










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
There is scientific evidence for the superiority of human milk over human milk substitutes (HMS). Breastfeeding (BF) prevents infectious diseases, reduces the probability of morbidity and mortality in infants, and prevents future non-communicable diseases such as hypertension, diabetes mellitus, and obesity (1). Additionally, BF has a favorable effect on the mother's health (2). Moreover, it is economically beneficial to the family (3), the institutions that encourage BF (4,5), and the health system (6). Another benefit is that BF may contribute to environmental sustainability and food security (7).
However, several factors are predictive of BF abandonment, such as working while breastfeeding and low milk production perception (8,9). The availability of a space at the workplace for breast pumping during the workday could help mothers to maintain milk production, encourage breastfeeding for a longer duration, and facilitate role combination as mothers and employees or professionals. In countries such as Taiwan, Thailand, and the United States, the availability of an adequate space for BF at the workplace has proven to be effective in increasing the practice of BF, and was associated with a BF duration of at least six months in working mothers (10-12).
Mexico began providing human milk extraction spaces at workplaces in 2014 (13); however, there is no scientific evidence for their utilization and association with breastfeeding practice and duration. The objective of this study was to compare the frequency and duration of breastfeeding among working mothers based on the presence of lactation rooms at their workplaces in the city of Guadalajara, Mexico.
MATERIAL AND METHODS
STUDY DESIGN
In an analytical cross-sectional study and with sampling carried out at concentration sites we surveyed mothers who worked at institutions with more than 251 employees. These institutions belonged to the three predominant economic units in Guadalajara, Mexico, according to the Directory of Economic Units interactive tool (14). The economic units included manufacturing, governmental, and health services/social assistance units. Two types of economic units were eliminated: 1) business support services unit, which was eliminated because mother location was confidential; and 2) the wholesale trade unit, which was eliminated because either they had no female staff, the children of the female staff were older than three years, or the institution did not want to participate.
The sampling system was not probabilistic at the site of concentration. Finally, 25 institutions were included, of which 12 had lactation rooms. We created a directory of the selected institutions with their identification data. The corresponding persons at the selected institutions were contacted by telephone. They subsequently received emails containing information about the study (nature of the study, risks, benefits, and data confidentiality) and an invitation to participate.
The institutions that agreed to participate scheduled an appointment with the corresponding authority to briefly explain the project, answer questions, deliver the official document for participation, and request the support of the Human Resources department. In that department, a list of women who had infants between the ages of six and 35 months was requested; mothers were located and invited to participate. Each mother who agreed to participate signed the written informed consent form before the face-to-face questionnaire was administered. Additionally, the person in charge of the Human Resources department answered questions on the registration sheet about the institution's characteristics.
PARTICIPANTS
We enrolled healthy mothers in the study. Mothers who had children aged between 6 and 35 months, those who had term pregnancies, and those whose children were born with adequate weight for the gestational age were included in the study. On the other hand, mothers who had physical or mental conditions that prevented them from breastfeeding, those who had multiple pregnancies, and those whose newborns had genetic, congenital, or chronic conditions that prevented them from sucking correctly, were excluded from the study. Additionally, mothers with incomplete information were excluded. The sample size was calculated with a significance level of 0.05, β-value of 0.20. This resulted in a sample size of 140. We included 30 % more participants to account for lost participants, therefore, we enrolled in 182 working mothers.
Twenty-six questionnaires were eliminated because either the mothers were working elsewhere, the mothers were not working when they started breastfeeding, or their working activities did not allow them to complete the survey. The participants were surveyed between April and July 2018, with the support of three researchers trained to complete the questionnaire.
QUESTIONNAIRE
We used an ad hoc questionnaire composed of 127 items. We asked questions about the duration of BF, exclusive breastfeeding (EBF), partial breastfeeding (PBF), predominant breastfeeding (PrBF), and HMS. We also asked questions about the mother's characteristics and identification data, the institutions' traits, and the type of infant feeding. The socioeconomic status of mothers was obtained using a survey developed by the Mexican Association of Market Research Agencies (15).
Partial breastfeeding was divided into three categories according to the maternal perception of human milk feeding (either directly from the breast or extracted), and compared to HMS utilization—when working mothers feed their infants with more human milk than HMS (more than half BF), less human milk than HMS (less than half BF), or to a similar proportion (half-and-half BF and HMS). In addition, to evaluate the presence of a lactation room at the workplace, we also evaluated their utilization, so we asked the mothers who had lactation rooms if they used it for subgroup analysis.
STATISTICAL ANALYSIS
We reported quantitative data as mean and standard deviation if they showed a normal distribution, or as medians and 25th to 75th percentiles (Shapiro–Wilk test). Comparisons between mothers with and without a lactation room were performed either with the t-test for independent samples, if data were normally distributed, or with the Mann-Whitney U-test for non-normal data. Comparisons between mothers who used the lactation room, women who did not use it, and women who did not have a lactation room were performed using the Kruskal-Wallis test and Dunn's post-hoc test.
For qualitative data, results are reported as frequencies and percentages. We used Fisher's exact test to compare frequencies between mothers with and without a lactation room. The X2 test was performed to compare frequencies between mothers that used, did not use, or did not have a lactation room at the workplace. We used multiple t-tests for proportions, with Bonferroni adjustment as a post-hoc test. Additionally, we analyzed the association between the existence of a lactation room at the workplace (predictive variable) and both duration of BF, EBF, PBF, and HMS (dependent variable), and type of BF at sixth month (EBF vs. PBF) using binomial logistic regression (odds ratios [OR] and 95 % confidence intervals [95 % CI]). We performed the data analysis with IBM's SPSS software version 25.0 (IBM Corp., Armonk, NY, USA), and the graphs were plotted with GraphPad Prism, version 7.05 (GraphPad Software Inc., La Jolla, CA, USA).
ETHICAL CONSIDERATIONS
This study adhered to the guidelines of the Declaration of Helsinki, as amended at the 64th Annual Assembly organized by the World Medical Association (2013). The protocol was approved by the Research, Ethics in Research, and Biosafety Committees of the University Health Sciences Center, University of Guadalajara (No. CI-05918).
RESULTS
INSTITUTION CHARACTERISTICS
There were participating 19 public and six private institutions. Ten public participating institutions and two private participating institutions had a lactation room. The most common economic unit was the government unit (15/25; 60 %). Most of the surveyed women (99/158; 62.7 %) worked in a government unit, and most of the government units (8/12; 66.7 %) had lactation rooms (Table I).
Table I. Participating institutions and women
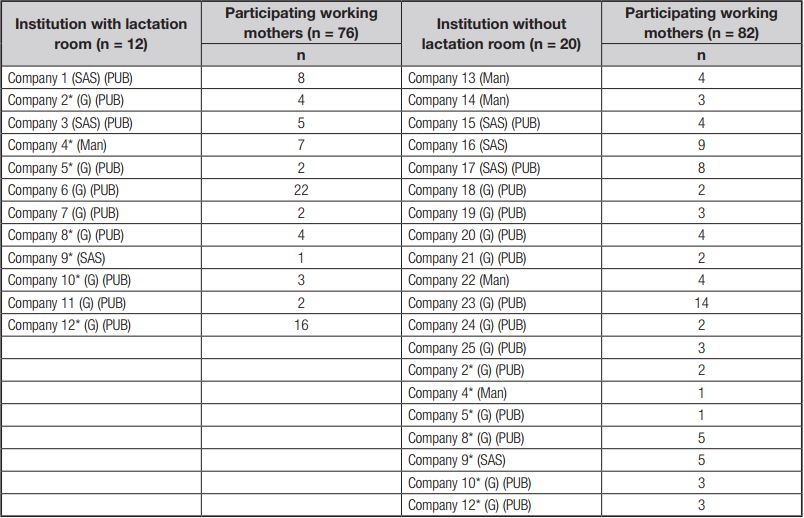
Some working women at the same institution, during their lactation period, did not have a lactation room because the institution had not yet implemented one; G: Government; SAS: health and social assistance services; PUB: public sector; Man: manufacturing.
MOTHERS' CHARACTERISTICS
We analyzed data from 158 mothers with complete data; 76 had a lactation room at the workplace, and 82 did not have this resource. Maternal age ranged from 21 to 46 years; women with a lactation room at the workplace were significantly older, had heavier pre-gestational weight, and had a higher BMI than those without a lactation room. The proportion of infants by age group and mother's education did not differ significantly between the groups. There were similar results for the categories of socioeconomic level, except for the medium-low level and lower level; this category had significantly fewer working mothers with lactation room vs. mothers without it. There was a significantly lower proportion of single working mothers and a higher number of married working mothers with lactation rooms than of those without lactation rooms. The percentages of working mothers, according to economic activity, except for the governmental unit, were similar. A significantly higher proportion of working mothers with a lactation room was working in a governmental unit (Table II).
Table II. Working mothers' characteristics based on the presence of a lactation room at the workplace (n = 158)

a Data expressed as mean ± standard deviation; bData expressed as median (25th-75th percentiles); cn = 72; dn = 81; eData expressed as frequency (percentage); fCategories according to the Mexican Association of Market Research Agencies (AMAI).
Three of the 12 institutions continuously educated mothers on BF, and 6/12 institutions had personnel in charge of the lactation room (4/6 personnel were trained in BF). No institution received external advice on BF. Eight of the 12 institutions promoted the use of the lactation room by employing at least one institutional resource (printed, electronic, or invitation of personnel). The remaining four did not use any institutional resources. Eight of the 12 institutions had not institutional promotion; the diffusion of the area was person-to-person. Only one mother reported not knowing about the existence of a lactation room at her workplace.
LACTATION ROOM CHARACTERISTICS
Four of the 12 institutions had an always-open lactation room, 7/12 required the mothers to request a key to use it, and 1/12 had an established schedule. One of the rooms did not have personnel in charge during the afternoon work shift and remained closed to mothers during these working hours. Some lactation rooms were not adequately equipped, according to the breastfeeding guide at the workplace (16). Eleven out of 12 lactation rooms had refrigeration equipment, 6/12 had a sink, and 4/12 offered breast pumps, mostly manual. Two lactation rooms were difficult to clean following milk spillage because one had a carpet on the floor, and the other room had a cloth armchair.
Of the 76 mothers with a lactation room, 41 used it, and 35 did not. The most common reasons for using it were that the rooms were comfortable (15/41, 36.7 %), convenient and private (14/41, 34.1 %), and hygienic (10/41, 24.4 %). On the other hand, the most common reasons for not using the lactation rooms were that they had decided to stop breastfeeding (8/35, 22.9 %), they had extracted the milk at home or in the office (7/35, 20.0 %), they did not have enough time (5/35, 14.3 %), and the lactation room was closed (4/35, 11.4 %).
Most mothers continued breastfeeding when they returned to their jobs after maternity leave (122/158, 77.2 %). Among these mothers, 64/76 had a lactation room, and 58/82 did not. On the other hand, 12 mothers with a lactation room and 24 without this resource abandoned BF when they returned to work. Notably, all the mothers that stopped BF among the mothers with a lactation room reported that they were not using it.
FEEDING DURATION
All mothers reported that they were initially breastfeeding, but feeding duration differed depending on whether they had a lactation room at the workplace or not. BF and EBF lasted significantly longer among mothers with a lactation room. The length of HMS utilization was significantly shorter among mothers with a lactation room. PBF was not significantly different between groups (Fig. 1). When we performed a sub-analysis, we found that mothers who used a lactation room had significantly longer BF and EBF duration and shorter HMS utilization period than those who did not use a lactation room or those without a lactation room. For these three feeding types (BF, EBF, and HMS), mothers that did not use a lactation room, and those without a lactation room had similar results. PBF duration showed no significant differences between groups (Fig. 1B).
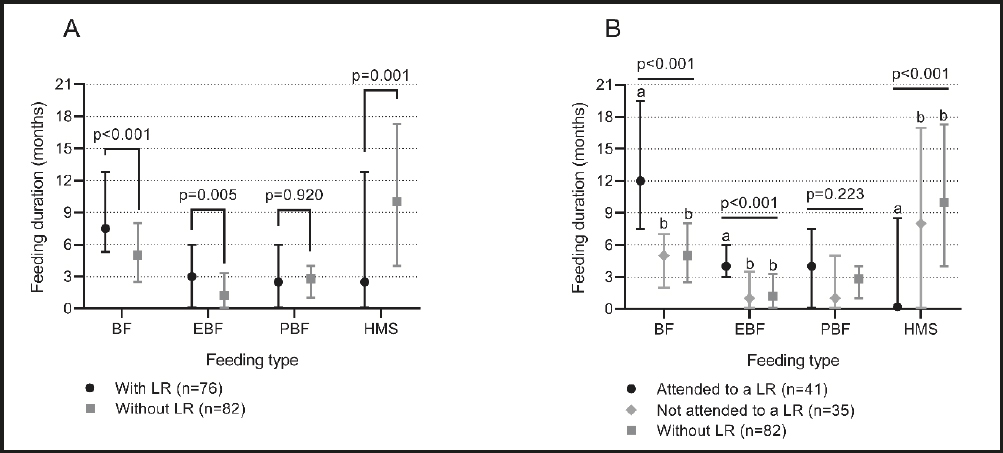
Figure 1. Feeding type duration depending on: a) the existence of a lactation room at the workplace, or b) the existence and utilization of a lactation room at the workplace. Data are expressed as median and 25th-75th percentiles. The p-values were calculated using the Mann-Whitney U-test (A) or Kruskal-Wallis test (B). Different lowercase letters within feeding types denote significant differences (p < 0.05, Dunn's test). BF: breastfeeding; EBF: exclusive breastfeeding; HMS: human milk substitutes; LR: lactation room; PBF: partial breastfeeding.
When the BF duration was categorized (< 6 vs. ≥ 6 and < 12 vs. ≥ 12 months), we found that mothers with a lactation room were about three times and two and half times more likely to BF for ≥ 6 and ≥ 12 months, respectively, compared to mothers without a lactation room. It was more likely to reach the EBF recommendation for six months with a lactation room; likewise, to offer PBF for more than six months. On the other hand, mothers were more likely to feed their infants with HMS for less than six months when they had a lactation room. Similarly, mothers with a lactation room were about three times more likely to feed their infants with EBF (instead of PBF) than those without a lactation room (Table III).
Table III. Frequency of feeding type duration based on the presence of a lactation room at the workplace (n = 158)

BF: breast feeding; EBF: exclusive breast feeding; PBF: partial breastfeeding; HMS: human milk substitutes; OR: odds ratio; CI: confidence interval. ap-value obtained from Fisher's exact test; bTested category to calculate OR and 95 % CI; OR for the selected category when there was a lactation room at the workplace; cn = 138 (66 with lactation room vs 72 without lactation room), excluding 15 participants that reported HMS during the sixth month and 5 with predominant BF.
We compared the use of human milk vs. HMS utilization in mothers who provided PBF. There was a significantly higher percentage of working mothers who preferred breastfed to the use of HMS (more than half of the mothers in the category), when they had a lactation room and used (Fig. 2). One hundred and nineteen participants were included in this analysis because 39 (24.7 %) of them reported that they never provided PBF.
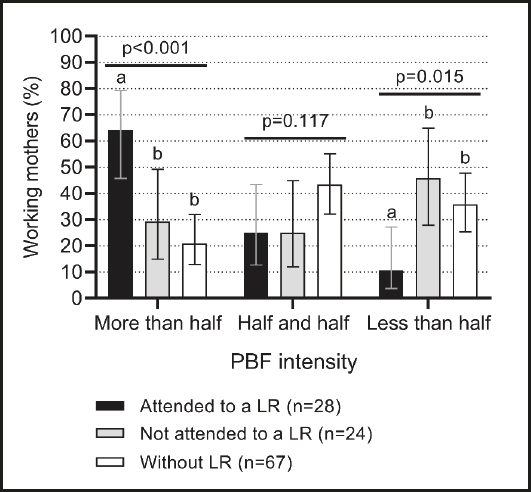
Figure 2. Partial breastfeeding (PBF) intensity in working mothers depends on the existence of a lactation room (LR) at the workplace and its utilization (n = 119). Data are expressed as percentage and 95 % confidence intervals of working mothers within each PBF intensity category. Categories represent the mothers' perceived proportion of human milk vs. HMS utilization: more than half: when working mothers feed their infants with more human milk than HMS; less than half: when working mothers feed their infants with less human milk than HMS; half and half: when working mothers feed their infants with similar proportions. The p-values were calculated using the X2 test. Different letters denote significant differences (p < 0.05) between PBF intensity categories (multiple t-tests for proportions with Bonferroni correction).
DISCUSSION
The results obtained emphasize the need to provide lactation rooms at the workplace to enable mothers to achieve the recommended EBF for six months and BF duration above six months and even 12 months. This could be because mothers can empty their breasts and maintain their breast milk supply (17). Similarly, a lactation room might help deal with the common barriers to BF when returning to work (18,19). In a study conducted in Taiwan, the authors observed a similar result. The availability of a lactation room was a predictor of breastfeeding for more than six months (10). This reduced the health risks of the mother and infant (1,2), and reduced cost for society and institutions that support breastfeeding (4 5-6). Additionally, some lactation rooms provided either a manual or electric extractor, which facilitates and optimizes extraction (20).
In addition to the implementation of lactation rooms, mothers should be encouraged to use these rooms for better results of BF duration and frequency. In the present study, we observed a longer BF duration among mothers who used the lactation room compared to those who had the resource and did not use it, and those who did not have a lactation room.
Significantly predominated women who worked in institutions of governmental economic activity and the public sector that had lactation room. On the contrary, there were more women who worked in private institutions that did not have a lactation worker (p = 0.01). This finding is similar to that of a study in Pakistan, which reported that breastfeeding support was higher in public and multinational institutions (21). Only three institutions had an internal breastfeeding support policy. Two of them were public hospital institutions and the other was the Secretary of Health that regulates the previous two. These institutions were represented by 15 women (9.5 % of the total sample and 19.8 % of the sample of women with lactation rooms).
It is important to convince managers of the benefits of having a lactation room not only for the mother and her infant but also for the company. The institution itself benefits because staff loss or turnover decreases, absences are reduced, the mother returns early from her maternity leave, productivity is increased, and the corporate image is improved (3 4-5).
It is important to highlight that the PBF duration did not differ according to the presence or use of a lactation room. Nonetheless, due to the analysis of PBF intensity, we demonstrated that the presence and utilization of a lactation room promote human milk feeding over the use of HMS. Additionally, previous studies suggest that both EBF and PBF are preventive factors for child overweight and allergies, while PBF tends to be less protective than EBF. It remains to be determined whether the categorization of PBF intensity would yield different results (22,23). Therefore, when assessing PBF, we recommend evaluating its intensity to deepen in the analysis.
To our knowledge, this is one of the few studies in Mexico (24) to show that mothers who have a lactation room at their workplace report more than six months of BF, higher adherence to EBF, and shorter duration of HMS use. We know that other factors may influence the practice of BF, regardless of whether mothers have a lactation room at their workplace or not (25). Therefore, future studies should analyze the effect of such variables on the presence of a lactation room to design interventions and political strategies to promote variables associated with extended BF among working mothers.
One of the most important limitations of this study, due to reporting and memory bias, is that infant feeding was evaluated retrospectively. However, a retrospective assessment was necessary because mother-infant dyads required time of exposure to the lactation room. The duration of the BF was measured, and mothers were asked if they achieved EBF for six months. Another limitation is that most of the mothers worked in governmental (and public) institutions. Therefore, results might no represent the feeding type in mothers who work in private institutions and other public institutions.
Access to institutions was difficult. More than half of the initially selected institutions did not want to participate. Some of the reasons (aside from the exclusion criteria) were the existence of bureaucratic procedures, the lack of personnel to whom the participation request could be sent, and the existence of internal regulation that restricts access by external people. Another obstacle was that most of the institutions did not have a lactation room, although it is a requirement by law in Mexico (13).
We suggested ways to improve and promote the use of lactation rooms in other institutions. These operation and equipment characteristics have been studied in other countries (26). These results should be considered in the legal framework along with industry concerns (27) to increase the availability of lactation rooms at the workplace to guarantee the working mothers' right to continue BF.
CONCLUSION
The presence of a lactation room at the workplace was associated with more extended BF and EBF, and shorter HMS duration in working mothers. However, having a lactation room but not using it resulted in shorter BF and EBF duration, and higher dependence on HMS, similarly to not having a lactation room.

