










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
The Project MEDICS was approved by the European Commission on the initiative of the Italian Administration1, concerned by the increasing number of inmates with psychopathological disorders. This project was carried out between June 2014 and June 2016 and among its activities we hereby present this project. The objective was to know the stance of correctional staff on the potential causes, management methods and improvement proposals regarding the assistance to inmates with psychopathological disorders aside severe mental disorders. We intended to obtain the information from the practices implemented by the Administration of each participating country: Catalonia, Croatia, Wales and England. We had a triple aim:
to develop plans in the reception, assistance and treatment of inmates;
to implement regulated training programs for correctional staff (healthcare or not); and
to make recommendations to the EU Commission for Justice, which had already stated its concern on this issue.
The European Parliament Resolution 2011/2897 (RSP)2 of December 2011 on the detention conditions in the European Union, considered alarming the increased number of inmates with mental and psychological disorders and in its initiative number 7 called on Member States “ to earmark appropriate resources for the restructuring and modernisation of prisons, to protect detainees’ rights (…) to provide the police an prison staff with training based on contemporary prison management practices and European human rights standards, to monitor prisoners suffering from mental and psychological disorders and to create a specific EU budget heading with a view to encouraging such projects”.
In the same league, European Recommendation Rec (2006)3 of the Committee of Ministers to member states on the European Prison Rules was issued, where we find two basic principles, fully integrated in the objectives of the project: 40.5 which states that all necessary medical, surgical and psychiatric services including those available in the community shall be provided to the prisoner for that purpose and 47.2 which states that the prison medical service shall provide for the psychiatric treatment of all prisoners who are in need of such treatment and pay special attention to suicide prevention.
Other European Recommendations, such as Recommendation CM/Rec (2012) 12 of the Committee of Ministers to member states concerning foreign prisoners4 and Recommendation R (2004) concerning the protection of the human rights and dignity of persons with mental disorders5, as well as Article 35 of the latter deepen even more this specific issue. Moreover, they add that prisoners should be able to access an appropriate therapy and that involuntary treatment should not be carried out in correctional facilities but in hospitals or specific units adapted to the treatment of mental disorders. Last, these Recommendations also bring to light that an independent system should supervise their treatment and ensure the care that should be provided to affected prisoners.
MATERIAL AND METHODS
The study gathered the opinion of correctional staff in contact with prisoners of standard modules, not in psychiatric infirmaries or penitentiary psychiatric units/hospitals with no diagnosis of psychiatric disorder. We intended to know the degree of knowledge and attitude of the staff towards potential psychopathological disorders, aside severe mental disorders.
We used a quantitative methodology, based on a sole technique of data use, based on questionnaires. These were designed in the leading country (Italy) and adapted and differentiated according to the professional collective targeted. Seven different groups were identified: prison wardens, treatment technicians, surveillance officers, teachers, primary care physicians, nurses with no experience on mental health and volunteers.
Field work was previously presented to management teams in prisons and was carried out between 23/2/2015 and 23/5/2015 in three correctional facilities: a male prison with 1050 inmates, a female facility hosting 252 women and a juvenile facility with 260 preventive detainees.
The target population was 744 members of the staff in direct contact with prisoners. Seven types of autofill questionnaires were designed for each collective. Participation was voluntary.
Sampling procedure: Management teams in each prison distributed and collected the questionnaires. These were later sent to the General Directorate of the Corrections Department for their revision and classification. Last, they were forwarded to the University of Vic-Central University of Catalonia for statistical processing.
Data was processed by means of the statistical software SPSS-PC. For the description of continuous variables, the mean, standard deviation, minimum, median, maximum and number of valid cases were used. For the description of categorical variables, the number and percentage of patients per category were used. In all statistical tests, a level of statistical significance (p) of 0.05 was defined.
RESULTS
Participants Features
Out of 744 potential participants, 174 (23.4%) fulfilled que questionnaires. The participation was higher among wardens, nurses, physicians, teachers and treatment technicians (Figure 1). The men age was 46.3 (standard deviation 9.6 ± 3.7). Only participants of the treatment teams included people under 25 years old. Moreover, physicians presented an older mean age than other groups 856.8 vs 46.3) with statistically significant differences (p >0.001). According to genre, 57.7% were women and 40.7% men.

Professional experience was over 5 years as a mean and longer (mean ≥ 10 years) in nurses and surveillance officers. 67% of all participants were university graduates and 70% of surveillance officers had higher studies. Furthermore, most of professionals (62.4%) reported having direct or indirect experience on the issue: 38.1% had attended training courses and 34.1% reported a personal interest or studies on the issue.
Most relevant descriptive characteristics on the content of answers according to specific collectives
Wardens
100% answered the question “Does the prison you manage ensure appropriate care to prisoners with psychopathological disorders?” with “Yes, in collaboration with the prison’s healthcare team and the national health system”.
Treatment teams
For the question “What tools would be useful introducing for an early identification of the disorders?” which was also asked to wardens, the most common answers were contact with an expert on psychopathology and information protocols (Figure 2). As well, 92% defended the need of specific training on mental health issues. In fact, in the question “The prison where you work can ensure appropriate care and treatment to prisoners with mental disorders?” 37% of professionals believed that should be involved in the assistance of these prisoners but that the responsibility should further rest in psychiatrists and clinical psychologists. Yet, 33% believed that “this type of assistance was only a responsibility of physicians”.
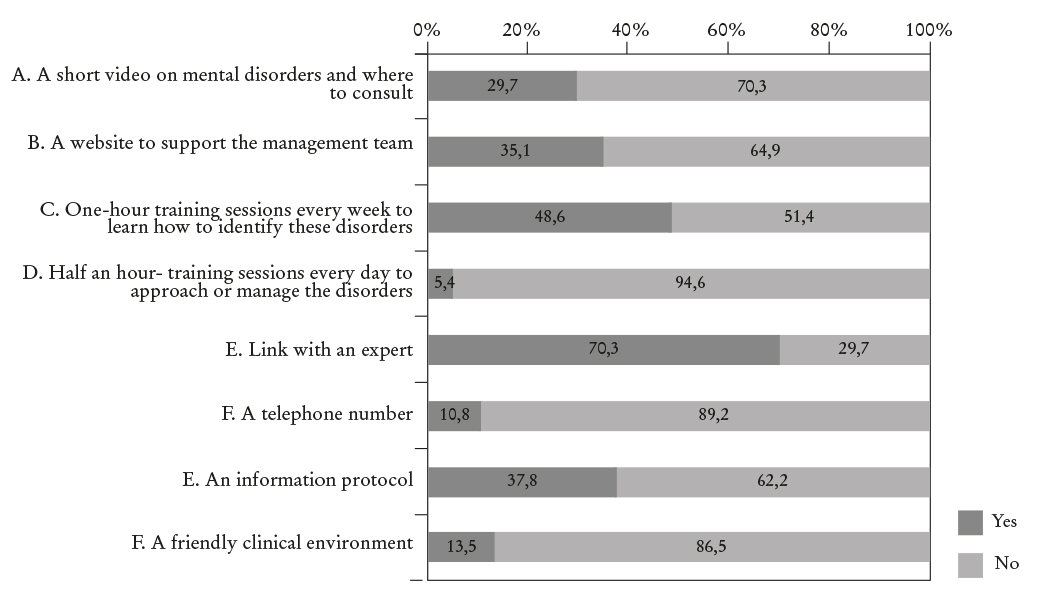
Figure 2 Assessment of potential tools for the identification of mental disorders provided by wardens and treatment units.
The statement “Contact with a psychiatry specialist” was reported in 81.1% of all answers to the question “What is the best option when reporting that a prisoner may be developing a mental disorder?”. And for the question “Would it be useful to update your knowledge in identifying and managing prisoners with severe mental issues?”, 91.9% answered “Yes, I would like to know more on this issue”.
Surveillance officers
For the questions “What are the causes or states of uneasiness among inmates?” the most common answer was “inappropriate drug use”, followed by “lack of support”, “being raised in a dysfunctional family” and “presence of internal psychological conflicts” (Figure 3).

Figure 3 Distribution of the main causes leading to disturbance or disorders according to surveillance officers.
About the question “What sources of support or resources can be activated in prison?” the most common answer was “Join a self-help group” (22.9%) while the “initiation of therapeutic activities” and “reach someone trustworthy” were options for 15.7% and 2.9% of the sample correspondingly. For the question “Who do you contact when you identify some sign or problem among inmates before they resort to self-harm or severe self-harm?” the most relevant answers were “my immediate supervisor” (63%) and “the physician” (33.3%). With reference to the question “Do you believe that you form part of a system aimed at reducing problems?” 75% answered affirmatively. And for the question “What future do inmates with psychopathological disorders face?”, the general opinion is pessimistic since they believe that the problem will remain despite undergoing treatment and that it will get worse in those who do not initiate therapeutic measures. In relation to the question “What situations could promote or jeopardize the rehabilitation of inmates with psychopathological disorders?” the most common answer (60%) for positive situations was “individual or group psychological treatment” and as a hindering factor “Discontinuation of the prescribed treatment” (72%) and “Not having anything to do” (80%).
Teachers/Trainers
SOnly one question directly addressed the issue of students’ mental health. Most of the professionals (71%) would accept students with some type of psychopathological disorder as long as “They underwent some type of treatment” (12.9%).
Physicians
The first section had to do with inmates that were under periodic psychiatric control and supervision and the second, with inmates who were exclusively controlled by primary health physicians. For those inmates with a background of attempted suicide but under the control and supervision of psychiatrists, 91% of physicians preferred not to admit the patient in the 24 hours psychiatric observation ward. When asked about their actuation before self-harm episodes, the most frequent answer was “Talking directly to the inmate” (90.0%). Both for self-harm episodes and attempted suicide, assistance was immediate (100%). They also answered on the factors that most negatively affected their intervention. The most common answer was “The lack of staff specifically trained on mental health”.
Regarding the inmates without psychiatric supervision/control, before recent episodes of self-harm or attempted suicide, the most common intervention was contacting the psychiatry team (91%). In these cases, the most negative factor was the lack of specific training on mental health by the correctional staff (18.2%) (Figure 4).

Nurses
This group was the only one to highlight the importance of everyday experience as part of their training. It is worth considering the answers to the main questions:
- “What factors do you believe that influence the psychological stability of prisoners?”: “The use of drugs or psychotropic substances” (88.2%), “Acute pain” and “The lack of impulse control” (76.5%) were the main answers.
- “What types of support measures can be activated in prison?”: “Improved assessment of individual needs” was the most common answer (82.4%). Furthermore, the promotion of continuous technical education was considered necessary (70.6%).
- “What interventions can be most effective?”: For this collective “Psychotherapeutic treatment (56.3%) and “Family and Friend support” (18%) were the most common answers.
- “What situations could encourage or jeopardize the recovery of prisoners with psychopathological disorders?” (Figure 5): promotors were considered “Individual or group psychological treatment” (82.4%) and “Encouraging inmates to take part in collective activities within or outside the facility” (52.9%). Negative factors were considered “Inappropriate penitentiary structures” (29.4%), “Not having anything to do”; “Stress situations” and “Discontinuation of prescribed treatment” (88.2%).

Figure 5 Distribution and quantification of the causes that encourage or jeopardize the recovery of prisoners with psychopathological disorders.
Volunteers
They considered promotors for recovery “Encouraging inmates to take part in collective activities or sports in the open” (53.3%) and “Increasing family visits outside prison” (46.7%); and negative factors: “Not having anything to do” (100%), “Stressors (such as overcrowding)” (60%), “Inappropriate penitentiary structures” (53.3%) and “Discontinuation of prescribed treatment” (33.3%).
DISCUSSION
The prevalence of mental disorders in prison is very high. A study considering Spanish prisoners estimated a lifetime prevalence for mental disorders, including drug abuse, of 84.4%: five times higher than in the general population6. These results do not differ significantly from those presented by other countries of our socioeconomic background7 8. Thus, the concern of health authorities in the European Union for this issue and the implementation of projects such as that presented by this article. It was carried out in the autonomous community of Catalonia, the only one in Spain with its own healthcare and penitentiary competences. Moreover, this community has a psychiatric model that significantly differs from those in the rest of the country, with its own organization system and therefore, results may not be extrapolated to other Penitentiary Administrations in Spain, although collectives developing their job un psychiatric infirmaries and penitentiary psychiatric units were excluded from the study.
From the initial design of questionnaires, their fulfilment, collection and classification, the statistical processing, analysis and discussion of results took approximately seven months. The duration of the fulfilment of questionnaires took three of the seven months, time enough for the staff to report their degree of knowledge, stance and criteria on the causes of behaviours of potential dysfunction or psychopathological disorder, the methods of management and the improvement proposals in the assistance of these inmates. Part of the questionnaire targeted at physicians asked on interventions associated to self-herm and suicidal behaviours, which are also especially prevalent in the correctional setting aside diagnosed mental disorders. In Catalonia, for example, the mean yearly incidence of suicide in prison for a 15-years period was 59 per every 100,000 inmates according to a study published in 2009, almost eight times higher than in the general population. It was therefore estimated that imprisonment implied an eight-fold increase of the risk of suicide9. As for self-harm behaviours, these are very common, but in 80% poorly determinant, of low fatality and frequently demanding and manipulative10.
It is worth highlighting that the analysis of questionnaires showed an increased awareness of mental health disorders among prisoners with no discrimination due to this fact. We should also consider that 67% of participants were highly qualified, which can affect the results obtained. On the other hand, their homogeneity leads to the belief that results can be very accurate in depicting the opinion of professionals.
Since prisons receive many information requests connected to penitentiary and criminological research that interfere with everyday activities, at first questionnaires did not receive a very enthusiastic response. Presumably this affected certain groups, such as surveillance officers, that were concerned that their activities would be inspected. On the other hand, all participants considered that questionnaires were too long and difficult to answer.
The overall participation of professionals is considered insufficient, since the error rate of the sample is ± 6.5% for a participation of 23.4%. Nevertheless, we should consider that the results for each collective are scientifically valid, with participation rates over 30% in five of the groups. By contrast, the results obtained in the two remaining groups are a “weak spot” of the study. Therefore, the low participation rate among volunteers (4%) lead to their exclusion even though the information on their opinions was gathered. The main factors explaining this participation rate were: a) their register had not been updated for a long time; b) their number had significantly dropped throughout recent years due to subsidy cut-offs; and c) their presence in prisons has been sporadic for the last years. Instead the study’s “strong points” were the delimitation of the population under study, which encouraged the implementation of the project and access to participants, except for volunteers.
In conclusion, the activity exhibited by this project allowed the comparison between different approaches to manage prisoners with some type of psychopathological disorders in among studied countries, and it identified models to share. Some of the proposed recommendations, which we believe to be particularly relevant were the following:
- To promote alternative measures to detention, according to different security levels and disorder types and delay sentences in patients with severe mental disorders.
- To encourage continuous education, multidisciplinary team work and improved inter-professional relationships.
- To implement activity and rehabilitation programs according to objectives, interventions and expected results.
- To facilitate intercultural communication with foreign prisoners and, for inmates with psychopathological disorders, increase the number of family visits.
- To encourage the creation of different types of mental health experts.
- To regularize access to unprotected medical data for other professionals taking part in the rehabilitation program.
- To spread research studies by means of trans-national networks and suggest State Members the appropriate modifications by means of a series of regulations

