer medication. Endoscopic treatment is also feasible using a biliary sphincterotome (7).
Our case is an example of acquired double pylorus found by chance, because the related peptic ulcer bled and an urgent endoscopy became necessary to achieve haemostasis. This is a rare event that may occur only one or twice in all working life of an endoscopist.
N. Almeida, J. M. Romãozinho, M. Ferreira, P. Amaro, L. Tomé, H. Gouveia and M. Correia Leitão
Department of Gastroenterology. Coimbra University Hospital. Portugal
References
1. Wiseman SM, Tan D, Hill HC. Double pylorus: an unusual endoscopic finding. Endoscopy 2005; 37: 277. [ Links ]
2. Smith VM, Tuttle KW. Gastroduodenal (pyloric) band. Gastroenterology 1969; 56: 331-6. [ Links ]
3. Mylonas A, Papaziogas B, Paraskevas G, Fragos E, Gigis P, Papaziogas T. Congenital double pyloric ostium in the adult. Surgical Endoscopy 2002; 16: 1639. [ Links ]
4. Matsuyama E, Nagashima R, Watanabe S, Takahashi T. Endoscopic hemostasis for hemorrhage from gastric cancer complicated by double-channel pylorus. Gastrointest Endosc 2001; 53: 679-8. [ Links ]
5. Hu TH, Tsai TL, Hsu CC, Lu SN, Hsiao M, Changchien CS. Clinical characteristics of double pylorus. Gastrointest Endosc 2001; 54: 464-70. [ Links ]
6. Hunt RH, Day RC, Jewell DP. Acquired double pylorus. BMJ 1978; 1: 759. [ Links ]
7. Graham SM, Lin F, Flowers JL. Symptomatic double pylorus: successful treatment with a biliary sphincterotome. Surg Endosc 1994; 8: 792-3. [ Links ]
8. Akazawa Y, Mizuta Y, Osabe M, Nakamura T, Morikawa S, Isomoto H, et al. A case of double pylorus caused by recurrent gastric ulcers: a long-term endoscopic observation. Dig Dis Sci 2005; 50: 2125-8. [ Links ]

