










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Omega-3 fatty acids or n-3 long chained polyunsaturated fatty acids (n-3 LCPUFA) are nutrients mainly found in the diet that could reduce the risk or help in the treatment of cognitive decline. There are three different types of n-3 LCPUFA: α-linolenic acid (ALA), docosahexaenoic acid (DHA) and eicosapentanoic acid (EPA). Of these, DHA and EPA (in lesser proportion) are important components of the neuronal membranes in the brain 1,2,3. These n-3 LCPUFAS have been shown to have a major role from the moment of the fetus formation to the aging process and brain senescence 1,4,5. Brain function, visual development and neural development depend on an adequate n-3 LCPUFA supply 2,6. In fact, a study performed in children yielded beneficial effects from supplementation of n-3 LCPUFA on cognition and motor skills 7.
As humans age, the concentration of n-3 LCPUFAs in the brain decreases, which translates into an increase in the risk of suffering from the negative consequences of neurodegeneration 8,9,10. Moreover, aging is also linked to damage in the neural tissue due to different cellular processes like chronic mild inflammation 11,12, mitochondrial insufficiency 13, oxidative stress 14,15,16 and accumulation of ß-amyloid 17. Recent evidence suggests that n-3 LCPUFAs have a beneficial effect on the prevention of cognitive decline due to different mechanisms such as anti-inflammatory and antioxidant effects and others that slow down or "compensate" neurodegeneration 10.
Even though human aging is a physiological process, it involves the global degeneration of motor and cognitive abilities due to different biological and chemical processes. As humans age the brain shrinks, vasculature gets damaged and neurotransmitters and hormone levels change, which can be globally translated into cognitive decline 18. Deterioration throughout the lifespan due to normal aging is referred to as age related cognitive decline (ARCD) 19. On the other hand, mild cognitive impairment (MCI) is the term used to identify the state of cognitive function prior to dementia, which is different from normal ageing, being it an intermediate stage between the two 20. However, there is no agreement in the field for early detection of MCI 21. As research work on MCI continues to increase, lack of consensus has arisen concerning its identification in a patient and its specific boundaries 22. According to the first key symposium on MCI conducted by the International Working Group on Mild Cognitive Impairment, there are three key criteria for a general detection of MCI: "(i) The person is neither normal nor demented; (ii) there is evidence of cognitive deterioration shown by either objectively measured decline over time and/or subjective report of decline by self-report and/or informant report in conjunction with objective cognitive deficits; and (iii) activities of daily living are preserved and complex instrumental function are either intact or minimally impaired" 22.
A growing population of elder subjects and unhealthy diets are nowadays leading to the increase in the prevalence of different age-related diseases, being cognitive impairment one of the most prevalent ones 23,24,25. Cognitive decline is considered as inevitable, however, its magnitude is highly variable and affected by different pathogenic processes such as hypertension, diabetes and cardiovascular risk factors 26,27,28. Cognition can also be impaired by other different factors such as decreased physical activity, genetic predisposition, metabolic disorders and unhealthy diet 25,27,29,30,31. In this context, the beneficial effect of nutrition on cognitive function is a topic of increasing interest 32. Due to the possible positive effects that n-3 LCPUFAs might exert over cognition, several research work were conducted 33,34,35,36,37 in order to explore its possible therapeutic effects. Several clinical studies have explored the association of omega-3 with cognitive impairment. However, conflicting results have been reported 8, making it difficult for the scientific community to draw a conclusion on this topic. In this sense, the main objective of the present work is to review the evidence on the role of n-3 LCPUFAs on cognitive function in aged adult and elderly populations, and to determine whether they can be used as a preventive/therapeutic strategy for cognitive decline in elder populations. Additionally, we also remark how different factors such as duration periods, different cognitive baseline status in subjects, dosage of n-3 LCPUFAs administration and the presence of other factors might be related to different outcomes.
METHODS
For the elaboration of this systematic review, the standard informative methods corresponding to the PRISMA statement were followed 38. Relevant studies were identified through a search in a scientific database (PubMed). Additional literature searches included the examination of the reference lists of all pertinent/relevant reviews and studies. The studies chosen were published between January 2010 and December 2017. The search strategy was based on the use of terms related to n-3 LCPUFA (Docosahexaenoic acid OR Omega-3 fatty acids OR n-3 polyunsaturated fatty acids OR DHA) and their effect on cognition in aged adults (Cognition OR Memory OR Mild Cognitive Impairment AND Elderly).
Randomized controlled trials (RCTs) on the effect of omega-3 supplementation, including DHA and EPA or a combination of both, on cognition and/or memory outcomes in healthy aged adults with or without MCI were included in this review. Studies were excluded when: a) they only used dietary sources for the intervention; b) participants were not in the age range of 45-80 years old; and c) participants were diagnosed with dementia, Alzheimer's disease, cardiovascular diseases or diabetes, or they suffered from other relevant health conditions that might affect cognitive status. Moreover, studies in animals, in vitro studies and reviews were also excluded. Studies that only considered the effects of multivitamins including n-3 LCPUFA but not their independent effects (e.g., evaluation of the effect of multivitamin supplementation including omega-3 fatty acids without the evaluation of the effect of omega-3 fatty acids alone) and studies that did not specify the dosage of n-3 LCPUFA used in the intervention were excluded.
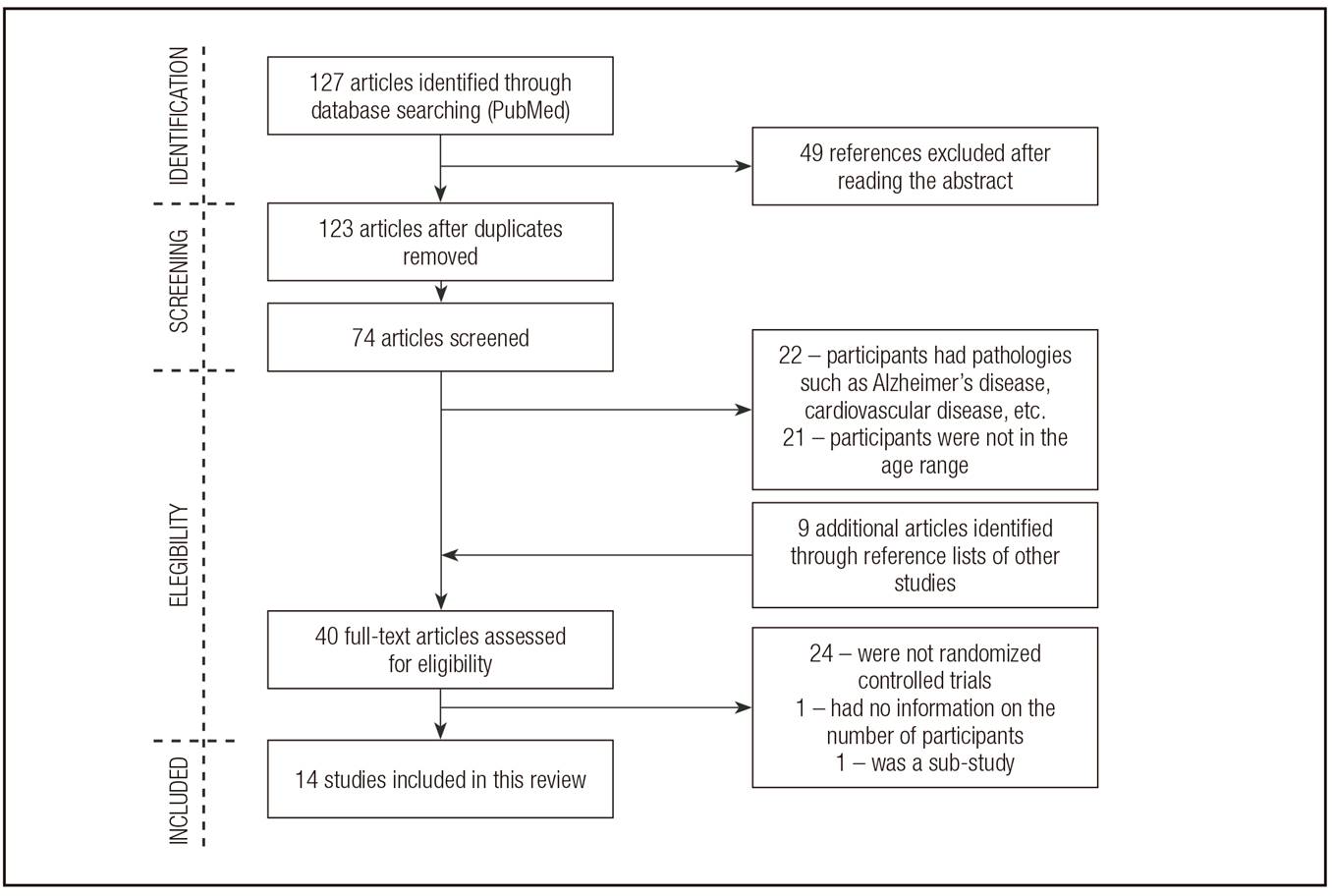
The initial search (which included the following filters: five years, human subjects) yielded 127 references, of which 49 were excluded due to initial screening of titles (Fig. 1). Seventy-four full-text articles were left for further screening. The second screening consisted in the reading of the Abstracts; 22 articles were excluded because participants were diagnosed with health conditions that could affect their cognition such as dementia, cardiovascular diseases, diabetes, recent strokes or head injuries, Alzheimer's disease, etc., and 21 others due to age ranges different from 45-80 years old. Forty full-text articles were then assessed for eligibility; 24 were excluded because they were not RCTs (cohorts, open label extension studies, etc.), and two were also excluded for other reasons (sub-study and not including number of participants). During the full-text review, nine additional articles were included from the reference list of the studies being reviewed. Finally, 14 interventional studies were included in this synthesis of the current systematic review.
RESULTS
The main characteristics of the 14 RCTs included in this work are summarized in Table I. Six studies were conducted in cognitively healthy adults, four in participants with subjective cognitive impairment/complaints, three in participants with MCI and one with participants with cognitive impairment no dementia (CIND) or Alzheimer's disease (AD). This last study was included because it analyzed the effects in both the CIND and the AD participants and because participants with AD are 19 out of 57 participants. The interventions ranged from a time period of one month to 12 months with an average of 5.7 months. Four different types of intervention relating the dosage and type of n-3 LCPUFA used were identified. In relation to the type of omega-3 administration, the majority of the interventions consisted of a combined administration of DHA + EPA. Nine studies administered DHA+EPA in a dose range of 252 to 1,500 mg of DHA and 60 to 1,500 mg of EPA. Three studies administered DHA only, in which 252 mg DHA was the minimum dosage and 2,000 mg DHA was the maximum. One study had two fish oil intervention groups, one group had krill oil and the other one sardine oil. Lastly, there was one study that consisted in the administration of 300 mg DHA + 100 mg EPA + 120 mg arachidonic acid (ARA). All studies were conducted in subjects over 45 years of age. Furthermore, ten studies included less than 90 participants. Most of the RCTs were conducted in men and women except two that included men only subjects. Studies were conducted in different countries, such as the European Union, the United States, Japan and China.
Table I. Main characteristics of the articles included in this review evaluating the effect of omega-3 supplementation on cognitive decline in elderly populations



AD: Alzheimer's disease; ARCD: age related cognitive decline; BOLD: cortical blood oxygen level-dependent activity; CIND: cognitive impairment no dementia; DHA: docosahexaenoic acid; EPA: eicosapentanoic acid; FA: fatty acids; FO: fish oils; GM: grey matter; KO: krill oil; MCI: mild cognitive impairment; PAL: CANTAB paired associate learning; SO: sardine oil.
Moreover, most of the studies did not mention their statistical power. Nonetheless, ten out of 14 achieved significant results in relation to the positive effect that n-3 LCPUFAs exert on cognition. However, four studies lacked significant positive results. From the studies with positive outcomes, improvements in perceptual speed, space imagery, working memory, episodic memory, learning function, immediate visual memory, short term memory, delayed recall capability, executive functions and cognitive processing speed were observed. Furthermore, working memory was the domain of cognition most commonly enhanced between the studies 39,40,41,42.
DISCUSSION
This review identified 14 RCTs studying the effect that omega-3 supplementation exerts over cognition in aged adult and elder populations.
Ten out of fourteen studies showed a positive association between omega-3 supplementation and cognitive decline. Different study factors may account for differences in results between studies such as study duration, number of participants as well as their cognitive baseline status, dosage and type of n-3 LCPUFA used, diet of the participants, APOE-4 genotype, etc.
Exclusion criteria were similar in all studies, thus the subjects studied could be comparable among them. They excluded participants with history or current neuropsychological disease, psychiatric disease, mental illness and previous intake of FOS. Other exclusion factors that were taken into acquaintance in almost all studies were: depression, diabetes, cardiovascular disease, kidney failure, alcohol or drug abuse, intake of multivitamins previous to the study and use of medications that could affect the outcome of the intervention such as angiotensin-converting-enzyme inhibitor. Another factor that added reliability to these studies was that eleven out of 14 studies reported no significant between group differences and the other three reported studying the differences and adjusting them with statistical analyses such as Student's t, Chi-square test and paired t test.
An important factor that might have affected the results is the cognitive baseline status of the participants. Some of the previous studies that have yielded positive results on n-3 LCPUFA supplementation have mentioned that the positive effects could only be observed in subjects with MCI but not in healthy subjects or those with AD 53. However, this review showed no difference in results based on the main three different baseline statuses: healthy, subjective cognitive impairment/complaints and MCI. It is also important to mention that most of the studies used different tools to measure baseline cognitive status in participants, being the Mini Mental State Examination (MMSE) the most used one. This methodologic difference in assessing cognitive status could influence the effect that n-3 LCPUFAs exert over cognition.
Moreover, they used different tools to assess cognitive improvement in the participants. This may also account for different results since some tools may be more or less accurate as well as having different sensitivities for diverse aspects of cognition. Furthermore, it was mentioned in three studies 39,41,46 that a possible factor that might have affected results was proficiency in the tests administered to measure cognitive improvements such as the Basic Cognitive Aptitude Tests (BCAT) and the Swinburne University Computerized Cognitive Assessment Battery. Since tests were administered more than once, participants in both groups could have had the practice effect, showing improvement in cognition without necessarily being it so 39.
A rather novel way to measure cognitive improvement is the near infrared spectroscopy (NIRS), which is a non-invasive neuroimaging technique that measures relative changes in oxyhemoglobin concentration in the superficial cortex in response to a localized neural activity. Both Jackson (2016) 48 and Konagai (2013) 40 used the NIRS to measure cognitive function in their studies. However, they obtained conflicting results which might be attributed to the fact that they used different tasks to activate neural activity.
Moreover, the study lead by Yurko-Mauro (2010) 54 consisting in a supplementation of 900 mg of DHA in healthy participants with ARCD was the first to clinically confirm that DHA significantly improves learning functions and episodic memory. Other studies 39,42,44,49 that consisted in a DHA+EPA intervention corroborate the positive results of n-3 LCPUFA supplementation on cognition, which increases the amount of evidence that omega-3 supplements might be used as a nutritional neuroprotective agent. The mechanisms related to the positive effects of omega-3 on cognition are the following (Fig. 2):

Enhancement of the brain-derived neurotrophic factor (BDNF) levels 55.
Reduction of ARA and its metabolites availability in brain compartments, which contributes to glial and neuronal hyperactivation 55,56.
Increase of the antioxidant defenses: reduction of in vivo oxidant stress by either direct or indirect pathways 55,57.
Increase of phosphatidylserine (PS) concentration in the brain: faster translocation and phosphorylation of protein kinase B (Akt), which increases neuronal survival 58.
Synthesis of neuroprotectin D1 (NPD1): a metabolite of DHA which appears to have multiple neuroprotective functions such as up-regulation of anti-apoptotic and down-regulation of pro-apoptotic mediators that modulate cell death 59.
Promotion of neurogenesis 60 and improvement in the fluidity in synaptic membranes 61.
Increase of a glucose transporter which improves brain glucose transport 15.
Improvement of G-protein coupling involved in signal transduction pathways whose deficiency is associated with cognitive deficits 62.
However, not all studies yielded positive results. There are a number of factors involved in the design and methodology of the studies that could have potentially cofounded the results. One important confounder is the polymorphisms in APOE 63. It has been found that APOE-ε4 genotype influences the way n-3 LCPUFA are metabolized 64,65, specifically in the manner DHA is incorporated into the plasma lipids 66,67. However, the exact effect that APOE-ε4 has over cognition is not clear yet, even though large epidemiological studies 68,69,70 testing the influence DHA supplementation has over cognition reported that the benefits linked to DHA were restricted to subjects that were non-carriers of the APOE-ε4 allele. Although this genotype has been demonstrated to be important in this topic, it was only taken into acquaintance in the study conducted by McNamara et al. (2017) 50 in which it was found that APOE-ε4 genotype did not affect the n-3 LCPUFA metabolism.
Furthermore, diet is another relevant factor which might have affected results. The diet of participants previous to the study is an important confounder since n-3 LCPUFA are more present in some diets than others, which might affect the cognitive status of the subjects. It should also be considered that there is evidence that the effects of n-3 LCPUFAs on cognitive function have a beneficial effect on short term memory only on people deficient in n-3 LCPUFAs 71. Tokuda et al. (2015) 45 mentioned that one limitation of his study was the fact that Japanese population has a high intake of n-3 LCPUFA for which participants of this study might not be comparable with participants of European or American studies. Moreover, McNamara et al. (2017) 50 as well as Boespflug et al. (2016) 49 applied 3-day diet records during the week before enrollement to characterize the background diet of participants. They also applied the same three-day diet records during week 12 and week 24 (final week). Additionally, an omega-3 dietary intake questionnaire 72 was also administered before starting the intervention to identify the habitual intake of omega-3 in their diet. Other studies mentioned the use of Food Frequency Questionaires (FFQs). Yurko-Mauro et al. (2010) 47 made use of the FFQ to minimize the potential confounding effect of a diet high in DHA before the study entry. Participants that had a high intake of 200 mg of DHA per day were excluded.
As well as the diet previous to the study, the diet followed during the intervention period in the study is of major importance 40,50. Konagai et al. (2013) 40 also used the FFQ but with the purpose of measuring the nutrient intake of participants during the study. Their results showed no significant differences between the ingestion of any of the nutrients measured by the FFQ which helped attribute the results of the study on the omega-3 supplementation only. Furthermore, we found that only two studies out of fourteen restricted the n-3 LCPUFA intake so that the changes in cognition could only be attributed to the n-3 LCPUFA oil supplementation and not to the n-3 LCPUFAs consumed from the diet which makes their results more reliable.
Intervention duration is a very important factor to take into acquaintance. Shorter intervention periods might not give enough time to the omega-3 to show significant results on cognition 52. However, interventions of one month 45 and of two months and a half 42 showed significant results. Interestingly, both of these studies had a statistical power ≥ 80%. The RCTs that yielded no results from the intervention all had durations of over two months and a half, which makes the factor duration a less likely confounder factor in the results.
It was also observed that three out of four RCTs with no positive outcome in the intervention had an overall younger age range (≈ 63 years old) of the participants compared to the studies with positive outcomes. It could be inferred that older participants benefit more from this kind of intervention although different studies support the idea that early intervention for prevention of worsening of cognitive decline is more effective than an intervention in older participants that already have an evident cognitive decline 73.
Moreover, an interesting study was the one carried out by Nilsson et al. (2012) 42 in which participants acted as their own control since it was a cross-over study. It revealed that a five-week intervention consisting in daily intake of omega-3 from fish oil improved cognitive function in a healthy population. Since the control and intervention group were the same, it annulled the possibility that between group differences might have been a confounder in the results.
N-3 LCPUFAs effect over cognition have also been assessed in combination with other nutrients relevant to brain function to check for synergic effects that could benefit cognition 48. Two of the reviewed studies tested the effects of a combined supplementation of n-3 LCPUFAs and a multinutrient 46,48, nevertheless, none obtained significant results of the combined omega-3 and multinutrient intervention. Some of the nutrients being used were: ginkgo biloba, vitamin B6, vitamin B12, phosphatidylserine and anthocyanins. Additionally, there was also another study that investigated the effect of omega-3 alone, in combination of blueberry (BB) powder and of BB powder alone 50. Shukitt-Hale et al. (2015) studied BBs and their relation to neurocognitive function in aging which yielded positive effects 74. However, the study from this review obtained positive results in cognition both from the BB intervention and the one from omega-3 but not from the combined intervention. The reason for which the combined intervention lacked effect is unknown, however, McNamara et al. (2017) stated that one consideration could be that daily, long-term supplementation of omega-3 and BB powder may have sabotaged a beneficial outcome 50.
Moreover, fatty acids (FA) were measured in blood to evaluate the changes in n-3 LCPUFAs concentration in blood. Previous scientific studies have reported a positive relationships between high concentrations of circulating omega-3 FA in blood and cognitive decline 75. Nevertheless, these findings, specifically those referring to verbal fluency, appear to be inconsistent 75,76. This might be explained by the different methods used to measure FA in blood given that they reflect different results 77. Red blood cell (RBC) membranes reflect FA intake over the last 120 days, whereas plasma and serum concentrations of FA reflect the intake of a few prior days 78. Also, it is still uncertain whether FA concentration in blood reflects the concentration of FA in tissues of the central nervous system 51. Most of the studies reviewed measured FA concentration in blood in plasma and only four measured it in RBC membranes. These findings might explain why some studies yielded negative results regardless of the increase in FA concentration in plasma since the increase could only be reflecting the few previous days and not a constant long period.
This systematic review has several limitations such as: a) most of the reviewed RCTs had small sample sizes; b) not all RCTs had the same dosage of omega-3 or duration of intervention; c) baseline cognitive status and assessment of cognitive decline was measured differently among studies; and d) almost none of the studies performed the APOE genotyping.
Regarding previous reviews, meta-analysis and community studies 1,54,71,77,79,80,81,82,83 results have been contradictory. For instance, Burckhardt et al. (2016) 81 found no benefit from n-3 LCPUFA supplementation on cognition; however, this review focused on studies conducted in participants with higher degree of dementia and AD. Additionally, Mazereeuw et al. (2012) 53 suggested a positive effect of n-3 LCPUFAs on the cognitive domains of attention and processing speed on a number of subjects with MCI but not on those with AD. In accordance with the previously mentioned, the results from the only study in this review that included participants with AD were also negative, indicating no effect of n-3 LCPUFA supplementation on cognition. However, most of the conducted reviews on this topic yielded similar results: a possible beneficial effect of n-3 LCPUFA supplementation on cognitive decline 54,83. Nonetheless, just as the studies included in this review, all of them agree on the fact that more RCTs with longer duration and bigger sample size should be conducted for further understanding of the effect of n-3 LCPUFAs on cognition in order to determine an effective and safe therapeutic dosage for cognitive decline.
CONCLUSION
This systematic review concludes that omega-3 supplementation might have a positive effect on cognition. Thus, n-3 LCPUFAs could be used as a preventive tool for cognitive decline in aged or elder adults or as a therapeutic measure in subjects with cognitive decline. Further studies containing detailed information in regard to duration of the trial, dosage of n-3 LCPUFAs in the supplementation, presence of APOE-ε4 carriers, baseline conditions of the participants, etc., are needed for more accurate information upon the effect of n-3 LCPUFAs supplementation in cognition in elder populations.

