










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.107 no.2 Madrid feb. 2015
LETTERS TO THE EDITOR
Lethal pseudomembranous colitis in an immunocompetent patient
Colitis pseudomembranosa letal en paciente inmunocompetente
Key words: Pseudomembranes. Colitis. Cytomegalovirus. Immunocompetence. Infection. Severe disease. Surgery.
Palabras clave: Seudomembranas. Colitis. Citomegalovirus. Inmunocompetencia. Infección. Enfermedad grave. Cirugía.
Dear Editor,
The most common etiology of diarrhea in hospitalized patients is Clostridium difficile (CD). This bacterium can cause pseudomembranous colitis (PC), although there are other agents that also can produce this illness, such as cytomegalovirus (CMV) that, occasionally, can affect immunocompetent patients.
We present a case of severe pseudomembranous colitis by CMV in an immunocompetent patient, after a clean elective surgery for ovarian cyst.
Case report
A 69-year-old woman, who underwent laparoscopic left oophorectomy for benign ovarian cyst 6 days before, without requiring prophylactic antibiotherapy. She was readmitted to the hospital because of diarrhea initiated the first postoperative day.
The CT scan showed colonic dilation and inflammatory changes in the sigma and rectum wall (Fig. 1). Flexible sigmoidoscopy demonstrated pseudomembranes and ulcerations in the mucous membrane. It was oriented as a PC (with compatible biopsies) establishing treatment with metronidazole. The detection in stool samples of toxin A and B for CD was negative as well as the stool culture and serology for HIV.

Because of a torpid evolution with vomiting and megacolon without toxaemia, she was urgently operated and a subtotal colectomy with ileostomy was carried out, twelve days after admission.
In the postoperative period, she was admitted to the Intensive Care Unit needing vasoactive drugs due to a multiple organ failure and treated with piperazilin-tazobactam.
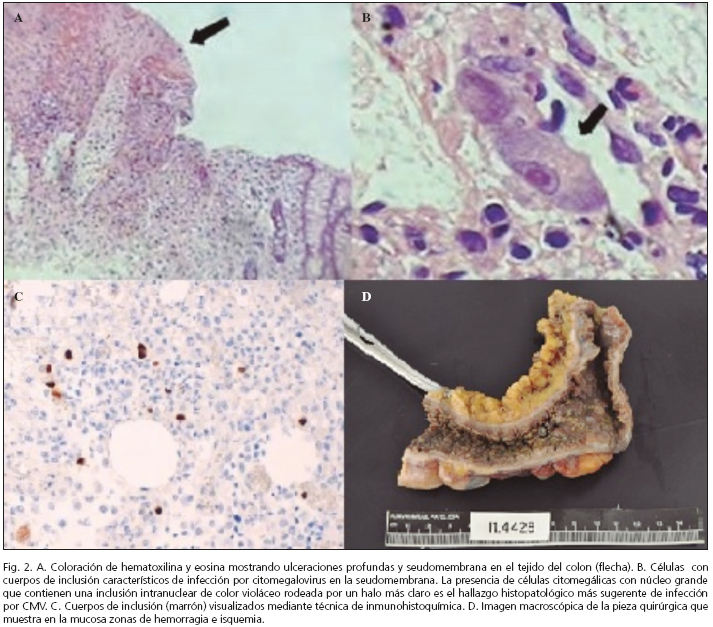
On the 5th day, she became hemodynamically unstable due to upper gastrointestinal hemorrhage and signs of ischemia in the ileostomy. The upper endoscopy showed a friable, necrotic and ulcerated mucosa from the esophagus to the duodenum. The results of the surgical specimen (Fig. 2D) reported pseudomembranous colitis with inclusion bodies (Fig. 2) (immunohistochemical technique) (1) (Fig. 2C), treated with foscarnet but the patient developed a multisystem failure dying the eighth day. The initial sigmoidoscopy biopsies were reviewed without evidence of inclusion bodies.
Discussion
Although in 96-100 % of the cases of PC the cause is CD (2), it also can be caused by other agents, like CMV.
The clinical spectrum ranges from a simple diarrhea to a fulminant colitis with a mortality rate of up to 80 % (3).
Its diagnosis, in addition to the sigmoidoscopy, involves the search for the causative agent by stool cultures, serology... Nowadays, it has been using the CT scan as an initial complementary test because of its quick results. Typical findings are dilation and thickening of the colonic wall, "sign of the accordion" and ascites.
In an immunocompetent host, CMV infection is usually mild but severe cases have also been described (4,5) in immunocompetent patients, although they usually are elderly, with comorbidity (6) and/or underlying intestinal inflammatory illness.
Although CMV can affect any part of the gastrointestinal tract, the most frequent affected are colon and rectum (7-9). Common endoscopic findings are erosions and ulcerations (4,8), but it has also been described pseudomembranes in 2 % case (2,10).
CMV colitis may be complicated with massive hemorrhage, toxic megacolon (7)..., requiring surgery and the best technical election is subtotal colectomy with ileostomy.
The possibility of a specific treatment is hindered by usual late diagnosis. Furthermore, the use of ganciclovir and foscarnet is controversial in the immunocompetent subject due to their toxicity.
Cristina Gas-Ruiz1, Susana Eugenia Ros-López1, Felip Vilardell-Villella2,
Carmen Mias-Carballal1, Rafael Villalobos-Mori1, Mari Cruz de la Fuente Juárez1,
Juan Antonio Baena-Fustegueras1 and Jorge Juan Olsina-Kissler1
Departments of 1General Surgery and 2Pathology.
Hospital Universitario Arnau de Vilanova. Lleida, Spain
References
1. De Castro ML, Tardío A, Del Campo V, Estévez A, Pineda JR, Domínguez F, et al. A comparative study of two histological techniques for the identification of cytomegalovirus infection in colorectal biopsies from patients with chronic inflammatory bowel disease. Rev Esp Enferm Dig 2009;101:697-705. [ Links ]
2. Orellana A, Salazar E. Colitis pseudomembranosa asociada al uso de antibióticos. Revisiones bibliográficas. Acta Odontol Venezolana 2009;47:1-5. [ Links ]
3. Greenstein AJ, Byrn JC, Zhan LP, Swedish KA, Jahn AE, Divino C. Risk factors for the development of fulminant Clostridium difficile colitis. Surgery 2007;143:623-9. [ Links ]
4. Seo TH, Kim JH, Ko SY, Jong SN, Lee SY, Sung IK, et al. Cytomegalovirus colitis in immunocompetent patients: A clinical and endoscopic study. Original Paper. Hepatogastroenterology 2012;59:2137-41. [ Links ]
5. Rafailidis PI, Mourtzoukou EG, Varbobitis IC, Falagas ME. Severe cytomegalovirus infection in apparently immunocompetent patients: A systematic review. Review. Virol J 2008;5:47. [ Links ]
6. Kurtz M, Morgan M. Concomitant Clostridium difficile colitis and cytomegalovirus colitis in an immunocompetent elderly female. BMJ Case Rep 2012 Dec Doi: 10.1136/bcr-2012-007273. [ Links ]
7. Dinesh BV, Selvaraju K, Kumar S, Thota S. Cytomegalovirus-induced stricture presenting as acute intestinal obstruction in an immunocompetent adult. BMJ Case Rep Published online: 2013 Sep 10 Doi: 10.1136/bcr-2013-200944. [ Links ]
8. Galiatsatos P, Shrier I, Lamoureux E, Szilagyi A. Meta-analysis of outcome of cytomegalovirus colitis in immunocompetent hosts. Dig Dis Sci 2005;50:609-16. [ Links ]
9. Tejedor MA, Velasco A, Fernández A, Piñero MC, Calderón R, Prieto AB, et al. Ileítis por citomegalovirus en paciente inmunocompetente. Rev Esp Enferm Dig 2011;103:154-6. [ Links ]
10. Nomin N, Telisinghe PU, Chong VH. Cytomegalovirus colitis in immunocompetent patients. Case Report. Singapore Med J 2011;52:e170-2. [ Links ]

