










 Custom services
Custom services
 English (pdf)
English (pdf)
 Article in xml format
Article in xml format Article references
Article references
 Send this article by e-mail
Send this article by e-mail Cited by SciELO
Cited by SciELO  Cited by Google
Cited by Google  Similars in
SciELO
Similars in
SciELO  Similars in Google
Similars in Google 
 Permalink
PermalinkINTRODUCTION
Malnutrition in hospitalized patients is associated with heightened risks of mortality and morbidity (1). While numerous studies highlight a connection between malnutrition and adverse clinical outcomes in Intensive Care Units (ICUs), this relationship is not universally recognized (2,3). The complexity in identifying and diagnosing malnutrition within the ICU context, compounded by pre-existing malnutrition and suboptimal feeding after admission, often results in increased morbidity (4). As such, early and accurate detection of malnourished individuals becomes prior, directing them to appropriate nutritional interventions. Though various screening tools exist for assessing the nutritional risk status of hospitalized individuals, their validation within the ICU population still needs to be discovered. Emerging data suggests that tools like the Modified Nutrition Risk in Critically Ill (mNUTRIC) score and the 7-Point Subjective Global Assessment (7pSGA) Score may be promising. According to specific nutrition guidelines, the Nutritional Risk Screening-2002 (NRS-2002) score is also recommended for ICU patients (5,6).
In parallel, the consequences of malnutrition also appear clearly as muscle atrophy and dysfunction. Muscle mass and function assessments often serve as reliable nutritional status indicators (4,7). The diaphragm, our primary respiratory muscle, displays increased sensitivity to disuse compared to other skeletal muscles. A notable consequence is that patients on controlled mechanical ventilation (MV) experience faster diaphragmatic muscle mass depletion, leading to rapid diaphragm atrophy (8,9). Several conditions, ranging from myopathies and neuropathies to prolonged MV and surgeries, can precipitate diaphragmatic dysfunction (DD) (10-12). DD is a significant loss of muscle force of the diaphragm, compromising respiratory capacity and muscle strength (13). Advances in bedside transthoracic diaphragm ultrasonography (US) have transformed the priority imaging method of diaphragmatic function (14). The technique, validated for both healthy and ICU patients, offers a non-invasive tool to measure diaphragmatic thickness and respiratory thickening (15,16).
Moreover, DD and Diaphragm Atrophy (DA) prevalence in ICU settings is frequent, often correlating with unfavorable outcomes (17,18). While the consequences of critical illnesses and MV on DD and DA are well-documented, the relationship between critical illness-induced nutritional risk status and diaphragmatic muscle function and structure remains unclear. Since malnutrition risk, DD, and DA might be present upon ICU admission, their relationships still need to be explored. Our study aims to clarify the connections between nutritional risk status and both diaphragm muscle thickness and function upon ICU admission.
PATIENTS AND METHODS
PATIENT POPULATION
This study spanned six months in a 9-bed medical ICU. The local Ethics Committee approved the protocol, and informed consent was obtained from the patients or their next of kin. The study involved 50 consecutive patients. Nutritional risk assessment and diaphragmatic measurements were taken on their first ICU day.
Exclusion criteria
− Usage of sedative or neuromuscular blocker agents 24 hours before ICU admission.
− History of neuromuscular disease, trauma, recent abdominal or thoracic surgery.
− Presence of pneumothorax or pneumomediastinum.
− Signs of respiratory fatigue during US examinations.
− Patients previously on MV in assisted or controlled mode.
DEFINITIONS OF MALNUTRITION RISK
Nutritional risk status was assessed using screening tools and Mid Upper Arm Circumference (MUAC) on the ICU admission day, concurrent with diaphragmatic examinations. Nutritional risk assessment tools included the NRS-2002 Score, 7pSGA Score, and mNUTRIC Score. Patients with NRS-2002 scores ≥ 3,7 pSGA score < 6, mNUTRIC score > 4, or MUAC < 22 cm for females and < 23 cm for males were identified as having malnutrition risk (19-22).
ULTRASONOGRAPHIC MEASUREMENTS
Ultrasonographic examinations were performed according to a standardized protocol on the initial day of ICU admission by an intensivist skilled in diaphragm ultrasonography. For patients meeting the inclusion criteria, the right hemidiaphragm was assessed in a supine position. These ultrasonographic evaluations were conducted before any spontaneous breathing trial for patients needing MV support. Each examination typically lasted approximately 10 minutes for mechanically ventilated patients. We used a high-end ultrasonography device (Vivid-Q, GE Healthcare). For measurements, diaphragmatic thickness (DT) was measured using a linear probe (7-13 MHz) in B-Mode, while diaphragmatic excursion (DE) was assessed with a phased array probe (3.5 MHz) in M-Mode. During the ultrasonographic examinations of mechanically ventilated patients, they were temporarily disconnected from the ventilator.
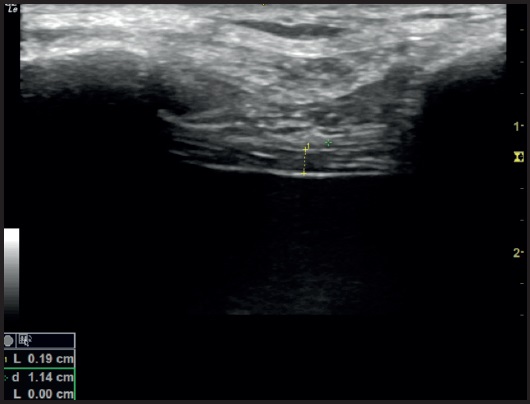
DT was appraised at the zone of apposition, with the probe placed perpendicular to the chest wall in the 8th to 10th intercostal spaces between the anterior and midaxillary lines. Later, the diaphragm was visualized as a hypoechoic structure sided between two echogenic lines, representing the pleural and peritoneal membranes (23) (Fig. 1). Three images from consecutive respiratory cycles were captured during normal tidal breathing for accuracy. The thickness of the diaphragm was measured from the pleural echogenic line to the peritoneal one during both the inspiratory and expiratory phases. The average of these three measurements was calculated, and the thickening fraction (TF) was computed using the formula:

DTins: Inspiratory diaphragm thickness
DTexp: Expiratory diaphragm thickness
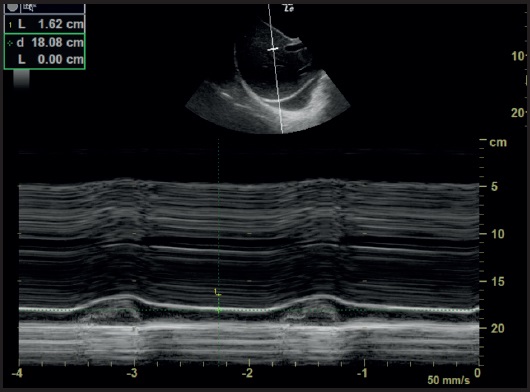
The DE measurements were performed with patients in a supine position. The probe was positioned below the right subcostal margin along the midclavicular line. The diaphragmatic movement was recorded in M-Mode during quiet tidal breathing, noting the distance between peak and trough echogenic lines (Fig. 2). A TF of ≤ 20 % and/or tidal DE of < 10 mm were indicative of diaphragmatic dysfunction (DD). Diaphragmatic atrophy (DA) was determined when the diaphragm thickness measured less than 2 mm at the end of expiration (24). Patients were categorized into two groups based on ultrasonographic findings: those with DD/DA and those without either condition.
STATISTICAL ANALYSIS
Given the absence of prior data on the association between nutritional status and diaphragmatic measurements in ICU patients, a medium effect size (Cohen’s d = 0.05) was anticipated for the primary outcome measures. Power analyses determined a required patient count of 42, with a desired power set at 80 % and a significance level set at 0.05. SPSS for Windows, version 21.0, used all statistical analysis. Both categorical and continuous variables were appropriately represented. Comparisons between DD, DA, and nutritional status were determined by Fisher’s exact and Chi-square tests. Logistic regression ascertained the independent risk factors for DD and mortality, with results shared as odds ratios (OR) within a 95 % confidence interval (CI). A p-value < 0.05 was accepted for statistical significance.
RESULTS
The baseline characteristics of the participants are given in table I. As assessed by MUAC measurements, the risk of malnutrition was 54 %. Based on nutritional screening tools, this risk ranged between 54 % to 78 %. DA was observed in 28 % of patients, while DD was evident in 24 %. While all scoring systems significantly associated higher malnutrition risk with DD (p < 0.05), no such association was found with DA (p > 0.05). Conversely, while MUAC-diagnosed malnutrition risk did not correlate with DD, it was significantly more prevalent in the DA group than in the non-DA group (Table II).
Table I. Characteristics of the medical ICU patients (n = 50).
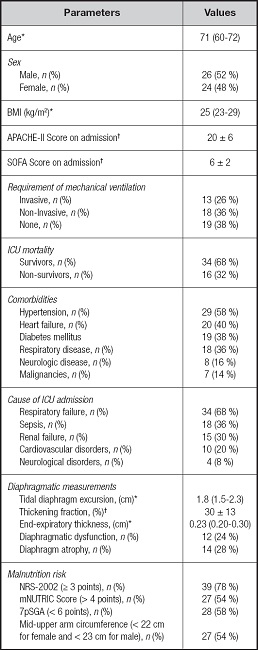
ICU: intensive care unit; n: number; BMI: body mass index; APACHE-II: Acute Physiology and Chronic Health Evaluation; SOFA: Sequential Organ Failure Assessment; NRS-2002: Nutritional Risk Screening-2002; mNUTRIC: Modified Nutritional Risk in Critically ill; 7pSGA: 7 points Subjective Global Assessment.
*Median (interquartile range);
†Mean ± SD.
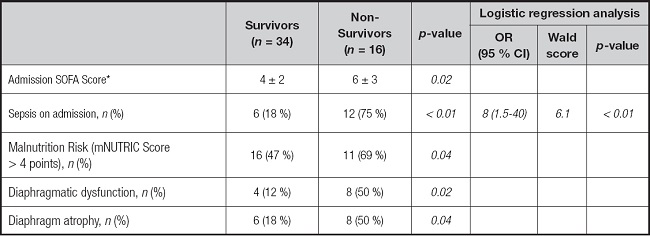
Table II. Factors affecting diaphragmatic dysfunction and diaphragm atrophy in medical ICU patients.
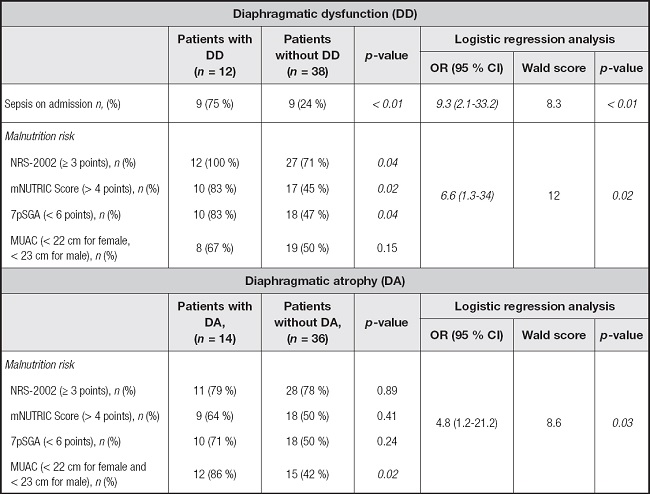
n: number; NRS-2002: Nutritional Risk Screening-2002; mNUTRIC: Modified Nutritional Risk in Critically ill; 7pSGA: 7 Points Subjective Global Assessment; MUAC: mid-upper arm circumference.
When examining the causes, diagnosis of sepsis upon ICU admission (OR: 9.3, 95 % CI: 2.1-33.2; p < 0.01) and malnutrition risk as per the mNUTRIC Score (OR: 6.6, 95 % CI: 1.3-34; p = 0.02) emerged as independent risk factors for DD. However, the sole independent risk factor for DA was malnutrition risk as determined by MUAC (OR: 4.8, 95 % CI: 1.2-21.2; p = 0.03) (Table II). A higher frequency of DD, DA, and mNUTRIC Score-diagnosed malnutrition risk was observed in non-survivors compared to survivors (p < 0.05). However, none of these emerged as independent predictors of mortality (p > 0.05). Notably, sepsis diagnosis upon ICU admission was highlighted as a significant independent predictor of mortality (OR: 8, 95 % CI: 1.5-40; p < 0.01) (Table III).
DISCUSSION
Our study highlights novel observations: ICU patients at risk of malnutrition, as determined by nutritional screening tools upon ICU admission, indicate a higher prevalence of DD. Moreover, malnutrition risk, as per the mNUTRIC Score, is an independent risk factor for DD. Further, our findings indicate that malnutrition risk, as assessed by MUAC, serves as an independent risk factor for DA. Notably, the diagnosis of sepsis upon ICU entry also emerged as an independent risk factor for DD, suggesting a potential link between the acute inflammatory state of sepsis and diaphragmatic dysfunction. Additionally, malnutrition risk ranged between 54 % and 78 %, DA was observed in 28 %, and DD was evident in 24 % of the medical ICU patients.
This study is the initial investigation examining the relationship between nutritional risk status and diaphragm morphology and functionality among ICU patients. Protein-energy malnutrition can lead to muscle wasting, and the diaphragm is no exception. Muscle protein synthesis can decrease while proteolysis can increase in malnourished states, leading to atrophy of skeletal muscles (25). Given the diaphragm’s essential role in respiration, any decline in its functional capacity can have significant clinical implications. Our study emphasizes the association between ICU admission nutritional risk status and diaphragm function and thickness.
Additionally, the mNUTRIC Score incorporates not just traditional nutrition variables but also severity of illness indicators (26). This situation suggests that the interaction between the severity of the disease and nutritional status might play a crucial role in the development of DD in ICU patients.
Our observation that malnutrition risk, as assessed by MUAC, serves as an independent risk factor for DA. MUAC, as a nutritional assessment tool, is simple and non-invasive, providing quick insights into nutritional status. A low MUAC is indicative of muscle wasting and fat loss, which are hallmarks of malnutrition. This relationship between DA and malnutrition risk, as assessed by MUAC, may be explained better with the broader understanding of malnutrition’s role in muscle wasting.
While all scoring systems significantly associated higher malnutrition risk with DD, no such association was found with DA. These results can be explained by one of the concepts indicating muscle mass and the other indicating muscle function. MUAC, as an anthropometric measure, might be more reflective of diaphragm muscle mass, explaining its efficacy as an independent predictor for DA in our study. In contrast, the multifaceted nutritional risk scores may offer deeper insights into diaphragm functionality.
Previous research corroborates the link between diaphragmatic sarcopenia and poor ICU outcomes exacerbated by sepsis (26). On the other hand, the etiology of DD during sepsis remains elusive. Some studies hint at sepsis-induced diaphragmatic damage, attributing it to mitochondrial dysfunction, even in the early stages of the disease (27,28). Our results, identifying sepsis as a potent risk factor for DD, support this theory, suggesting that early mitochondrial dysfunction due to sepsis might be pivotal.
The high prevalence of malnutrition risk on ICU admission in this study, ranging from 54 % to 78 % based on different screening tools, confirms global concerns about malnutrition in the ICU setting, which has previously been linked to adverse clinical outcomes (2,3,29). Remarkably, non-survivors in our cohort exhibited a higher malnutrition risk as assessed by the mNUTRIC Score.
Literature reports a considerable prevalence of DD among medical ICU patients, with figures ranging from 23 % to 36 % (30,31). Our findings align with these statistics, recording a DD prevalence of 24 % and a DA rate of 28 %. Our results emphasize the elevated incidence of DD in ICU patients under malnutrition risk, underscoring the link between muscle mass and nutritional status.
Our study has some limitations. We utilized “malnutrition risk” indicators rather than diagnostic measures of “malnutrition,” such as body composition analyses. Given the complexity of diagnosing malnutrition in ICU settings, our findings should be interpreted cautiously. The limited patient sample size may also restrict the generalizability of our results. Furthermore, integrating pressure-based diaphragmatic metrics, like maximum inspiratory or transdiaphragmatic pressure, could provide a more comprehensive assessment.
CONCLUSION
This study indicates a potentially significant association between the risk of malnutrition, diaphragm function, and thickness upon ICU admission in medical ICU patients. More extensive population-based studies employing objective methods for assessing nutritional status are needed to understand this relationship better.

