










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkIntroduction
Traditionally, experts have studied the psychological factors that influence obese population’s eating behaviour. Specifically, the most important factors for this study are food restriction, food addiction or emotional eating, which are described below.
Food restriction was defined by Herman and Maherck (1975). However, Lauzon-Guillain et al. (2006) carried out an important research that we used as a theoretical basis for the present paper. These authors concluded that food restriction is used as an effective strategy to avoid fat accumulation, but it may lead to a long-term body weight gain in both obese and non-obese populations. However, it is a very controversial subject. Some researchers found no clear link between lower development of obesity and food restriction (Lawson et al., 1995; Lindroos et al., 1997), while other authors defend a clear link (Beiseigel & Nickols-Richardson, 2004; Lluch, Herbeth, Méjean & Siest, 2000) or suggest that this link may be reverse (Boschi, Iorio, Margiotta, D'Orsi & Falconi, 2001).
In some of the above-mentioned studies (Lawson et al., 1995; Lindroos et al., 1997), the disinhibition factor in eating behaviour was also studied. According to these authors, the uncontrolled food consumption can be associated with obese population (Meule, 2011), being physiological factors one of the hypotheses supporting these facts (Volkow et al., 2008). However, it is not an exclusive behaviour of obese population (Pelchat, 2009), but population with normal weight can also eat too much uncontrollably even if they do not get fat. In line with this hypothesis, Lopez-Morales and Garcés de los Fayos (2012) analysed the reason why an individual can eat too much without gaining weight. From a multidisciplinary perspective, these authors explained that obesity can take place through interaction of energy intake with other factors such as energy expenditure, homeostatic mechanism, and genetic vulnerability. However, it is possible that an individual can increase energy intake (eating excessively) and, at the same time, increase energy expenditure by practicing physical activity. Finally, we cannot forget the influence of genetic factors.
Another area that has been studied refers to emotional eating. This concept is defined as food consumption seeking relief for negative emotions. According to classical theory, non-obese people tend to reduce their food consumption in response to negative emotions (Herman & Polivy, 1984; Schachter, Goldman & Gordon, 1968) due to the physiological suppression that occurs (Herman, Polivy, Lank & Heatherton, 1987). However, data obtained in numerous research are contrary. Macht (2008) stated that only a small part of non-obese population reduces food consumption, while most increases consumption. In line with these data, reward deficiency theory (Blum, Liu, Shriner & Gold, 2011) correlates conducting behaviours with recovery of optimal reward levels in specific stress situations. This hypothesis could be applied to individuals consuming food to reduce a negative emotion. On the other hand, the five-way theory establishes the connection between emotions and eating behaviour (Macht, 2008). According to the author, emotion intensity can vary an individual’s diet: high intensity emotions would cause a reduction in food consumption, and moderate emotions would increase it. Likewise, several authors propose that the increase in the desire to eat in a previous restriction situation may be due to deterioration of cognitive control (Boon, Stroebe, Schut & Jansen, 1998; Lattimore & Maxwell, 2004; Wallis & Hetherington, 2004) or negative emotions themselves (Gibson & Green, 2002; Macht & Mueller, 2007).
In accordance with the ideas explained in the previous studies, we can highlight that non-obese population presents different eating behaviours. And even some individuals can present pathological behaviours such as uncontrolled food consumption (Pelchat, 2009). In addition, their eating behaviour may be influenced by psychological factors that have typically been related to obesity, such as food restriction, food addiction or emotional eating. These factors may modify perception of appetite by increasing and/or reducing food consumption (Blum, Liu, Shriner & Gold, 2011; Macht, 2008).
On the other hand, in addition to the connection that the previous psychological factors have with food behaviour, personality and coping style can play a mediating role in food behaviour. Personality features can both facilitate food abuse and prevent food consumption through restriction. Keller and Siegrist (2015) conclude that the underlying personality feature can vary both consumption and type of food consumed. Neurotic and emotionally unstable individuals tend to consume sweet, salty and high-calorie foods. In accordance with these authors, Bollen and Wojciechowski (2004) and MacLaren and Best (2009) notice that neuroticism feature is related to eating disorders both in anorexia nervosa (Bulik et al., 2006) and in bulimia nervosa (Mueller et al., 2010). However, it does not happen with scrupulosity feature, for which there are different theories. While Heaven, Mulligan, Merrilees, Woods and Fairooz (2001) defended the fundamental role of scrupulosity in the development of eating disorders, Keller and Siegrist (2015) emphasized its protective role. These authors observed that high levels of scrupulosity are related to low consumption of sweets and sugary drinks.
On the other hand, overfeeding can also be related to a coping style focused in emotion (Koff & Sangani, 1997) and in avoidance (Lee, Greening & Stoppelbein, 2007). In most cases, individuals with an avoidant coping style show metabolic diseases such as insulin resistance, metabolic syndrome, and obesity. This may indicate the existence of a connection between diseases and coping style (Boersma, Scheurink, Wielinga, Steimer & Benthem, 2009; Boersma, Benthem, van Dijk & Scheurink, 2011). In line with the above-mentioned psychological factors and their relation with food behaviour, Benard et al. (2017) highlights the importance of impulsivity in the development of obesity. These authors explain the relation of impulsivity with the process of choosing food, so that an impulsive individual could tend to overeat and choose sweet and high-fat foods.
In accordance with Stoeckel et al. (2017) proposing a psychological model of appetite self-regulation, Lopez-Morales and Garcés de los Fayos (2012) raise the concept of Edorexia as a psychological problem characterized by a perception of constant, daily and uncontrollable appetite. Based on other research on psychological factors influencing food consumption, excessive desire to eat is related to food dependence (Avena & Rada, 2012; Meule, 2011), anxiety and stress (Stice, Spoor, Bohon, Veldhuizen & Small, 2008), and depression (Jun & Choi, 2014), i.e. the above factors can be related to an increase in uncontrollable appetite. Edorexia Syndrome integrates this excessive and uncontrollable appetite, and hypothesizes that this appetite is the main precursor of excessive and inadequate eating behaviour. Besides, these authors confirm that psychological factors may explain relapses into nutritional treatments or lack of control in food consumption.
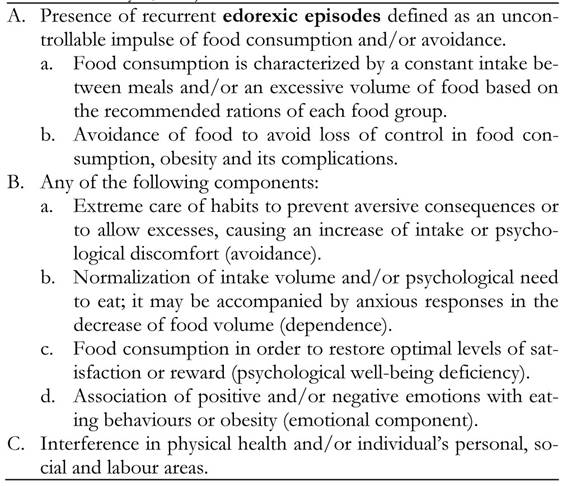
Unlike other studies that analyse psychological factors separately, they integrate them, as the proposed diagnostic criteria show (Table 1). This stance gives rise to a set of inseparable and closely related symptoms. The data show that individuals may eat too much due to dependence and, at the same time, express other behaviours. These include food consumption to restore reward levels, food restriction or fear of gaining weight. Unlike obesity, this set of symptoms can also occur in non-obese population with the same psychosocial alterations. It is also important not to mistake it for other Eating Disorders; Edorexia Syndrome mainly differs from other psychological problems because it does not include purges or binges. For this reason, the present paper has the following main objectives:
To evaluate edorexic population’s eating habits, regarding food abuse and restriction.
To analyse the influence of emotional stability, and the coping style focused on avoidance, on eating behaviour.
Based on the above objectives, the following hypotheses are proposed:
Individuals with Edorexia Syndrome will tend to eat too much and use avoidance strategies such as diets and sport practice.
Edorexia Syndrome will relate to low levels of emotional stability and high levels of coping styles focused on emotions and avoidance.
Method
Participants
The recruitment of participants was made through the psycho-bonus program of the Faculty of Psychology of the University of Murcia, with which students of this centre receive a bonus with academic benefit in a subject of their choice in exchange for participating in a research. 111 subjects volunteered. The inclusion criterion was to have normal weight (18.5 <BMI <24.9), and exclusion criteria were: to have some eating disorder and to practice vigorous physical activity, defined as an intense activity performed every day and for several hours. 36 participants were excluded based on these criteria, so the final sample was 75 subjects with a mean age of 21.32 years (SD = 4.4 years), of which 85.3% were women. The average BMI was 21.28 kg/m2 (SD = 1.59 kg/m2).
The sample was divided into two groups using the Edorexia Syndrome Questionnaire (ESQ). 17 subjects were classified as edorexic, with a mean age of 21.18 years (SD = 2.51 years), and a BMI of 21.91 kg/m2 (SD = 1.79 kg/m2). The rest, 58 subjects, formed the non-edorexic group, with a mean of 21.36 years (SD = 4.83), and a BMI of 21.09 kg/m2 (SD = 1.50). Any group showed significant differences in age and BMI.
Instruments
Sociodemographic questionnaire that also included anthropometric measurements using a measuring rod and a bioimpedance scale, and a record of frequency, type, duration and intensity of physical activity.
Edorexia Syndrome Questionnaire (ESQ). This questionnaire is composed of 32 items with four choice response on a Likert-type scale. It evaluates psychological factors related to eating behaviour, in particular factors related to edorexic episodes, such as food restriction, lack of control in eating and emotional eating. In addition, this questionnaire has an internal consistency of .92, which gives reliability for its use in this research. The cut-off point used for the diagnosis of Edorexia Syndrome is equal to or greater than 11, as established in a previous study. With this criterion, we obtained a sensitivity of 100% and a specificity of 98% of cases.
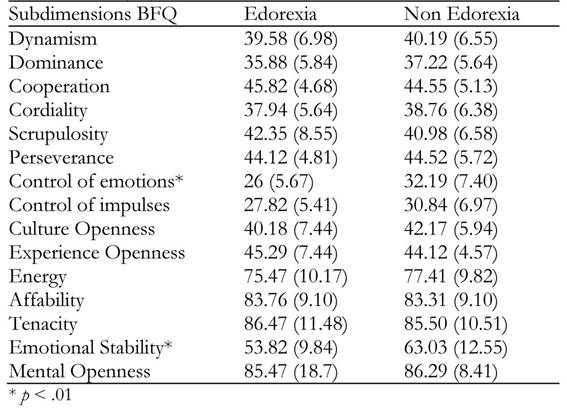
Big Five Questionnaire (BFQ) (Caprara, Barbaranelli, Borgogni & Perugini, 1993). It is a 132-items personality questionnaire based on five dimensions: Energy, Affability, Tenacity, Emotional Stability and Mental Openness. Besides, there are ten subdimensions (Dynamism, Dominance, Cooperation, Cordiality, Scrupulosity, Perseverance, Control of Emotions, Control of Impulses, Culture Openness and Experience Openness. It was fully applied.
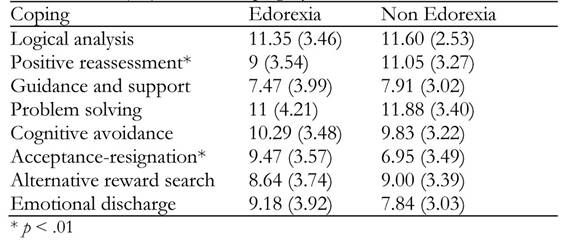
CRI-A Coping Styles Questionnaire (Moos, 1993). It is based on 48 items, divided into 8 scales, grouped in approach scales and avoidance scales, Logical analysis, Positive reassessment, Guidance and support search, Problem solving, Cognitive avoidance, Acceptance or resignation, Alternative reward search and Emotional discharge.
Procedure
For this study we carried out a recruitment process of the sample of participants, by means of a call to the university community of the University of Murcia, to which 111 responded voluntarily.
The questionnaires were distributed in groups, depending on participants’ availability. Subsequently, anthropometric measurements were taken by means of a bioimpedance scale and a measuring rod. Once the participant answered the test set and the sociodemographic questionnaire, and we noted down their anthropometric measurements, they were classified in edorexic or non-edorexic according to their score.
After data collection, 36 subjects were excluded from the study following the exclusion criteria. Therefore, the final sample consisted of 75 participants: 17 diagnosed as edorexic and 58 as non-edorexic.
Statistical analysis
The chi-square test was used to compare frequencies of behaviours related to food abuse and restriction between edorexic and non-edorexic groups. To compare means between both groups, Student’s t-test was used, both in personality dimensions and subdimension (BFQ) and in coping styles (CRI-A), after verification of variances homogeneity using Levene’s test. As a measure of the effect size, Odds ratio and its 95% interval are provided to compare proportions, and Cohen’s d to compare means. All calculations were performed using SPSS (v.19).
Results
Information provided by ESQ allows the identification of a series of behaviours related to food consumption and exercise practice in which edorexic subjects behave in a significantly different way to non-edorexic ones. Table 2 shows that edorexic subjects with normal weight consume significantly more food uncontrollably, diet more, and avoid the intake of some foods more often. They appear to perform physical activity more frequently, although they recover their lost weight more frequently too. Edorexic subjects show to have more difficulties to follow healthy habits, although this difference is not statistically significant.

Regarding personality factors, any group differs in most dimensions of BFQ (see Table 3), except for emotional stability, significantly lower in edorexic subjects (t 86 = 2.782; p = .007; SD = .75). In this regard, there are no differences in BFQ subdimensions, except for emotional control, which, in the same sense, is significantly lower in edorexic subjects (t 86 = 3.174; p = .002; SD = .86).
Finally, in terms of coping response (see Table 4), edorexic subjects show a significantly higher resource of acceptance-resignation (t 86 = 2.609; p = .011; SD = -.70) and significantly lower resource of positive reassessment (t 86= 2.232, p = .029; SD = .60). There were no statistically significant differences in the rest of coping styles.
Discussion
This study aims to go deeply into the psychological factors related to food consumption without physiological need, specifically the mental disorder called Edorexia Syndrome and its connection with personality and coping style.
Compared with the control group, individuals positively diagnosed with this syndrome showed tendency to low-calorie diets. These data are in line with several authors. Firstly, Lauzon-Guillain et al. (2006) consider food restriction as a strategy to avoid fat accumulation. Secondly, Ogden (2003) concluded that dieting could be associated with an improved self-control and, consequently, would be a relief to the sense of loss of control. Therefore, high tendency of edorexic individuals to diet could be related to their fear of gaining weight and the need to reduce perception of loss of control.
Regarding uncontrolled food consumption and without physiological need, the data obtained show a direct relation with Edorexia Syndrome individuals. These data are related to the results of Balantekin and Roemmich (2012). These authors identified that individuals with a high food restriction faced stressful situations with increased consumption. In addition, other authors consider overfeeding as a consequence of food dependence (Pelchat, 2009) or a strategy to cope with anxiety situations (Blum, Liu, Shriner & Gold, 2011). In this line, individuals with Edorexia Syndrome may tend to avoid food consumption through diets and restriction of some foods, while abusing others.
Edorexic individuals recover easily their lost weight, as our data show. These results coincide with Beiseigel and Nickols-Richardson (2004) who observed a rebound effect in individuals who carried out food restrictions. However, there are also studies that do not notice this relation (Lawson et al., 1995; Lindroos et al., 1997), so future studies should go deeper into this topic.
Regarding personality pattern, non-obese edorexic individuals score lower on control of emotions and emotional stability. These data can rely on five-way theory (Macht, 2008), which proposes that negative emotions can increase food intake (Gibson and Green, 2002; Macht & Mueller, 2007), i.e. this theory relates lack of skills to manage emotions with uncontrollable food abuse. In accordance with the studies of Bollen and Wojciechowski, (2004), Keller and Siegrist (2015) and MacLaren and Best (2009), it is observed that emotional instability may be the key to the development of excessive food intake. On the other hand, edorexic individuals present an emotional discharge that refers to the behavioural attempts to reduce tension through the expression of negative feelings. This data are in line with the research by Macht, (2008) and Blum, Liu, Shriner & Gold (2011); eating behaviour can be understood as a behavioural attempt to reduce an aversive stimulus. In accordance with Koff and Sangani (1997) and Lee et al. (2007), this coping style is also related to excessive food intake, as our data show.
In conclusion, the data obtained could show a behaviour and personality pattern related to a poorly studied psychological problem. Edorexia Syndrome is characterized by a lack of ability to manage emotions and behavioural attempts to solve this deficiency. Consequently, individuals with this problem try to compensate for their lack of emotional control by carrying out dietary behaviours such as food abuse and restriction of other types of foods.
However, this paper may present limitations that could be improved by a broader sample; the ESQ could be accompanied by some method of dietary assessment that allows to improve its objectivity in food intake; to diagnose individuals with Edorexia Syndrome, a psychological interview could be used, and the number of studies on the Edorexia Syndrome could increase. In this sense, future research should continue to delineate in this syndrome as it differs from other eating behaviour disorders. In addition, the relation that emotional management has with uncontrolled abuse and dieting in non-obese people should be further analysed.

