










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
A diverticulum is a limited saccular protrusion of the esophageal wall, communicating with its lumen. Anatomically, esophageal diverticula are classified into pharyngoesophageal, mid-esophageal, and epiphrenic. Depending on the mechanism of occurrence, they are distinguished as pulsatory and traction diverticula. Pulsatory diverticula are formed due to increased intraesophageal pressure and represent a protrusion of the layers of the esophagus through muscle fibers. Pharyngoesophageal diverticula are usually traction diverticula, while epiphrenic diverticula are pulsatile. Epiphrenic diverticula are often combined with other diseases of the esophagus, in particular those associated with impaired motility [1].
Esophageal diverticula are found in less than 1% and are the cause of dysphagia in 1-3% of cases during endoscopy [1]. X-ray studies with contrast agents demonstrate that epiphrenic diverticula are found in 0.015-0.2% of the population [1, 2, 3]. A more selective study, including only patients with identified swallowing disorders, indicates that epiphrenic diverticula occur in 2% of cases. The number of new cases of epiphrenic diverticulum detected is about 1 in 500,000 people per year [4]. This is largely because in most patients, the disease is asymptomatic for a long period until the diverticulum reaches a large size [5]. As a rule, this pathology is detected in patients who are 65 years and older [6].
Epiphrenic diverticula is a rare disease and, even large specialized institutions do not have sufficient experience in treating this pathology [7]. The current case demonstrates a difficult case of a giant diverticulum and the management of postoperative complications.
CASE REPORT
A 54-year-old man was admitted to the hospital with complaints of pain in xiphoid region after eating, dysphagia and bad breath. The symptoms persisted for the last 3 months. During the inspection, no visible changes were found. The patient had several comorbidities: grade II hypertension, grade 3 cardiovascular risk; and stage 1 chronic obstructive pulmonary disease, type A GOLD (Global Initiative for Chronic Obstructive Pulmonary Disease). Body mass index - 22.53, blood pressure - 150/90 mm Hg. Computer tomography (CT) of the chest cavity revealed a protrusion of the esophagus wall anteriorly up to 80x90 mm in diameter, with a vertical size of 60 mm, located at the border of the middle and lower third of the esophagus, 20 mm below the tracheal bifurcation. The size of the diverticulum was 88x60x90 mm, with the presence of heterogeneous contents in the cavity (Figure 1). The lungs were emphysematous, with a few thin-walled air cavities in both apexes. Based on the data obtained, the patient was diagnosed with an epiphrenic diverticulum. Considering the size of the diverticulum, as well as the presence of symptoms, the patient had indications for surgery.
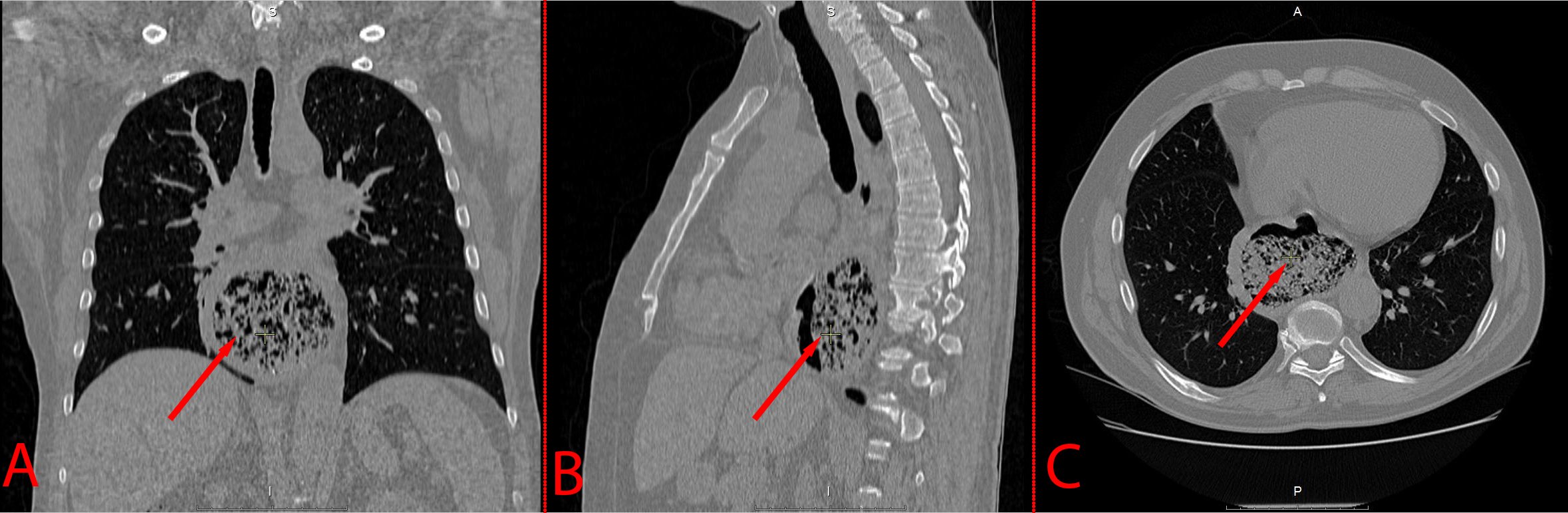
Figure 1. Giant epiphrenic diverticulum.A: Coronal plane; B: Sagittal plane; C: Axial plane (arrow points at the diverticular sac).
Surgical access was performed with lateral thoracotomy on the right in the 5th intercostal space. A diverticulum was fetermined in the lower third of the thoracic esophagus, with a diameter of up to 9.0 cm. The wall of the esophagus in the area of the diverticulum was thin. Taking into account the localization, size and nature of the diverticulum, as well as the state of the esophageal wall, it was decided to perform resection of a part of the esophagus with a diverticulum with proximal resection of the stomach and the formation of an anastomosis (Lewis operation). The esophagus was exposed with a nasogastric tube and transected proximal to the diverticulum. Then an upper midline laparotomy was performed. The stomach was isolated, and a proximal resection of the stomach was performed with a three-row suture with additional covering of the suture line with a continuous atraumatic suture, followed by a diaphragmotomy according to Savvinykh. A circular apparatus was inserted through the gastrotomy along the anterior wall of the stomach, and an apparatus esophago-gastroanastomosis was formed with a circular stapling apparatus. The suture line was additionally reinforced with separate interrupted atraumatic sutures. The gastrotomy opening was sutured in two rows of atraumatic continuous sutures. Hemostasis and aerostasis were performed. The pleural cavity was drained with two silicone drains, which were brought out through the counterpertures. Additional drain was brought to the esophageal opening of the diaphragm through counterperture in the right hypochondrium. The drains were fixed to the skin by suturing. The operation ended with layer-by-layer suturing of the wound. A control CT scan was performed after oral administration of a water-soluble contrast agent. Clear wall defects and “leakage” of the contrast agent beyond the walls of the esophagus and in the area of the anastomosis were not visualized. Laboratory tests demonstrated inflammation and mild deviations: leukocytosis 19.68*109/l (normal range 4-9*109/l), anemia 119 g/l (normal range 130-160 g/l), overestimated ALT 153.9 U/l (normal range up to 45 U/l) and AST 154.8 U/l (normal range up to 35 U/l), underestimated albumin 28.9 g/l (normal range 35-55 g/l) and total protein 55.1 (normal range 66-83). The postoperative period was favorable and proceeded without particularities until the 9th day, when there was an eventration of the abdominal organs. The patient was scheduled for urgent reoperation. During revision, in the area of the lower 1/3 of the postoperative suture, there was a 12 cm long eventration. Aponeurosis diastasis was up to 10-12 cm and the abdominal cavity contained 50 ml of clear, odorless serous effusion. During the revision, there were no pathological changes. The edges of the wound were inflamed; the tissues were loose, edematous. The abdominal cavity was drained. The operation ended with layer-by-layer suturing of the wound. The postoperative period was without complications and the patient was discharged 10 days later. There were no symptoms after a one year follow up.
DISCUSSION
The causes of esophageal diverticula could be a congenital weakness of the wall of the alimentary tract at these points [8]. These sites of weakness may pass unnoticed especially when they are small in size. However, it might be increased in size causing clinical disorders for patients if the intraesophageal pressure is increased. This leads to outpouching of mucosa and formation of diverticula. Moreover, this bulging might be a complication of disorders of alimentary tract motility such as in cases of achalasia [9].
There are three most common diverticula of the esophagus that healthcare professional see in clinical practice: pharyngeal, mid-esophageal and epiphrenic (Figure 2).
There is limited experience in the treatment of epiphrenic diverticula. Even large specialized institutions often have one case per year (anecdotal experience in the literature in the form of single-institution experience) [7]. Reznik et al. reported that operations on epiphrenic diverticula account for only 2% of the volume of operations on the esophagus [10]. The average age of patients is 65 years. The most common symptoms are dysphagia (87%), regurgitation (71%), and chest pain (26%) [7, 11]. Other symptoms include frequent lung infections, halitosis, heartburn, vomiting, and weight loss. Up to 10% of patients are admitted urgently for rupture, perforation, or bleeding of the esophagus [7]. Typically, surgery includes diverticulectomy, myotomy, and an antireflux procedure. Nevertheless, complications occur in 20-35.5% of cases, of which up to 19.4% are serious. In 3.2% of cases, there is inconsistency of the anastomosis. Other complications predominantly include postoperative infections. A rare but formidable complication in abdominal surgery is eventration, which occurs in 0.5-2.35% of patients and requires timely diagnosis and treatment, while associated infections can lead to 40-60% mortality [12]. Diagnosis of diverticulitis is often difficult due to non-specific symptoms associated with diverticulitis outside the classical anatomical area (diverticular disease of the colon). Therefore, non-colonic diverticula are often overlooked [13].
Patients often have concomitant diseases of the esophagus: diaphragmatic hernia (38.7%), achalasia (16.1-24.2%), nonspecific motor disorders of the esophagus (21.2-35.5%), diffuse esophageal spasm (9.1 %), hypertonicity of the lower esophageal sphincter (3%) [7, 14, 15]. Esophageal movement disorders and achalasia, as a rule, occur when the diverticulum is larger than 3 cm [16]. Mortality of surgical treatment reaches 2.8-9.1% [14, 15, 17].
Treatment of esophageal diverticula is based on several basic pathophysiological principles. Small and asymptomatic diverticula do not require specific treatment. Large and symptomatic diverticula require surgical intervention, consisting of diverticulectomy combined with myotomy [11]. The exact criteria for differentiation between small and large diverticula is subjective. However, postoperative results are variable. An excellent result is noted only in 48.2% of cases, good in 27.6% of cases, average in 17.2% and poor in 6.9% [15].
At the same time, given the rarity of epiphrenic diverticula, the approach to their treatment is often chosen individually, taking into account the location and clinical picture of the disease.
CONCLUSIONS
Epiphrenic diverticula are rare even in large specialized institutions, and as a rule, there are no more than one case per year. We describe a case of an epiphrenic diverticulum 88x60 mm in diameter and 90 mm in vertical size, found in a 54-year-old patient. Surgical treatment of this disease was performed according to the Lewis method. At the same time, operations for esophageal diverticula are often associated with various complications. The most common of these are suture failure and wound infections. Our article presents a case of resection of a giant epiphrenic diverticulum with a description of the postoperative period and the development of such a postoperative complication as the eventration of the abdominal organs. Timely detection and surgical correction of this complication is important for achieving good long-term treatment results.

