










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
The tight relationship among malnutrition, surgery, and poorer outcomes was for the first time established by the classic study of Studley, published in 1936 1. Eighty years later, malnutrition is a common condition in surgical patients, with a prevalence ranging from 20 to 40% 2,3. The deterioration of nutritional status during hospitalization has been associated with longer hospital stay, an increase in morbidity, and a higher economic burden 4.
Preoperative nutrition provided to malnourished surgical patients has been related to the reconstitution of immune function and significant reductions in complications 5) (6. The supply of immunonutrition in the perioperative period reduces the infection rate and shortens the length of stay, although a significant reduction in mortality has not been demonstrated 7. This improvement in the prognosis is associated with a significant reduction in the economic expenditure derived from hospitalization, which exceeds the cost of the intervention 8. Following this evidence, current clinical guidelines encourage active screening for malnutrition in surgical patients and the perioperative provision of nutritional support 9.
Nevertheless, the efficacy of nutritional support beyond hospital discharge has received less attention, in spite of the fact that some changes due to surgery can persist for weeks. In this way, an increase in resting energy expenditure has been observed in patients with peritonitis until 23 days after the injury, accompanied by the reduction in skeletal muscle and visceral protein 10. Furthermore, severe losses of weight, muscle mass, and grip strength have been described 180 days after major surgery 11. Dietary restrictions, anorexia, and gastrointestinal symptoms such as nausea, vomiting, abdominal pain, and diarrhea may persist for a long time after major surgery, compromising an adequate feeding.
A systematic review was performed to test the current evidence about the effects of nutritional support on nutritional status, complication rates, and quality of life, when administered after hospital discharge in patients who underwent gastrointestinal surgery.
METHODS
The systematic review was conducted following the principles of the PRISMA declaration 12.
SEARCH STRATEGY
A bibliographic search was performed in February 2015 using the Medline (PubMed), Trip Database, and Central (Cochrane Library) databases. The following strategy was used for this purpose: ("nutrition" OR "enteral nutrition" OR "nutritional supplements" OR "oral nutritional supplements" OR "sip feed" OR "sip feeding" OR "dietary counseling") AND ("patient discharge" OR discharge OR postdischarge) AND (surgery OR operation OR "surgical procedure").
INCLUSION CRITERIA
The eligibility criteria for including studies in the review were the type of assay (randomized, double-blinded, controlled studies), type of patients (patients undergoing either elective or urgent major gastrointestinal surgery), patients' age (adults), type of nutritional intervention (either dietary counselling, oral nutritional supplements, or enteral nutrition provided after hospital discharge, independently if any nutritional intervention was provided during hospitalization or not), and language (English, Spanish).
EXCLUSION CRITERIA
Non-randomized or non-controlled studies, trials including patients receiving home parenteral nutrition, trials providing nutritional support only during hospitalization, studies in which patients underwent surgical procedures other than gastrointestinal (e.g., cardiovascular, orthopedic, head and neck), and studies that did not fulfil the inclusion criteria were excluded.
TYPE OF INTERVENTION
Any kind of nutritional support that included dietary counselling, oral nutritional supplements (ONS), and/or enteral nutrition provided at hospital discharge. The control group should include no nutritional support or the usual care of the center. Home parenteral nutrition (HPN) was not considered for the purpose of this review. HPN is a complex modality of nutritional support used in a very specific group of patients with intestinal failure. The aim of this systematic review was to evaluate the utility of oral or enteral nutrition in the common surgical patient. The efficacy and effectiveness of HPN has been recently reviewed 13. Nutritional support exclusively provided during the perioperative period was excluded from this review as several previous trials and meta-analysis have evaluated its efficacy.
OUTCOMES
The outcomes of interest were the daily intake of energy and protein (comprising dietary intake and oral or enteral nutrition); nutritional status, assessed either with validated structured tools (e.g., Subjective Global Assessment, NRS-2002, Malnutrition Screening Tool, etc.), anthropometric measures (weight, body mass index, body circumferences, skinfold thickness), body composition (e.g., muscle mass or fat mass measured with bioelectrical impedance), or muscle strength (e.g., grip strength measured with dynamometry); complication rate at discharge, including infections, mechanical complications of surgery (e.g., anastomotic leak), mortality, and re-hospitalization; quality of life measured with any validated survey; and the cost-effectiveness of the intervention (e.g., incremental cost-effectiveness ratio).
DATA COLLECTION
Data were collected from the selected trials by the authors in an independent manner using a common structured form. Outcome measures were recorded as mentioned in the publication, either as intention to treat analysis or per protocol.
ASSESSMENT OF QUALITY AND RISK OF BIAS
The identified randomized, controlled trials were considered as suitable for revision if they matched the initial inclusion criteria. Quality was assessed following the methodology proposed in the Cochrane handbook for systematic review of interventions, version 5.1.0 14. Each identified study was independently evaluated for inclusion by two reviewers who were blinded to authors, institutions, and journals during the selection process. When several papers from the same study were found, the publication with higher methodological quality was selected. Any disagreement between the reviewers was resolved by consensus discussions with the other members of the team.
RESULTS
ELIGIBLE STUDIES
After the selection process, six publications with a total of 446 patients were included in the review 15) (16) (17) (18) (19) (20. One study presented results in two different publications, and it was treated as one single study 7) (8. The selection process is presented in figure 1, and the characteristics of these studies are summarized in table I.
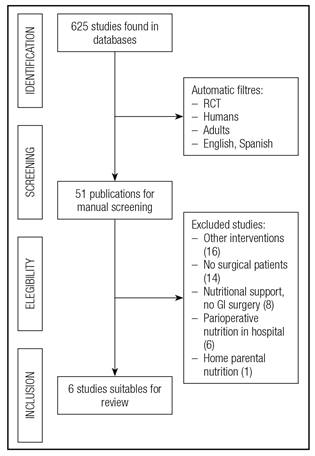
Figure 1 Flow char of the study selection process (RCT: Randomized, controlled trials; GI: Gastrointestinal).

CHARACTERISTICS OF THE SELECTED STUDIES
All but one of the studies were developed in a single center: the study by Smedley et al. took place in three different hospitals in the UK 18. Only two trials provided nutritional support exclusively after hospitalization 15) (16) (19, while the others offered perioperative nutritional support to any of the groups. The trial by Keele et al. included four arms of intervention: no nutritional support, nutritional support in the postoperative period and at discharge, nutritional support only in the postoperative period, and nutritional support only at discharge 14. Patients recruited in the trial by Beattie et al. received ONS during the postoperative period and at home, or the usual care (which was not described in the text) 17. The study by Smedley et al. also included four arms: usual care (progressive oral diet), preoperative ONS, perioperative ONS and at discharge, and postoperative ONS and at discharge 18. In the study by Carey et al., usual care was compared with nutritional support, both provided at discharge. The usual care included dietary advice provided by the ward dietitian in a single session of 45 minutes, with written information and recommendations about the use of ONS. The intervention group included regular phone calls from a dietitian, face-to-face interviews, and ONS or enteral nutrition, if necessary 19. The duration of the follow-up ranged between four and 24 weeks.
In four trials, specific commercially available ONS were provided to patients, in three of them a hypercaloric standard ONS (Fortisip(tm), NV Nutricia, Zoetermeer, The Netherlands; Ensure Plus(tm), Abbott Laboratories, Lake Forest, USA) was provided, and in the remaining, a combination of low-fat and non-fat, high-protein ONS (Top up special(tm) and Plus one(tm), Ferrosan, Søborg, Denmark) was provided 14) (15) (16) (17) (18).
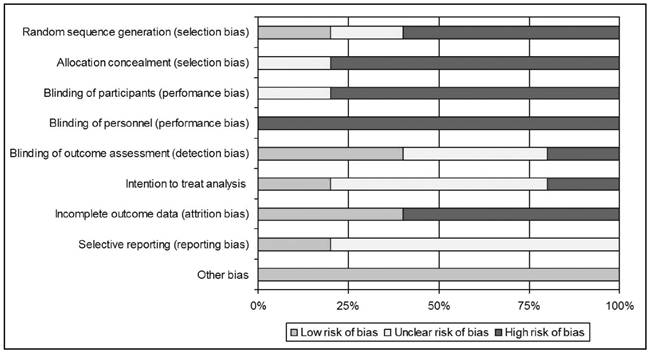
The risk of bias is summarized in table II and figure 2. For randomization, two studies used sealed envelopes 16) (18, one used a computer-generated table of random numbers 17, and another, a randomization table 19. In the other trials the method for randomization was not specified in the text. None of the studies blinded personnel and participants, and only two studies blinded the outcomes assessment 17) (18. Only in the study by Carey et al. were data analyzed in an intention-to-treat mode 19.

PATIENT CHARACTERISTICS
The number of patients recruited for each trial ranged from 27 to 179, with an age of 53 to 66 years. Most patients were male (257/461). Three studies included patients who underwent programmed major gastrointestinal surgery 6) (9) (10, the study developed by Jensen et al. included emergency surgery 7) (8, and another study did not report this characteristic 11. All of the studies except one (Jensen et al.) reported the nutritional status of the patients, although it was evaluated with different methods. The study by Keele et al. found 14% of patients with severe nutritional risk according to the Nutritional Risk Index, Beattie et al. reported 3% of patients with low body mass index, and Carey et al. found malnutrition in 62.9% using the Subjective Global Assessment. In the study by Smedley et al., 34% of patients had nutritional risk, but the method used to detect it was not described.
EFFECTS ON ENERGY AND PROTEIN INTAKE
Oral intake was measured in all but one study (Beattie et al.). Three of these studies found a positive effect of the intervention on energy or protein intake. In the study by Keele et al., one month after discharge the patients who received ONS in the postoperative period and at discharge ate more calories than those receiving only postoperative ONS or no nutritional support 14. Two months after hospital discharge, ONS at discharge was related to higher energy intake than nutritional support limited to hospitalization. There were no differences in protein intake 14.
Jensen et al. described higher energy (57.8 kcal/kg muscle mass vs 47.3 kcal/kg muscle mass, p = 0.022) and protein (1.5 g/kg vs 1 g/kg, p = 0.002) intake in the intervention group 15. A similar result was found by Smedley et al.: patients with nutritional support ate 2,133 kcal and the control group, 1,791 kcal (p < 0.05) 19. Nevertheless, Carey et al. did not find significant differences in energy (control 1,956 kcal vs intervention 1,723) or protein intake (control 91 g vs intervention 69 g) 19.

EFFECTS ON WEIGHT
Weight was assessed in all of the studies, and three of them found positive results with nutritional support 15) (17) (18. Keele et al. did not detect significant differences in weight among the four arms of the trial 14. The other trial with four different arms detected a better weight maintenance and recovery in subjects who received ONS pre and postoperatively compared with the other groups 18. At the end of the study by Jensen et al., weight gain was significantly better with nutritional support (+4.6 kg vs +1.9 kg, p = 0.014), and in the trial by Beattie et al. the intervention diminished weight loss (-1.5 kg vs -5.9 kg, p < 0.001) 15) (17. The most recent publication found no differences between groups (-0.9 kg vs -3.2 kg, p > 0.05) 19.
EFFECTS ON ANTHROPOMETRY AND BODY COMPOSITION
All studies determined anthropometry, but different methodologies were followed. Keele et al. measured mid-arm circumference (MAC), mid-arm muscle circumference (MAMC), and triceps skinfold thickness (TST), but without differences among groups 14. A similar methodology was used by Beattie et al., with favorable results associated with intervention in MAC (-0.42 cm vs -1.28 cm, p < 0.001) and TST (-0.16 mm vs -0.82 mm, p < 0.001), and by Smedley, without finding any beneficial result 17) (18. Carey et al. described similar changes in arm muscle area among patients allocated to the intervention (+0.4 cm2) or control (+0.3 cm2). Nutritional intervention produced a better gain of muscle mass (+3.1 kg vs +1.7 kg, p =0.014), measured with dual-energy X-ray absorptiometry (DXA) in the study by Jensen et al. 15.
EFFECTS ON MUSCLE FUNCTION
The effects of nutritional support on body function were assessed in the five studies. Grip strength was the most common method in the studies, but only the study by Beattie et al. found a positive result 14) (16) (17) (19. Those patients randomized to nutritional support lost less muscle strength than controls (-0.82 kg/m2 vs -1.93 kg/m2, respectively; p < 0.001). Jensen et al. measured expiratory forced volume and a fatigue score without finding benefits related to nutritional supplementation 16. A visual analogue scale of fatigue was used by Smedley et al., and there were no favorable results from the intervention 18.
EFFECTS ON QUALITY OF LIFE
Quality of life was evaluated in four studies 16) (17) (18) 19). In two cases more than a single questionnaire was used 16) (18. Two studies used the SF-36 17) (18, and the General Well Being and Quality of Life 16, EuroQOL 18, and EORTC-QLQ30 were used in the others 19. Two of the studies provided numerical results. Nutritional support yielded a significantly better evolution of the physical (+21.1 pts vs +4.1 pts) and mental (+16.0 pts vs +0.9 pts) scores of SF-36 17. There were no significant differences in quality of life measured with EORTC-QLQ30 between the controls and intervention (64% vs 58%, p > 0.05) in the study by Carey et al. 19.
EFFECTS ON CLINICAL OUTCOMES
None of the selected publications studied clinical outcomes, such as mortality or readmission, after hospital discharge. Fewer patients required antibiotic treatment during hospitalization in the group that received nutritional support than in the control group to nutritional support in the trial by Beattie et al. (7/52 vs 15/49, p < 0.05) 17. The global rate of complications was inferior when ONS were provided in the study by Smedley et al. (15/35 vs 34/44, p < 0.05) 18.
COST ANALYSIS
Only one study analyzed the resources consumption 18. The use of ONS tended to reduce costs by 15% per patient episode. The mean cost per patient was £2,289 with ONS before and after surgery, £2,286 with ONS only before surgery, £2,324 with postoperative ONS, and £2,618 in the no-intervention group. These differences were not significant.
DISCUSSION
MAIN FINDINGS
This review analyzed the disposable evidence about the utility of nutritional support in surgical patients when provided after hospitalization. A PICOS strategy was followed and risk of bias systematically assessed for this purpose. The comprehensive search of the literature obtained a very limited number of studies when compared with the extensive research that exists about this issue during hospitalization.
The more consistent result through the different publications was that nutritional support increased energy intake. An increase in protein intake was only described in the study that provided high-protein ONS, but the oral supplements most commonly used in the studies were hypercaloric 15. In addition to this, most trials described a better weight evolution with nutritional intervention that resulted either in more weight gain or in less weight loss during the follow-up. The evolution of weight seemed to improve when the nutritional intervention included hospitalization and home care. The data about changes in body composition were inconsistent, and the intervention did not enhance muscle strength or quality of life. Only the study of Beattie et al. found positive effects on these parameters of the administration of ONS in the postoperative period and at home 17.
The trials included in this systematic review did not consider clinical outcomes after discharge. In the two studies that analyzed complications during hospitalization, nutritional support reduced antibiotic use and the overall complications in the hospital 17) (18. Therefore, the effects of nutritional intervention on readmission, mortality, or other ambulatory outcomes such as infection remain unknown. Finally, the only study that researched the cost-effectiveness of this intervention did not find significant differences in costs with the control group.
Of the included studies, the one by Carey et al. stands out for its complete lack of positive results in any of the measured outcomes 19. This trial stands out for the nutritional care proposed to each group. The usual care provided to the control group consisted of dietary advice and probably included the administration of ONS, whereas the intervention group received more personal and intensive nutritional support. So, the control group probably received a similar nutritional support than intervention groups of the other trials, which can explain the absence of benefits of the provided care.
Two previous meta-analyses have studied if the use of ONS improved outcomes after hospitalization. The first included six trials which recruited mainly elderly patients with an acute disease who were not specifically undergoing surgery. ONS reduced readmissions with an odds ratio of 0.591 (CI 95%, 0.434 to 0.804, p = 0.001), independently of age 21. The second included six trials with patients older than 65 years who received ONS after hospitalization due to a medical disease or orthopedic surgery. The intervention caused a significant improvement in nutritional intake and status, but there were no benefits regarding readmission and mortality 22.
LIMITATIONS OF THE REVIEW
This review highlights the shortcomings of the research that has been carried out until now about the utility of nutritional support in surgical patients beyond their hospital stay. Regardless of the number of studies, the analysis of the methodology pointed out severe limitations in the development of the studies. Most studies have a high risk of bias, especially in the items of blinding. If the concealment of intervention in oral nutrition is in practice impossible, the blinding of collaborators, outcomes assessment, and data analysis has to be guaranteed. Furthermore, an intention-to-treat analysis is almost mandatory in a clinical intervention like nutritional support in which compliance can definitively influence results.
A critical point when analyzing the efficacy of nutritional support is the initial nutritional status of patients. Only one of the studies used a validated tool for nutritional assessment like the Subjective Global Assessment 19. The other trials used unsatisfactory methods to evaluate malnutrition (e.g., BMI, NRI), so the obtained results could be influenced by recruiting well-nourished patients. Regarding the measurement of outcomes, several limitations can be signaled. Weight changes can be masked by intravenous fluid administration and edema, which tend to improve after discharge. The assessment of nutritional status by means of circumference and skinfold thickness measurement is subjected to a high inter and intraobserver variability. Only one study used DXA, a more accurate method, for body composition study.
Finally, it is difficult to separate the effects of nutritional support administered during hospitalization and at discharge, as most studies combined both interventions. The study by Smedley et al., who included four different arms with a relatively large sample size, detected a better evolution of weight when ONS were administered during the complete process. Two studies included nutritional support only at discharge. The study by Jensen et al. detected favorable effects on energy intake, weight, and body composition, and was less affected by risk of bias 15,16. The other study, published by Carey et al., has been previously discussed.
FUTURE RESEARCH
New studies should cover the gaps described in the studies of this review. First of all, it is necessary to correctly identify the nutritional status of the patients at the moment of discharge, as well-nourished patients can hardly benefit from nutritional support. Second, nutritional intervention at discharge has to be integrated with nutritional support during hospitalization, a well-established care supported by evidence and several clinical guidelines. Third, a more comprehensive evaluation of nutritional status should be ensured using well-validated and universally recognized tools.
CONCLUSIONS
The methodological limitations of the studies included in this systematic review prevent us from offering firm recommendations about the utility of nutritional support in surgical patients after hospitalization. Nutritional care can ameliorate energy intake and weight, but there are insufficient data about its efficacy on clinical outcomes and quality of life. New studies with a high-quality design are greatly needed.

