










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.106 no.7 Madrid jul./ago. 2014
LETTERS TO THE EDITOR
Hepatic adenomatosis: A rare cause of liver transplant
Adenomatosis hepática: una causa infrecuente de trasplante hepático
Key words: Hepatic adenomatosis. Liver transplant.
Palabras clave: Adenomatosis hepática. Trasplante hepático.
Dear Editor,
Hepatocellular adenoma is the most common benign epithelial liver tumour, with an estimated average incidence of 3 cases/million people/year. It was first described by Edmondson in 1958 (1,2).
Hepatic adenomatosis (HA) was described by Flejou et al. in 1985, who reported 13 patients with multiple hepatocellular adenomas. The diagnostic features were: a) Presence of multiple hepatic nodules; b) similar distribution in both sexes; c) no confirmed association with prolonged oral contraceptive intake; d) presence of elevated serum alkaline phosphatase and GGT. Fewer than 4 % of all HA cases require orthotopic liver transplantation (OLT) (3).
Case report
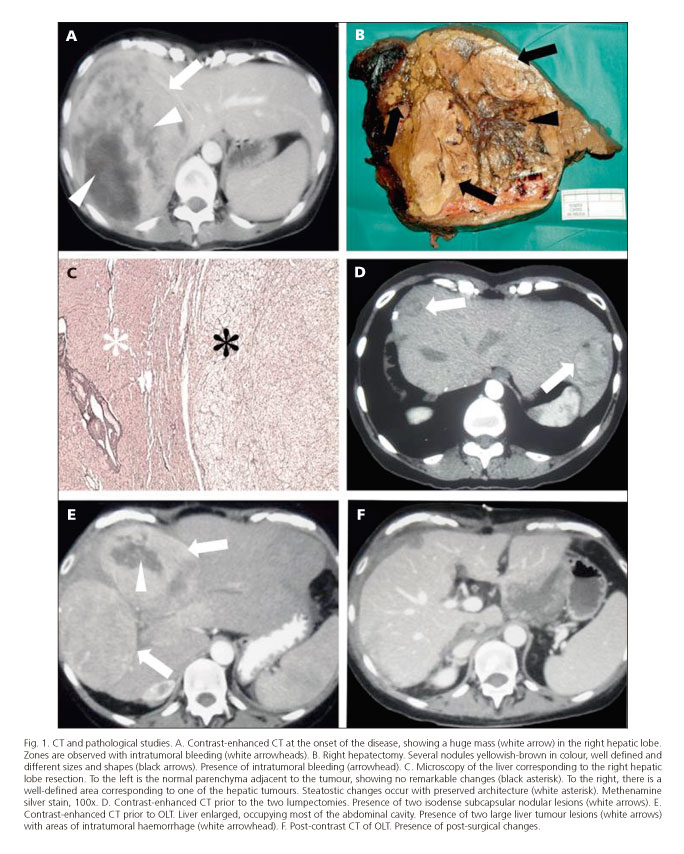
A female, 31 years-old, with a long history of oral contraceptive use, presented in the emergency room with acute abdominal pain and dyspepsia. Physical examination revealed moderate hepatomegaly. She presented moderate anaemia and liver function tests were normal. An abdominal CT identified a large liver mass measuring 17 x 16 cm, with a heterogeneous appearance and signs of bleeding, located in the right hepatic lobe (Fig. 1A). A fine needle aspiration was performed, which revealed no evidence of malignancy. The patient underwent a right hepatectomy.
The removed piece of liver measured 22 x 18 x 14 cm and weighed 2,300 g. Gross multiple nodular lesions with intratumoral haemorrhagic areas were observed (Fig. 1B). Microscopic examination revealed hepatocytes with foamy cytoplasm, with round nuclei and multiple uniform adenomatous nodules with varying degrees of steatosis (Fig. 1C). Taken together, the clinico-pathological findings were consistent with an HA with extensive involvement of the right hepatic lobe. Two years later, two new small lesions were observed in the left hepatic lobe. These were also resected (Fig. 1D).
After four asymptomatic years, the patient presented again with a clinical picture of acute abdominal pain. Abdominal CT revealed two large liver tumour lesions (Fig. 1E). Finally, the patient underwent an OLT (Fig. 1F). Three years later, she continues to be healthy and disease-free.
Discussion
The customary treatment of HA with localised lesions in one lobe is partial surgical resection by segmentectomy, hemi-hepatectomy or extended lobectomy (4-6).
Patients with multifocal lesions should be periodically monitored by serial measurements of serum alpha-fetoprotein and the periodic use of imaging techniques, principally magnetic resonance imaging, carried out at least, annually.
Disease progression is confirmed by the presence of large subcapsular adenomas (> 4 cm). The risk of malignancy and the presence of persistent symptoms are indications for performing partial resections of multifocal lesions. Partial resection is the preferred option, unless this is technically impossible (7,8).
Liver transplantation is the last therapeutic option. The indications for carrying this out include continuously elevated serum AFP, suspicion of malignancy from imaging techniques and/or PAF or BAF positivity in highly symptomatic patients, or those with marked hepatomegaly, or a history of repeated complications of adenomas, as occurred in the case described here (9,10).
Iván Fernández-Vega1, Jorge Santos-Juanes1, Carmen García-Pravia1,
Manuel F. Fresno-Forcelledo1 and Luis Rodrigo2
1Pathology Department and 2Gastroenterology Service.
Hospital Universitario Central de Asturias. Oviedo, Spain
References
1. Rooks JB, Ory HW, Ishak KG, Strauss LT, Greenspan JR, Hill AP, et al. Epidemiology of hepatocellular adenoma. The role of oral contraceptive use. JAMA 1979;242:644-8. [ Links ]
2. Edmondson HA. Tumors of the liver and intrahepatic bile ducts. Section 7, fascicle 25, Atlas of Tumor Pathology. Washington: Armed Forces Institute of Pathology; 1958. [ Links ]
3. Flejou JF, Barge J, Menu Y, Degott C, Bismuth H, Potet F, et al. Liver adenomatosis. An entity distinct from liver adenoma? Gastroenterology 1985;89:1132-8. [ Links ]
4. Vetelainen R, Erdogan D, de Graaf W, ten Kate F, Jansen PL, Gouma DJ, et al. Liver adenomatosis: Re-evaluation of aetiology and management. Liver Int 2008;28:499-508. [ Links ]
5. Hagiwara S, Takagi H, Kanda D, Sohara N, Kakizaki S, Katakai K, et al. Hepatic adenomatosis associated with hormone replacement therapy and hemosiderosis: A case report. World J Gastroenterol 2006;12:652-5. [ Links ]
6. Adam R, Karam V, Delvart V, O'Grady J, Mirza D, Klempnauer J, et al. Evolution of indications and results of liver transplantation in Europe. A report from the European Liver Transplant Registry (ELTR). J Hepatol 2012;57:675-88. [ Links ]
7. Ribeiro A, Burgart LJ, Nagorney DM, Gores GJ. Management of liver adenomatosis: Results with a conservative surgical approach. Liver Transpl Surg 1998;4:388-98. [ Links ]
8. Bambha K, Nagorney D, Sanderson S, Gores GJ. Hepatic adenomatosis in a young woman with glucose intolerance. Nat Clin Pract Gastroenterol Hepatol 2006;3:526-31; quiz (following 31). [ Links ]
9. Foster JH, Berman MM. The malignant transformation of liver cell adenomas. Arch Surg 1994;129:712-7. [ Links ]
10. Chiche L, Dao T, Salame E, Galais MP, Bouvard N, Schmutz G, et al. Liver adenomatosis: reappraisal, diagnosis, and surgical management: Eight new cases and review of the literature. Ann Surg 2000;231:74-81. [ Links ]

