










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkNutrición Hospitalaria
versión On-line ISSN 1699-5198versión impresa ISSN 0212-1611
Nutr. Hosp. vol.19 no.2 Madrid mar./abr. 2004
Original
Pre-and postoperative nutritional evaluation in patients with chagasic
megaesophagus
F. A. S. Penhavel*; D. L. Waitzberg**; H. P. Trevenzol*; L. Alves*; B. Zilberstein**; J. Gama-Rodrigues**
* Dept. of Surgery - Discipline of General Surgery - School of Medicine, Federal University of Goiás. ** Dept. of
Gastroenterology - Discipline of Digestive Surgery, LIM 35, School of Medicine University of São Paulo.
| Abstract Chagasic megaesophagus is a chronic disease that courses with progressive dysphagia, regurgitation and protein-calorie malnutrition. Advanced or recurrent megaesophagus can be treated with Serra Dórias operation (cardioplasty, partial gastrectomy and gastrojejunal Roux-en-Y anastomosis). A nutritional evaluation was performed on 27 patients (mean age 58 ± 10 years) with chagasic megaesophagus at admission and after postoperative day 90. The nutritional state was assessed through global subjective nutritional evaluation (GSNE), anthropometry and laboratorial exams, besides the analysis of alimentary intake. In the preoperative period, GSNE pointed to malnutrition in 2/3 patients, while the anthropometric and laboratorial evaluation revealed that over 60% of the patients had protein-calorie malnutrition of the marasmic type. The preoperative nutritional state as evaluated by GSNE did not correlate with complications or postoperative mortality. The postoperative evaluation showed an increase in the intake of proteins, recovery in the body mass index and a reduction in the hemoglobin levels of the peripheral blood. (Nutr Hosp 2004, 19:89-94) Key words: Esophagic achalasia/surgery. Chagas disease/ etiology. Nutritional evaluation. Nutritional disturbance/ diagnosis. Anthropometry/methods. Preoperative care. Postoperative period. Morbidity. Gastrectomy/adverse effects. Follow-up.
| EVALUACIÓN NUTRICIONAL PRE Y Resumen El megaesófago debido a la enfermedad de Chagas es una enfermedad crónica que cursa con disfagia progresiva, regurgitación y malnutrición proteínico-calórica. El megaesófago en fase avanzada recidivante se puede tratar con la operación de Serra Doria (cardioplastia, gastrectomía parcial y anastomosis gastroyeyunal Souxen- Y). Se efectuó una evaluación nutricional de 27 pacientes (promedio de edad de 58 ± 10 años) con megaesófago por enfermedad de Chagas durante el ingreso así como a los 90 días del postoperatorio. El estado nutricional se examinó a través de la evaluación nutricional subjetiva general (GSNE), la antropometría y los datos de laboratorio, aparte del análisis del aporte alimentario. Durante el preoperatorio, la GSNE delató una malnutrición de 2/3 de los pacientes, mientras que la evaluación antropométrica y de laboratorio reveló que más del 60% de los enfermos sufrían una malnutrición proteínico- calórica de tipo marásmico. El estado nutricional preoperatorio, a juzgar por la GSNE, no se correlacionó con las complicaciones ni con la mortalidad postoperatoria. La evolución postoperatoria reveló un aumento del aporte de proteínas, una recuperación del índice de masa corporal y un descenso de los valores de hemoglobina en la sangre periférica. (Nutr Hosp 2004, 19:89-94) Palabras clave: Acalasia esofágica/cirugía esofágica. Enfermedad de Chagas/etiología. Evaluación nutricional. Alteración nutricional/diagnóstico. Métodos antropométricos. Tratamiento preoperatorio. Período postoperatorio. Morbilidad. Gastrectomía/reacciones adversas. Seguimiento. |
Correspondence: FASP Hospital das Clínicas.
Departamento de Cirurgia da FM/UFG.
1ª Avenida, s/n.
Setor Leste Universitário, Goiânia, Goiás,
CEP 74605-020 (Brazil).
Recibido: 18-IX-2003.
Aceptado: 20-X-2003.
Introduction
Acquired megaesophagus is a chronic disease that courses with progressive dysphagia, regurgitation and malnutrition. The regurgitation is associated to the degree of dilation and involvement of the esophagus1.
It is worth bearing in mind that patients with chagasic megaesophagus develop abilities (when feeding) over the years of the disease, which protect them from precocious inanition.
Patients with advanced megaesophagus and recurrent megaesophagus are commonly treated by major surgical interventions. Although malnutrition is frequent in these patients, few studies have determined its incidence and gravity, as well as its effects on the postoperative morbidity and mortality.
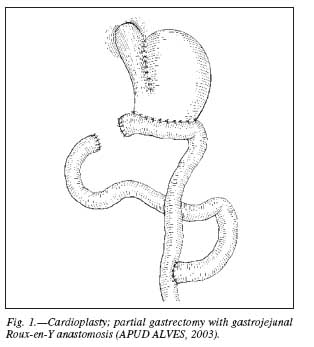
In the city of Goiás, one of the operations practiced to treat advanced chagasic megaesophagus is the Serra Doria operation, which consists of cardioplasty associated to partial gastrectomy and gastrojejunal Roux-en-Y anastomosis.
It is not known how the Serra Dória operation interferes in the patients postoperative nutritional state.
In the present study, on a group of patients with Group IV megaesophagus and recurrent megaesophagus that were candidates for the surgical intervention using the Serra Doria technique, the preoperative nutritional state was evaluated and its influence as a factor of surgical risk together with the postoperative nutritional modifications that occurred in the medium term
Patients and methods
In a period of 18 months, 27 adult patients were included in the study, after informed consent. The inclusion criteria were: age over 18 years; radiologic confirmation of megaesophagus (Group IV or recurrent); and serological diagnosis of Chagas disease2.
The exclusion criteria were: decompensation in myocardiopathy; nephropathy; hepatobiliary disease and diabetes.
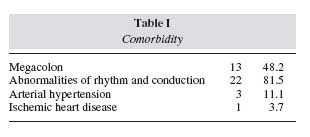
Megaesophagus is frequently associated with other morbid conditions, especially those due to Chagas disease (table I).
The mean age of the population studied was 58 ± 10 years (range, 38 - 80). Twenty patients were male and seven were female. Twenty patients had group IV megaesophagus and seven recurrent megaesophagus.
Eighteen patients were reevaluated after postoperative day 90.
The technical systemization of the Serra Dória operation included cardioplasty by lateral gastroesophageal anastomosis, associated to partial gastrectomy with gastrojejunal Roux-en-Y anastomosis3, figura 1.
Nutritional evaluation
The patients nutritional state was evaluated by the technique of Global Subjective Nutritional Evaluation (GSNE)5 and anthropometric measurements and laboratory methods adopted by Blackburn et al. (1977) 6, including: recent loss of weight; weight/ height ratio; triceps skin fold (TSF), arm muscle circumference (AMC); serum albumin level, serum transferrin level, hematocrit and hemoglobin. Besides these parameters, the serum iron level and ferritin were measured and the body mass index was calculated (BMI)7.
The measurement of caloric intake was obtained by recording alimentary ingestion for three consecutive days8. The theoretical applications were determined by Harris Benedict equation.
The preoperative nutritional evaluation was performed on hospital admission. GSNE preceded any objective method of evaluation.
The patients were operated by day 5 after admission. The postoperative was accompanied until the discharge or death by an observer that had not been informed of any results from the preoperative nutritional evaluation. The postoperative intercurrent diseases were registered according to previous definitions 9.
The postoperative nutritional evaluation took place in the out-patient clinic after postoperative day 90 and according to the same protocol as the preoperative evaluation.
Statistical analysis
Fishers exact test, Wilcoxon test and Students t test for paired data were applied when appropriate. Probability values of p ≤ 0.05 were considered statistically significant.
Results
The preoperative global subjective nutritional evaluation demonstrated that nine patients (33.3%) were classified as well nourished, eleven (40.7%) as moderately undernourished; and seven (25.9%) as seriously undernourished.
The body mass index was under 19 kg/m2 in seventeen (63%) of the patients. Weight loss in the recent past was greater than 10% in seven (26.9%) of the patients in the preoperative.
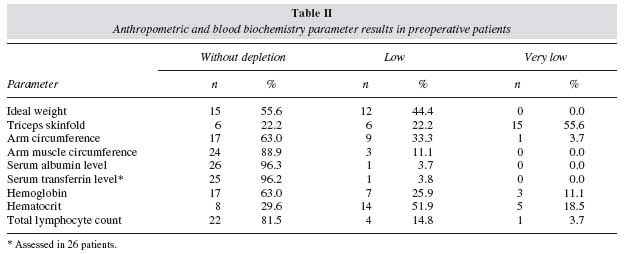
The classification of the patients in the preoperative, according to the frequency of alterations in the anthropometric and laboratorial variables, is given in table II.
The anthropometric variable, with greatest frequently of depletion, was TSF, in 77.8% of the patients; while that with the lowest frequency was AMC, in 11.1% of the patients.
Albumin and transferrin levels were found to be unaffected in 96.3% of the patients.
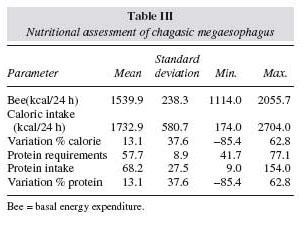
In the preoperative period, the dietary evaluation demonstrated that the caloric and protein intake were higher than the theoretical needs calculated using the Harris Benedict equation (table III).
Regurgitation, when occurring on a daily basis and for more than fifteen days, was considered to be a contributory factor for malnutrition in the preoperative period.
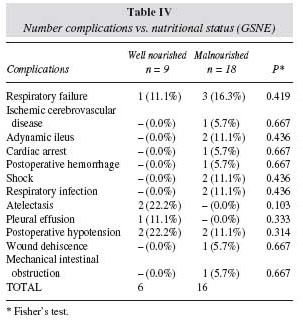
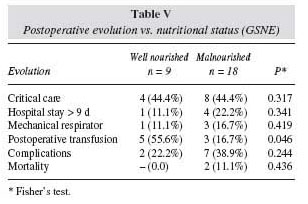
The overall incidence of complications was 33.3%. the association between preoperative nutritional classification (GSNE) and complications and surgical mortality was not significant (tables IV and V).
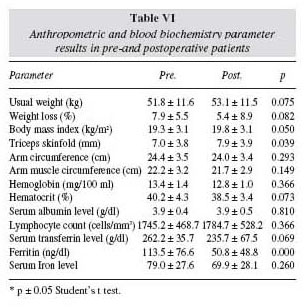
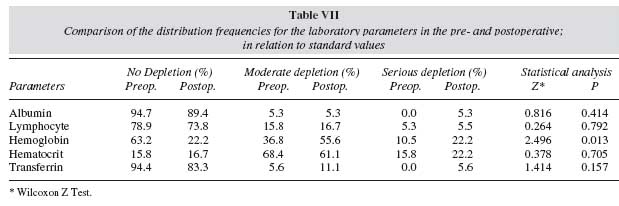
The postoperative follow-up demonstrated that there was an increase in TSF, BMI, and reduction of hemoglobin (tables VI and VII).
The postoperative dietary evaluation demonstrated an increased protein intake (table VIII) in comparison to the preoperative period.

Discussion
Chagasic patients can present alterations of the digestive system, grouped together under the denomination digestive alterations of Chagas disease 10. Of these, megaesophagus and megacolon are the most frequent and the latter was present in 48.2% of the patients of this study.
Cardiac disturbances, identified by the electrocardiogram, are frequent in chagasic patients and have a negative effect on their survival 11. In this sample of patients, 81% presented arrhythmia and/or disturbances in the cardiac conduction.
In Chagas disease, the interval between acute infection and onset of the digestive symptomatology is very variable. When considering the frequency of the disease in relation to age group, an aging of the chagasic population with digestive forms of the disease has been observed in recent years. This is principally due to the prophylactic measures that have been preventing the appearance of new cases1. In the present study, 44.5% of the patients were over 60 years of age.
Preoperative GSNE identified malnutrition in 2/3 of the patients a higher frequency than that reported by other authors.
Detsky et al5 determined malnutrition through preoperative GSNE in 31% of candidates for gastrointestinal surgery.
Waitzberg et al12 diagnosed hospital malnutrition, through GSNE - a frequency of 48.1% in a sample composed of 4.000 clinical and surgical patients.
In the present study among patients with chagasic megaesophagus, the malnutrition determined by anthropometric measurements and by laboratory exams, was the marasmic form, with a reduction in the body mass due to loss of fat, while body proteins were maintained.
The pattern of ponderal alteration we observed suggested chronic loss -considering the disproportion between the frequencies of alterations in the body mass measurements and the weight loss in the present past. This was considered serious, in one fourth of the patients.
Marasmic malnutrition was also observed among patients with chagasic megacolon (without associated dysphagia) and this was attributed to deficient dietary intake13.
In adults, marasmus is characterized by: reduced anthropometric measurements and maintenance of the visceral proteins; insufficient alimentary intake; and, commonly, without complication of the disease´s metabolic response14.
In the present study, an adaptation was observed between the values of protein-calorie intake and the estimated energy expenditure -as much in the pre- as in the postoperative period.
Regurgitation, when daily and for more than 15 days, was considered a contributory factor for preoperative malnutrition; however the total intake was not a reliable indicator in this evaluation period.
In the present sample, albumin and transferrin remained unaffected in 96.3% of the patients in the pre-operative and presented no statistically significant differences in the values observed in the postoperative.
In the postoperative, iron deficiency was detected in 30% of the patients; and hemoglobin suffered a statistically significant reduction (p < 0.05). It is known that transferrin levels can increase with a serious deficiency of iron and anemia15,16. Under these conditions, as observed in the postoperative, the method suffers limitations as a marker for the state of the visceral proteins.
Malnutrition, identified by various methodologies, is associated with greater morbidity and postoperative mortality17-19. As an independent variable, diagnosed by GSNE, it is associated with a higher frequency of infectious or noninfectious complications and mortality19.
In the present study there was no association between malnutrition (GSNE) and complication and postoperative mortality. No other variable that could be adopted as a criterion of postoperative course -such as postoperative hospital stay, time in an intensive care unit or under mechanical ventilation- was correlated with preoperative malnutrition.
Our attention was called to the fact that patients over 60 years of age presented greater morbidity.
Studies that look for an association between modification of the nutritional state and postoperative course suffer criticism in relation to the size of the sample, diversity of the patients and rates of complications associated with a given procedure5.
Furthermore, it is recognized that GSNE predicts complications of nutritional basis and, also, represents an index of disease, even before indicating malnutrition5,20.
In the postoperative, of this work, the complications present in 1/3 of the patients, were predominantly noninfectious. It has been reported that vital functions dependent on the metabolism of protein, which include immunocompetence, are relatively preserved in marasmus and that the albumin rates are important markers of malnutrition, with clinical significance, irrespective of the body weight14.
Chronic malnutrition prevailed in our patients which together with other factors -such as: maintenance of the visceral proteins; reduced number of complications inherent to the operation; sample size; patients´ age and associated diseases- are known to interfere in postoperative results and in the prognostic capacity of GSNE.
With the re-establishment of alimentary traffic, 16 patients (88.9%), referred to a subjective improvement in the alimentary intake. Measurement of this variable in the postoperative detected a significant increase in protein intake, when compared to preoperative levels.
The Serra Dória operation, on the other hand, enabled a partial recovery in the medium term of the nutritional state in terms of body fat.
References
1. Vaz MGM: Contribuição ao estudo clínico, radiológico e endoscópico do megaesôfago chagásico. Goiânia, 1991. Dissertação (Mestrado) - Instituto de Patologia Tropical e Saúde Pública, Universidade Federal de Goiás. [ Links ]
2. Luquetti AO: Evolution of knowledge on the etiological diagnosis of chagasic infection. Mem Inst Oswaldo Cruz, 1999, 94:283-284. [ Links ]
3. Dória OBS: Tratamento cirúrgico do megaesôfago operação de Serra Dória. Rev Goiana Med, 1973, 19:185-93. [ Links ]
4. Alves L: Operação de Serra Dória no tratamento do megaesôfago avançado: resultados imediatos. São Paulo, 2003. Dissertação (Mestrado). Faculdade de Medicina da Universidade de São Paulo. [ Links ]
5. Detsky AS, Baker JP, O´Rourke K, Johnston N, Whitwell J, Mendelson RA and Jeejeebhoy KN: Predicting nutrition associated complications for patients undergoing gastrointestinal surgery. JPEN J Parenter Enteral Nut, 1987a, 11:440-446. [ Links ]
6. Blackburn GL, Bistrian BR, Maini BS, Schlamm HT and Smith MF: Nutritional and metabolic assessment of the hospitalized patients. JPEN J Parenter Enteral Nutr, 1977, 1:11-22. [ Links ]
7. Nightingale JMD, Walsh N, Bullock ME and Wicks AC: Three simple methods of detecting malnutrition on medical wards. JR Soc Med, 1996, 89:114-118. [ Links ]
8. Barrett-Connor E: Nutrition epidemiology: how do we know, what they ate. Am J Clin Nutr, 1991, 54:1825-1875. [ Links ]
9. Buzby GP, Mullen JL, Matthews DC, Hobbs CL and Rosato EF: Prognostic nutritional index in gastrointestinal surgery. Am J Surg, 1980, 139:160-167 [ Links ]
10. Rezende JM: Forma digestiva da moléstia de Chagas. Rev Goiana Med, 1959, 5:193-227. [ Links ]
11. Porto CC: Eletrocardiograma no prognóstico e evolução da doença de chagas. Arq Bras Cardiol, 1964, 17:313-346. [ Links ]
12. Waitzberg DL, Caiafa WT and Correia MITD: Hospital malnutrition. The brazilian nutritional survey (IBRANUTRI): A study of 4.000 patients. Nutrition, 2001, 17:573-580. [ Links ]
13. Vieira MJF, Gama-Rodrigues JJ, Habr-Gama A, Faintuch J, Waitzberg DL and Pinotti HW: Preoperative assessment in cases of adult megacolon suffering from moderate malnutrition. Nutrition, 1996, 2:491-495. [ Links ]
14. Bistrian BR, Sherman M, Blackburn GL, Marshall R and Shaw C: Cellular immunity in adults marasmus. Arch Intern Med, 1977, 137:1408-1411. [ Links ]
15. Young GA, Chem C and Hill GL: Assessment of protein caloric malnutrition in surgical patients from plasma proteins and anthropometric measurements. Am J Clin Nutr, 1978, 31:429-35. [ Links ]
16. Shenkin A and Steele LW: Clinical and laboratory assessment of nutritional status. Proc Nutr Soc, 1978, 37:95-103. [ Links ]
17. Seltzer MH, Slown BA, Cataldi-Betcher EL, Fileti C and Gerson N: Instant nutritional assessment: absolute weight loss and surgical mortality. JPEN J Parenter Enteral Nutr, 1982, 6: 218-21. [ Links ]
18. Bozzetti F, Migliavacca S, Gallus G, Radaelli G, Scotti A, Bonalumi MG, Ammatuna M, Sequeira C and Terno G: "Nutritional" markers as prognostic indicators of postoperative sepsis in cancer patients. JPEN J Parenter Enteral Nutr, 9: 464-470. [ Links ]
19. Correia MITD and Waitzberg DL: The impact of malnutrition on morbidity, mortality, length of hospital stay and costs evaluated through a multivariate model analysis. Clin Nutr, 22: 235-239. [ Links ]
20. Jeejeebhoy KN, Detsky AS and Baker JP: Assessment of nutritional status. JPEN J Parenter Enteral Nutr, 1990, 14:1935-1965. [ Links ]

