










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.106 no.6 Madrid jun. 2014
PICTURES IN DIGESTIVE PATHOLOGY
Internal anal sphincter evaluation using 3D anal ultrasound
Evaluación del esfínter anal interno mediante ecografía anal 3D
José Luis López-Negre and David Parés
Department of General and Digestive Surgery. Parc Sanitari Sant Joan de Déu. Universitat de Barcelona. Sant Boi de Llobregat, Barcelona. Spain
Case report
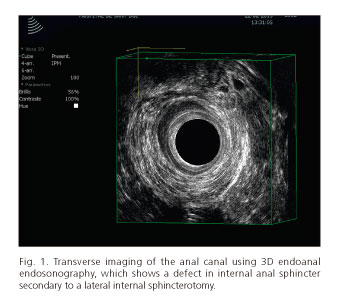
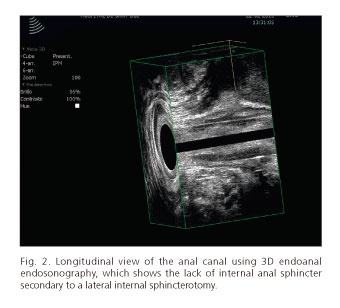
A 42 year-old male, with no relevant medical history except surgery three years before for chronic anal fissure in another center (without information regarding type of surgery), attended outpatient clinic for several week-history of anal pain. The patient related a sudden anal pain without irradiation and without relationship with defecation that improved with flexion of the lower extremities. On physical examination, the patient has no pain and there were no relevant findings. 3D endoanal ultrasound showed a defect in the internal anal sphincter on the left half of the anal canal (Figs. 1 and 2). This image was highly suggestive to be secondary to have been operated using a lateral sphincterotomy technique. The patient was diagnosed with chronic idiopathic anal pain type Proctalgia fugax and he was successfully treated with topical diltiazem.
Discussion
To study the morphology of internal anal sphincter, 3D endoanal ultrasound is a suitable technique (1). The internal anal sphincter assessment is necessary in different clinical situations. Specially, in those patients in whom there is a history of previous anal surgery for anal fissure and anal pain could permit to consider as anal fissure recurrence (2). This technique allows, depending on the appearance of internal anal sphincter, to consider whether the patient has been properly operated (internal sphincterotomy technique) (3,4). The presented case was finally diagnosed with chronic idiopathic anal pain (type Proctalgia fugax), which is very common that patients have previously undergone surgery for anal fissure. Thus, outcome was favorable with medical treatment, as it has been described (5). In cases of poor outcome with medical treatment, some alternatives like biofeedback may be considered (5).
References
1. Tan E, Anstee A, Koh DM, Gedroyc W, Tekkis PP. Diagnostic precision of endoanal MRI in the detection of anal sphincter pathology: a meta-analysis. Int J Colorectal Dis 2008;23:641-51. [ Links ]
2. Vieira AM, Castro-Poças F, Lago P, Pimentel R, Pinto R, Saraiva MM, et al. The importance of ultrasound findings in the study of anal pain. Rev Esp Enferm Dig 2010;102:308-13. [ Links ]
3. Christiansen J, Bruun E, Skjoldbye B, Hagen K. Chronic idiopathic anal pain: analysis of ultrasonography, pathology, and treatment. Dis Colon Rectum 2001;44:661-5. [ Links ]
4. Arroyo A, Pérez-Vicente F, Serrano P, Candela F, Sánchez A, Pérez-Vázquez MT, et al. Tratamiento de la fisura anal crónica. Cir Esp 2005;78:68-74. [ Links ]
5. Jeyarajah S, Chow A, Ziprin P, Tilney H, Purkayastha S. Proctalgia fugax, an evidence-based management pathway. Int J Colorectal Dis 2010;25:1037-46. [ Links ]

