










My SciELO
 Custom services
Custom servicesServices on Demand
Journal
Article
 text in
text in  English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mailIndicators
-
 Cited by SciELO
Cited by SciELO -
 Access statistics
Access statistics
Related links
-
 Cited by Google
Cited by Google -
 Similars in
SciELO
Similars in
SciELO -
 Similars in Google
Similars in Google
Share

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
Print version ISSN 1130-0108
Rev. esp. enferm. dig. vol.110 n.1 Madrid Jan. 2018
https://dx.doi.org/10.17235/reed.2017.5048/2017
PICTURE IN PATOLOGY DIGESTIVE
Hypersplenism secondary to splenoportal axis compression by a giant hepatic cyst
1Servicio de Aparato Digestivo. Hospital Universitario San Agustín. Avilés, Asturias. España
INTRODUCTION
Simple hepatic cysts (SHCs) are formations that contain serous fluid surrounded by normal hepatic parenchyma with no communication with intrahepatic bile ducts. Symptoms develop as a result of their size or complications such as bleeding, rupture, intracystic infection or compression of adjacent structures 1) (2) (3.
CASE REPORT
A 50-year-old female patient was referred to the Hematology Department for thrombocytopenia with no clinical manifestations. Ultrasound and abdominal CT scans revealed a space-occupying lesion (SOL) of the liver, 16 x 11 x 16 cm in size, compatible with SHC, exerting a mass effect on neighboring structures (Fig. 1)

Fig. 1 Abdominal CT scans showing a space-occupying lesion of the liver exerting a mass effect on neighboring structures and resulting in compression of the splenoportal axis.
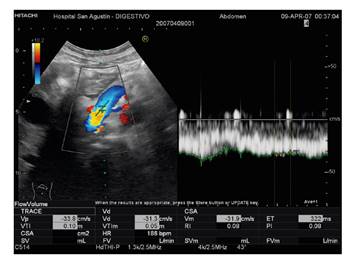
Doppler ultrasonography confirmed a large liver cyst, 20 cm in diameter, which compressed the portal vein and exhibited stenosis and retrograde dilation of 13 mm in caliber, with low velocity flow and a 13 cm splenomegaly (Fig. 2). A pigtail drainage catheter was used, which did not result in any immediate complications, and normal serous fluid was drawn out. A cystogram and sclerosis with absolute alcohol followed 48 hours later.
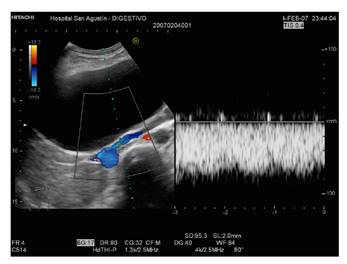
Fig. 2 A doppler ultrasound exam confirming the presence of a SOL of 20 cm in diameter in the liver and portal vein compression with retrograde dilation and slow velocity flow.
Laboratory parameters returned to normal after one month. Doppler ultrasound showed a 3 cm heteroechogenic area with poorly defined contours that corresponded to the residual cavity left behind by the drained cyst (Fig. 3).
DISCUSSION
Hypersplenism from extrinsic splenoportal axis compression is relatively uncommon. In this case, the cyst healed with minimally invasive therapy and ultrasound monitoring. Symptomatic liver cysts may be managed percutaneously (aspiration with/without intracystic injection of alcohol or other sclerosing substances) or surgically. Subsequent monitoring is required until full resolution 1) (2) (3.
BIBLIOGRAFÍA
1. Alvite Canosa M, Alonso Fernández L, Seoane Vigon M, et al. Intolerancia digestiva en un anciano por compresión de quiste hepático gigante. Rev Esp Geriatr Gerontol 2011;46(4)234-5. DOI: 10.1016/j.regg.2011.02.003 [ Links ]
2. Macho Pérez O, Gómez Pavón J, Núñez González A, et al. Quiste hepático simple gigante como causa de disnea en paciente de 93 años. An Med Int 2007;24:135-7. DOI: 10.4321/S0212-71992007000300008 [ Links ]
3. Martos M, Cosme A, Garmendia G, et al. Ictericia por quiste simple gigante de hígado. Rev Esp Enferm Dig 2011;103(2)103-4. DOI: 10.4321/S1130-01082011000200015 [ Links ]
Received: June 06, 2017; Accepted: August 16, 2017
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
