










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.104 no.6 Madrid jun. 2012
https://dx.doi.org/10.4321/S1130-01082012000600008
PICTURES IN DIGESTIVE PATHOLOGY
Bouveret syndrome: an infrequent presentation of gallstone ileus
Una forma infrecuente de íleo biliar: síndrome de Bouveret
Antonio Palomeque-Jiménez, Salvador Calzado-Baeza and Montserrat Reyes-Moreno
Department of Surgery. Hospital de Santa Ana. Motril, Granada. Spain
Case report
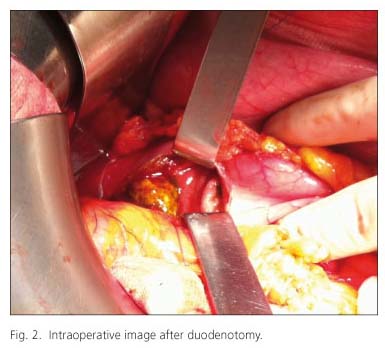
We report the case of a 75-year-old woman with a personal background of hypertension and peptic ulcer with a 5-days history of constipation, vomiting and abdominal pain. Simple radiology and abdominal computed tomography were performed, finding a great dilatation of the stomach until the first portion of the duodenum. The obstruction was due to a gallstone obstruction in the second portion of the duodenum (Fig. 1). The patient underwent emergency laparotomy. A gastric dilatation and an inflammatory plastron in the duodenum were found. Duodenotomy (Fig. 2) and gallstone removal was performed (Fig. 3). No surgery over the gallbladder or the fistula was performed.


Discussion
Bouveret syndrome is an infrequent presentation of gallstone ileus. It is caused by the presence of an obstructive gallstone in the duodenum. The gallstone is usually single and bigger than 2 centimeters. It accounts for the 2-3% of the cases of gallstone ileus and it is due to a cholecystoduodenal or cholecystogastric fistula. It usually occurs in elderly women with comorbidities and its clinical presentation is not very specific (1).
The diagnosis usually requires radiology techniques. Simple abdominal radiology can reveal pneumobilia, which can be diagnostic in the 23% of cases. Abdominal ultrasounds as well as gastrointestinal transit with barium meal can be of interest. Also tomography, as in our case, can be useful. Gastroscopy may have diagnostic and therapeutic interest, allowing the removal of the gallstone (2). However, there are very few cases reporting a single endoscopic treatment, or even combined with extracorporeal lithotripsy (3).
In our case, gastroscopy was not performed since it is not available for emergency in our hospital.
The definitive treatment is mainly surgical (2), with the removal of the gallstone and the eventual repair of the biliodigestive fistula.
References
1. Vidal O, Seco JL, Álvarez A, Triñanes JP, Serrano SR. Síndrome de Bouveret: cinco casos. Rev Esp Enferm Dig 1994;86:839-44. [ Links ]
2. Ruiz HD, Bruno M, Almasqué O, García R, Giménez M, Faillace R, et al. Morbimortalidad en el íleo biliar: estudio comparativo de dos décadas. Cir Esp 1997;62:191-4. [ Links ]
3. Rivera R, Ubiña E, García G, Navarro JM, Fernández Síndrome de Bouveret resuelto mediante litotricia mecánica endoscópica. Rev Esp Enferm Dig 2006;98:790-2. [ Links ]

