










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
The increase of overweight and obesity in children and adolescents is a fact registered globally. According to the World Health Organization (WHO) 1, over 340 million children and adolescents aged 5-19 years were overweight or obese in 2016, being obesity one of the main public health problems. In Argentina, different studies have reported a growing trend in the prevalence of overweight and obesity among children and adolescents by assessing body mass index (BMI) following the WHO criteria and cutoff values, as well as the Centers for Disease Control and Prevention (CDC) and the International Obesity Task Force (IOTF) standards 2,3,4,5,6.
Anthropometric assessment is an inexpensive, non-invasive and effective method to screen for malnutrition. The most commonly used indicator to measure overweight and obesity is BMI for age. However, in children and adolescents, it should be used to screen for potential weight and health-related issues, but not as a diagnostic tool. For example, a child may have high BMI for age and sex, but additional assessments would be needed to determine whether excess fat is a problem 7. Besides, measurement of BMI requires height and weight scales, as well as the BMI reference charts 8. An alternative method to diagnose overweight and obesity is the measurement of upper arm circumference, which is used to evaluate growth, protein and energy reserves as well as to provide information about body fat mass 9,10. Upper arm circumference measurement has the additional advantage of being easier and less expensive, since only a measuring tape and reference tables for age and gender are required. Thus, measurements can be easily performed in community and health facilities 11. At the same time, skinfold thickness remains an important and valid anthropometric indicator of regional and total body fatness, especially in research settings 12,13. In Argentina, reference values of upper arm circumference were developed with data from two samples of children from the same city collected in the 70s and the 80s. One of the samples belonged to a longitudinal study of 250 children and the other derived from a cross-sectional study of 1,589 children. However, these references had serious methodological limitations in the generation of smoothed centiles and lacked skinfold thickness data 14,15. The 2000 CDC Growth Charts are the most appropriate percentile criteria to screen for underweight, overweight and obesity in children aged 2-20 years 16,12. They are based on data from 32,600 children from the United States (US) measured between 1963 and 1994. Ages > 6 years were excluded from the revised weight and BMI growth charts to avoid the influence of an increase in body weight and BMI that occurred between NHANES III and the previous national surveys 17. The 2000 CDC Growth Charts include percentiles and z scores for height, weight, weight-for-height, head circumference and BMI, but not skinfold thickness. Thus, Addo and Himes published reference curves for triceps and subscapular skinfold thicknesses 12 and, more recently, Addo et al. developed reference curves for mid-upper arm circumference (MUAC), arm muscle area (AMA) and arm fat area (AFA) for US children and adolescents aged 1-20 years 18. In both studies, data of the 2000 CDC BMI references were used in a nearly identical sample of children not exposed to the obesogenic environment of previous decades. These references provided an important new complementary assessment tool for the interpretation of subcutaneous fat and muscle measures of the arm 12,18.
In a previous collaborative multicentric study conducted between 2003 and 2008, weight and height were measured in a sample of 18,698 children aged 3-13 years living in six provinces of Argentina (Buenos Aires, Catamarca, Chubut, Jujuy, La Pampa and Mendoza) 19. Later, percentiles of weight-for-age and height-for-age were obtained with the LMS method and compared with the WHO and the Argentinean References. The results obtained indicated that children were taller and heavier as compared with the national and international references and that the observed differences in weight-for-age percentiles particularly reflected the effect of the obesity epidemic on Argentinean school-children 20.
The obesogenic environment typical of the last decades may have induced secular changes in MUAC measurement. Further, information of the Argentine population before the obesity pandemic is missing. Thus, the aim of this study was to compare MUAC and the derived measures AMA and AFA in boys and girls aged 4-14 years from Argentina with the reference curves developed for US children and adolescents based on data collected 50 and 25 years ago.
SUBJECTS AND METHODS
POPULATION
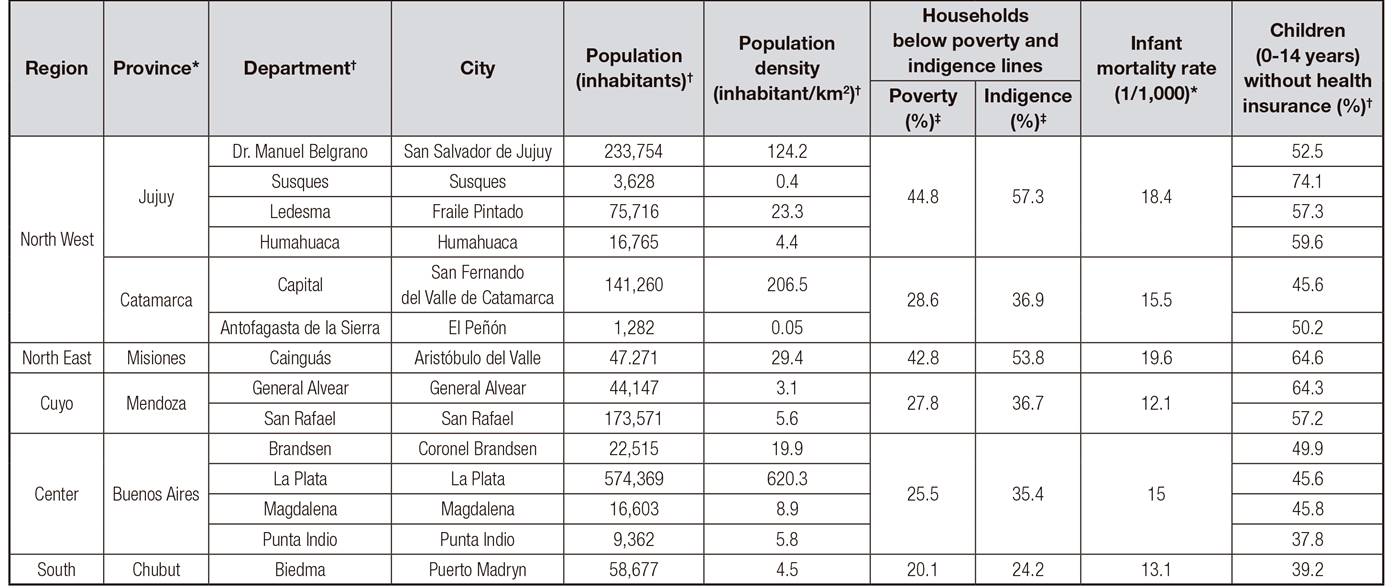
Data were collected in public schools between 2003 and 2010. The study sample consisted of 22,736 school-children aged 4.0 to 14.0 years (11,397 boys; 11,339 girls) from six provinces of the five sanitary regions of Argentina, namely: a) Northwest (n = 2,641), provinces of Catamarca (cities of San Fernando del Valle de Catamarca and El Peñón) and Jujuy (cities of San Salvador de Jujuy, Susques, Fraile Pintado and Humahuaca); b) Northeast (n = 2,206), province of Misiones (Aristóbulo del Valle); c) Center (n = 8,420), province of Buenos Aires (cities of La Plata, Brandsen, Magdalena and Punta Indio); d) Cuyo (n = 6,652), province of Mendoza (cities of General Alvear and San Rafael); and e) South (n = 2,817), province of Chubut (Puerto Madryn). The study regions and their demographic, economic, social and environmental characteristics are shown in Table 1. Sample selection was nonprobabilistic and largely determined by voluntary participation in the study. No cases of chronic diseases or pathological conditions were present among the individuals surveyed.
ETHICS STATEMENT
The study aims and procedures were explained during meetings held at each participating school. Informed consent was obtained from the children's parents or guardians.
In addition, children's oral assent was obtained and only those who agreed were included in the study.
This research was conducted in accordance with the principles proclaimed in the Universal Declaration of Human Rights (1948), the ethical standards instituted by the Nuremberg Code (1947), the Declaration of Helsinki (1964) and its subsequent amendments and clarifications, and national law 25326 (Law 26343/08) and its amendments, regulations and rules for the protection of personal data.
This study was approved by the Bioethics Committee of the Latin American School of Bioethics for the provinces of Buenos Aires, Chubut, Mendoza and Misiones; the Bioethics Committee of the Hospital Escuela Interzonal "San Juan Bautista", Catamarca; and the Bioethics Committee of the Province of Jujuy.
ANTHROPOMETRIC MEASUREMENTS
Anthropometric measurements were taken using standardized protocols 21) by research team members specially trained in these techniques. Intra- and inter-observer technical errors of measurement (< 5%) were calculated before measuring to ensure measurement standardization 22.
The following variables were recorded: age (y), obtained from the children's identification cards or school records; MUAC (cm) on the left arm midway between the acromion and olecranon processes of the ulna, using a non-stretchable measuring tape (Seca®, 1 mm accuracy); and triceps skinfold thickness (TS, cm) on the left side of the body using a constant pressure caliper (Lange®, 1 mm accuracy). The derived AMA and AFA measures were calculated following 23:

STATISTICAL ANALYSES
Raw data dispersion was analyzed using ± 4 standard deviations (SD), eliminating 42 cases from the total (0.18%). This cutoff value criterion is similar to the one used by Alfaro et al. 24. Data were grouped by sex and age groups.
The generalized additive models for location, scale, and shape (GAMLSS) were used to calculate MUAC, AMA and AFA curves, following Stasinopoulos et al. 25. The semiparametric maximum likelihood method was used to estimate smoothed growth curves that could be summarized by the median (M), generalized coefficient of variation (S) and Box-Cox power for skew (L) 18. Locally weighted splines were used to smooth across age and obtain final fitted objective functions to calculate percentiles. Statistical and visual diagnostic tools (worm plots, residual, Owen D-trend plots and examination of the percentile of smoothed curves that were superimposed on the empirical data) were also used to choose the final GAMLSS. All analyses were conducted with the R 3.2.0 software (The R Foundation for Statistical Computing).
Percentage differences (PD%) were calculated in percentiles 3, 50 and 97 by comparing the values of the US reference population ® 18 with those of our Argentinean sample (Sa):

RESULTS
Values and PD% of MUAC, AMA and AFA for R and Sa in percentiles 3, 50 and 97 of 4-14 year-old boys and girls are shown in Table 2, Table 3, Table 4.
Table II. Percentage differences (PD%) in midupper arm circumference (MUAC) values for the reference ® and the study sample (Sa)
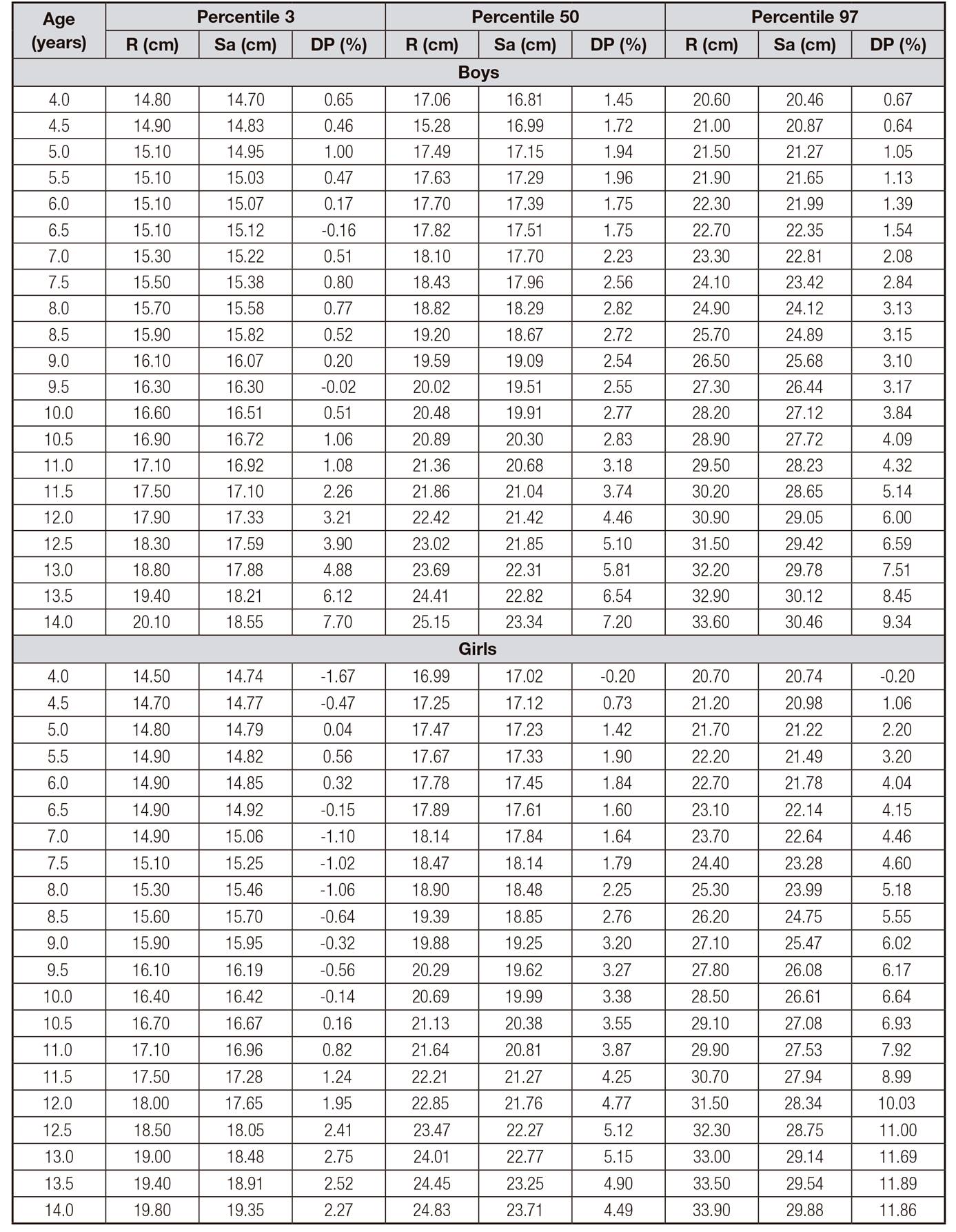
Table III. Percentage differences (PD%) in arm fat area (AFA) values for the reference ® and the study sample (Sa)

Table IV. Percentage differences (PD%) in arm muscle area (AMA) values for the reference ® and the study sample (Sa)

Figure 1, Figure 2, Figure 3 show M, S and L values of MUAC, AMA and AFA, respectively, as well as M values of R.

Figure 1. Comparison of median (M), generalized coefficient of variation (S) and Box-Cox power for skew (L) values of mid-upper arm circumference for age in boys and girls. Black line: Argentinean sample. Grey line: US reference
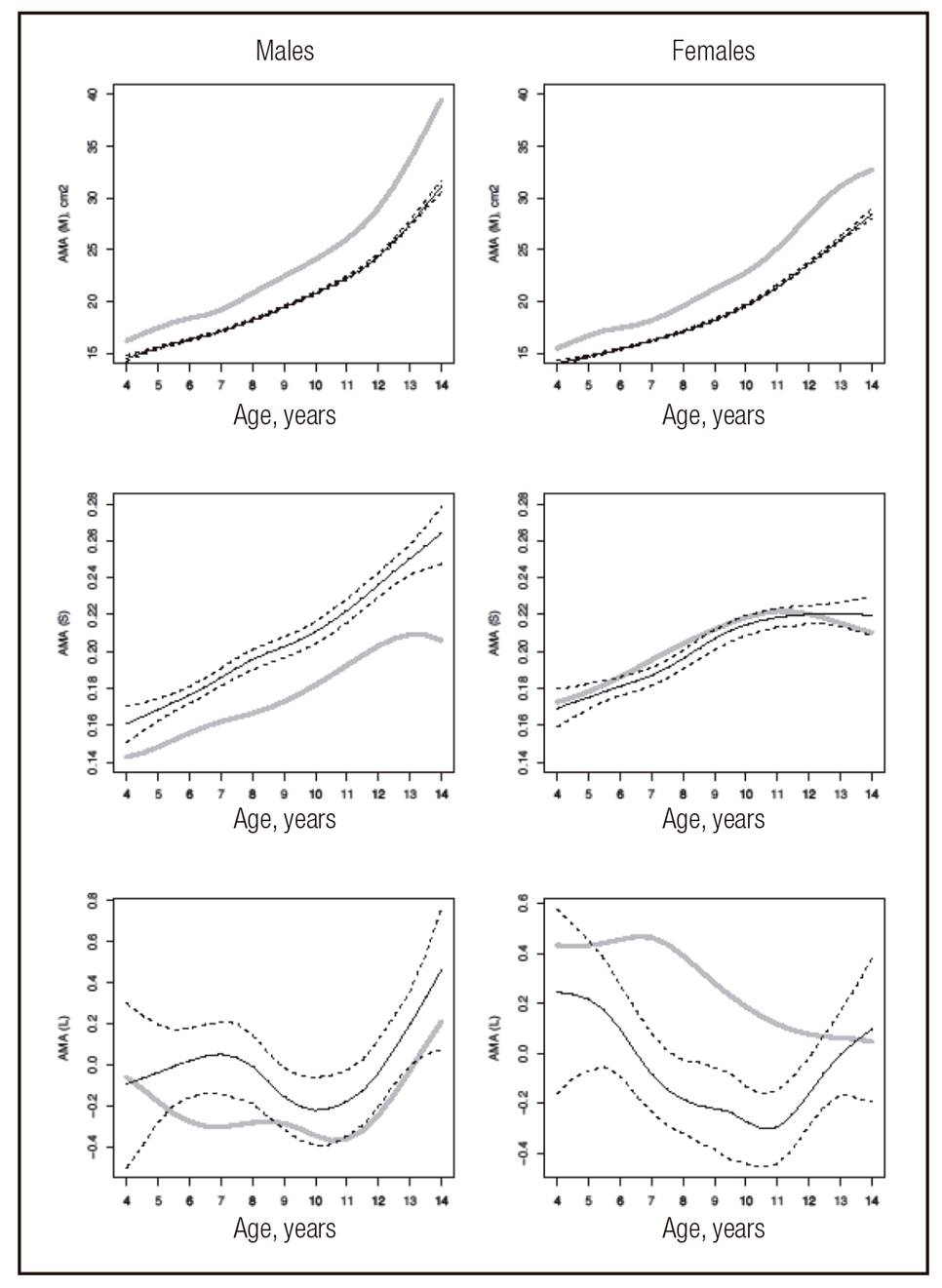
Figure 2. Comparison of median (M), generalized coefficient of variation (S) and Box-Cox power for skew (L) values of arm muscle area for age in boys and girls. Black line: Argentinean sample. Grey line: US reference
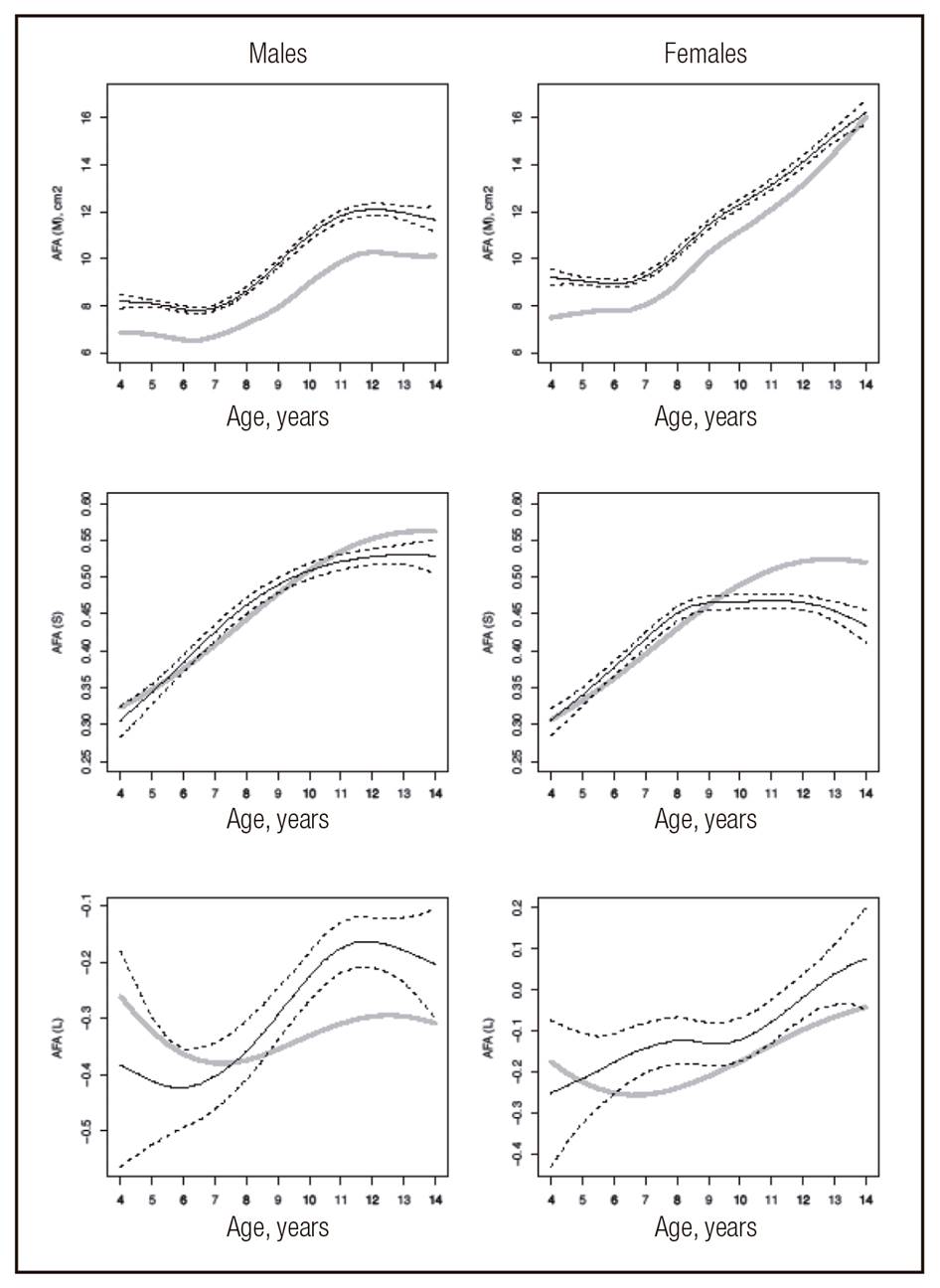
Figure 3. Comparison of median (M), generalized coefficient of variation (S) and Box-Cox power for skew (L) values of arm fat area for age in boys and girls. Black line: Argentinean sample. Grey line: US reference
In general, our results showed that M values in Sa were greater or lesser than in R, depending on the variable analyzed. Thus, MUAC and AMA curves in boys and girls indicated that M values in R were higher than in Sa at all ages (Fig. 1 and Fig. 2). Conversely, in AFA curves of both sexes, M values were lower in R compared with Sa. In all cases, R values were outside the confidence limits of Sa (Fig. 3).
According to the PD% formula, discrepancies between R and Sa values have a plus sign (+) when the R value is greater than the Sa one, and a minus sign (-) when the opposite occurs. Thereby, MUAC and AMA values of Sa in percentiles 3, 50 and 97 were lesser than those of R in both sexes. Such difference increased with age (Table 2 and Table 4). On the other hand, PD% AFA values in percentiles 3 and 50 were negative in boys and girls aged 4.0 to 14.0 years, while in percentile 97, such values were negative in boys from 4.0 to 14.0 years and girls from 4.0 to 9.0 years (Table 3).
DISCUSSION
Several anthropometric parameters have been recently used to complement the BMI-based estimation of nutritional status. Field measurements of MUAC have been used to rapidly identify young children with undernutrition who are at high risk of near-term mortality, especially under emergency situations such as famine or refugee crises 26. On the other hand, various pediatric researchers have attempted to use such measure to screen for overweight and obesity in children and adolescents 27,28. Also, mid-upper arm muscle and fat areas are useful monitoring, evaluation and clinical management alternatives that should be considered for application in different settings 18.
In this study, smoothed percentile curves for MUAC and the derived measures AMA and AFA in healthy Argentinean children and adolescents aged 4-14 years are presented. Thus, this is the first study that considers a large sample of school-children from several provinces, becoming representative of the geographical and sociocultural diversity of our country 19,20.
Our study sample is based on multiethnic groups, the same as that used by Addo et al. 18 to develop the US reference ranges for upper arm circumference.
The particular demographic and genetic background of the Argentine population involves an important, even though variable, contribution of Amerindian, European and African ancestries 29,30.
Percentiles of MUAC and AMA in the present study were comparatively lower in both sexes than those reported by Addo et al. 18. However, AFA percentile values were higher. In the latter case, besides ethnic factors, differences could be partly explained by the temporal differences between samples, since Addo et al. 18 did not include children born during the years in which obesity was recognized as a public health problem. It is known that the prevalence of obesity has increased over the past years worldwide 31,32, and Argentina was no exception 2,4,6,33,34. Also, a previous study analyzing secular changes in body composition of children from Argentina showed that childhood fat tissue increased significantly in the last three decades 35.
The results obtained in this study are consistent with the aforementioned since, on average, AFA increased 19% in boys and 11% in girls in percentile 50 with respect to the reference. Similar results were observed in the extreme percentiles 3 and 97; in the latter, while in boys the magnitude of the differences in Sa decreased from ten years, reference values in girls were greater than those of the sample. So, US obese girls had greater fat area than their Argentinean peers.
The increase in fat area did not correlate with an increase in MUAC, probably because the muscular area had lower values. According to Curilem Gatica et al. 36, evaluation of the muscular component is fundamental, due to the metabolic importance on energy expenditure and the functional capacity granted by normal muscle mass. Such importance may be similar or greater than that of fat mass. The variation of AMA in percentile 50 in both sexes was approximately 15% below the reference. This value was similar in percentiles 3 and 97, and slightly lower in girls.
These results might suggest that the diet eaten by Argentinean children is low in proteins and high in carbohydrates and lipids. Although we did not analyze food habits, a recent study by Zapata et al. 37 describing the changes in food and beverage consumption patterns in the last two decades would support our interpretation. The mentioned authors argued that the dietary pattern of the Argentinian population has shifted in recent years as a result of cultural changes and modifications in food accessibility. They informed a decrease in the consumption of fruits and vegetables, wheat flour, pulses, beef and milk, and an increase in the consumption of pie and pastry-filled crusts, yogurt, pork, semi-processed meat products, soft drinks, juices and ready-to-eat food. Likewise, Aguirre 38 suggested that in Argentina, a single pattern of consumption was replaced by two different types of diets during the past decades: diet for the poor and diet for the rich. The former is based on carbohydrates, fats and sugars and is cheaper, whereas the latter is based on meat, dairy products, fruits and vegetables, is rich in micronutrients and more expensive. Therefore, children who consume diets with excessive amounts of carbohydrates and lipids but deficient in proteins are expected to present overweight or obesity and muscular deficiency, as previously reported in two Argentinean population samples 39,40.
In conclusion, our results confirm differences in upper arm anthropometry of Argentinean school-children with respect to the US reference. The higher adipose tissue and lower skeletal muscle mass observed in Argentinean children could be partly associated with the different ethnic origin of both populations. However, differences should be interpreted in the context of an obesogenic environment, which has favored a calorie-protein imbalance.

