










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkREC: Interventional Cardiology
versión On-line ISSN 2604-7276versión impresa ISSN 2604-7306
REC Interv Cardiol ES vol.6 no.1 Madrid ene./mar. 2024 Epub 18-Mar-2024
https://dx.doi.org/10.24875/recic.m23000412
Images in cardiology
Transjugular left atrial appendage closure
aUnidad de Hemodinámica y Cardiología Intervencionista, Servicio de Cardiología, Complejo Hospitalario Universitario de Albacete, Albacete, España
bUnidad de Imagen Cardiaca, Servicio de Cardiología, Complejo Hospitalario Universitario de Albacete, Albacete, España
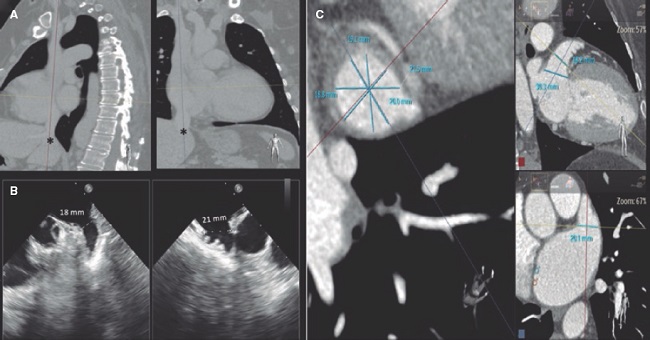
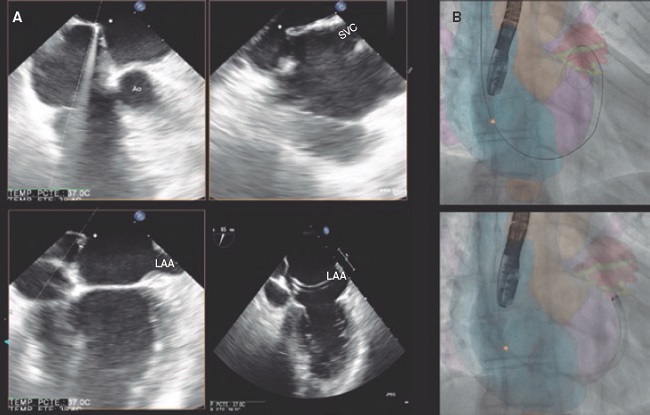
A 52-year-old woman with atrial fibrillation, thrombocytopenia, and severe gastrointestinal bleeding while on several anticoagulants was referred for left atrial appendage closure. A year earlier, pulmonary vein ablation had been attempted but femoral access proved impossible due to a previously undetected congenital interruption of the inferior vena cava (figure 1A; asterisk). A right transjugular procedure was planned under general anesthesia and guided by transesophageal echocardiography and computed tomography-fluoroscopy fusion imaging (video 1 of the supplementary data). The left atrial appendage had a windsock morphology, with a mean diameter of 20 mm at the landing zone and 30 mm at the ostium (figure 1B,C). Consequently, a 24 mm x 30 mm LAmbre LAA Occluder system (LifeTech Scientific, China) was used, because its secure anchorage and closure mainly through the disk could facilitate the procedure. Transseptal puncture was performed using an SL1 sheath and a BRK-1 XS needle (Abbott, United States) by pre-shaping a secondary curve, followed by the insertion of a SafeSept guidewire (Pressure Products, United States) specifically designed for greater accuracy of transseptal puncture (figure 2A,B; the asterisk indicates the posterior and mid-puncture. Ao, aorta; LAA, left atrial appendage; SVC, superior vena cava). The device was implanted through a 10-Fr Fustar steerable sheath (LifeTech Scientific, China), which improved reach and coaxiality (figure 3A,B. E, extension; I, impulse; LOM, ligament of Marshall; MV, mitral valve; PR, posterior rotation). The patient was discharged at 24 hours without complications and on apixaban therapy (2.5 mg for 45 days).
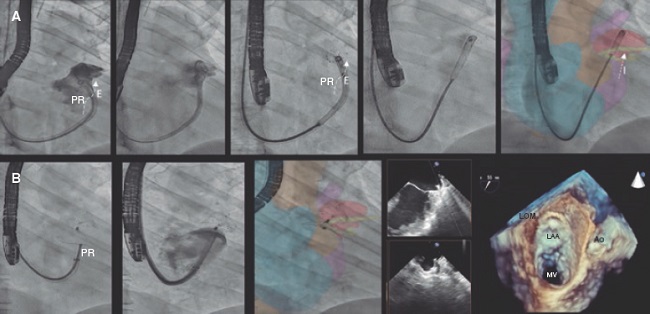
Multimodal imaging, tools that facilitate precise transseptal puncture, and steerable sheaths can simplify the performance of procedures via upper access with efficiency and safety.
ETHICAL CONSIDERATIONS
This work was published after approval was obtained from the research ethics committee of Complejo Hospitalario Universitario de Albacete, Spain. The patient gave her prior written informed consent to the intervention and publication of her case. Sex and gender variables were taken into consideration based on the SAGER guidelines.
SUPPLEMENTARY DATA
https://doi.org/10.24875/RECICE.M23000410Supplementary data associated with this article can be found in the online version available at https://doi.org/10.24875/RECICE.M23000410.
Received: July 28, 2023; Accepted: August 21, 2023; pub: October 03, 2023
 Sociedad Española de Cardiología. Publicado por Permanyer Publications. Este es un artículo open access bajo la licencia CC BY-NC-ND 4.0
Sociedad Española de Cardiología. Publicado por Permanyer Publications. Este es un artículo open access bajo la licencia CC BY-NC-ND 4.0
