










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Diabetes mellitus is a major public health problem with increasing prevalence worldwide, and in the year 2018, approximately 415 million people were estimated to have diabetes globally. This is expected to increase to 642 million of the population by 2040 [1]. Further, it is the 6th leading cause of death overall [2], contributing to 5 million deaths globally in 2017. According to the recent estimates, 69.2 million people are affected by diabetes in India [1].
Along with the rising prevalence of diabetes, an increase in its complications is also anticipated. Diabetes along with its complications is expected to result in increased morbidity, mortality, and health expenditure due to the increased requirement of specialized care [3].
Diabetic foot is one of the most substantial and devastating complications of diabetes and is defined as a group of syndromes in which neuropathy, ischemia and infection lead to tissue breakdown and possible amputation [4]. Approximately 15% of diabetic patients develop foot ulcers in their lifetime, which is known to precede amputation in 85% of the cases [5]. Every 20 seconds, a lower limb is lost to diabetes in the world, and it is the most common reason of non-traumatic lower limb amputation [6]. It is estimated that approximately 45,000 lower limbs are amputated every year in India, and the vast majority of these limbs are possibly preventable [5].
Prevention of diabetic foot ulceration is critical to decrease the associated high morbidity and mortality rates and the hazard of amputation. Several contributory factors work collectively to cause foot ulceration in patients with diabetes. These include peripheral neuropathy, mechanical stress, and peripheral vascular disease [7]. Since its development, it becomes imperatively vital to detect and diagnose diabetic peripheral neuropathy (DPN) as early as possible to prevent amputations and consequent disability and for improving the quality of life of the patients [8].
Regular and comprehensive foot examination, patient education on foot care practices such as simple hygienic practices, provision of appropriate footwear, and prompt treatment of minor injuries and a multidisciplinary team approach can reduce the ulcer occurrence by 50% and amputations by up to 85% [3, 9].
The early identification of diabetes with peripheral neuropathy and its associated factors is the key for reducing further complications and for providing baseline information to initiate appropriate interventions. There is a dearth of community-based studies, particularly from rural settings of India, which assesses the prevalence of diabetic foot and its associated risk factors among type 2 diabetics. The present study was planned to determine the prevalence of DPN and its associated risk factors in a rural secondary care setting from North India.
MATERIALS AND METHODS
STUDY DESING AND SETTINGS
This cross-sectional observational study was conducted at Civil Hospital, Naraingarh, a secondary level rural hospital attached to the Community Medicine Department of PGIMER, a premiere tertiary care medical & research Institute of North India from October to December 2018. The Non-Communicable Disease (NCD) clinic at the hospital run by resident doctors of Community Medicine under guidance of a faculty member receives patients from Naraingarh and its nearby blocks, which are predominantly rural in nature and cater to a population of approximately 100,000 people. The aim of the hospital is to provide good quality health care that is easily accessible, affordable, and culturally acceptable and to serve as a model for training post-graduates in community medicine and family medicine. The average general outpatient department (OPD) attendance of the clinic, including new and revisits, is approximately 100 per day and is held twice a week.
STUDY POPULATION AND SAMPLE SIZE
All cases of type 2 diabetes as per World Health Organization's criteria diagnosed for at least six months of duration constituted the study population. Those with cognitive impairment and obvious disability that could affect the functions of the nervous system affect independent self-care behavior, and those who had undergone amputations of the lower limbs were excluded from the study.
According to a previous study performed by George H et al. [10] from Southern India, the prevalence of peripheral neuropathy among people with diabetes was reported to be 47%. Thus, at confidence intervals of 95% and 80% power with 10% precision on prevalence of 47%, a sample size of 96 subjects was obtained. However, a total of 100 consecutive patients who were eligible and giving consent were enrolled in the study.
STUDY TOOLS
All enrolled patients with type 2 diabetes mellitus (DM) were administered a semi-structured questionnaire developed by the investigators. The questionnaire was first pilot tested on 10 patients of Type 2 DM for assessing suitability of the content, data of which was not included in the final analysis. The first part of the questionnaire consisted of data on sociodemographic details, history of diabetes mellitus including treatment details and associated risk factors for the development of diabetic foot, including dietary habits, physical activity, tobacco use and alcohol consumption, anthropometric details (height, weight, waist circumference, BMI), associated comorbidities, such as hypertension and dyslipidemia, and laboratory parameters to assess glycaemic control status, such as FBS and HBA1C levels. The second part of the questionnaire assessed peripheral neuropathy by Michigan Neuropathy Screening Instrument (MNSI) [11], a simple and validated screening tool for diabetic peripheral neuropathy (DPN). The MNSI is designed to be used in an outpatient setting by primary care or other providers. It consists of two steps: the history questionnaire and the physical assessment. The history questionnaire assesses the presence of neuropathic symptoms. This part consists of a total of 15 items: (13) items assessed symptoms of DPN, item number (4) assessed peripheral vascular disease (PVD), and item number (10) assessed general asthenia. The score ranges from 0 to 13 points, and a score that is ≥ 7 indicates the presence of neuropathic symptoms. The second part of the MNSI is a brief physical examination involving 1) inspection of the feet for deformities, dry skin, hair, or nail abnormalities, callous, or infection; 2) semi-quantitative assessment of vibration sensation using a tuning fork at the dorsum of the great toe; 3) grading of ankle reflexes; and 4) monofilament testing. Patients screening positive on the clinical portion of the MNSI (greater than or equal to 2.5 points on a 10-point scale) were considered to have peripheral neuropathy and were classified as having high-risk feet. The physical assessment was performed by one of the investigators who were trained in performing it.
The subjects found to have foot problems were then classified according to The International Working Group on Diabetic Foot (IWGDF) Risk Classification System [12]. Health education regarding foot care practices was imparted to all the subjects. Subjects found to be in category 1 or 2 were managed at the health facility, and subjects with category 3 risk were referred to the Department of Endocrinology, PGIMER, Chandigarh for further evaluation and management.
STATISTICAL ANALYSIS
The collected data were tabulated and analyzed using SPSS (Statistical Package for Social Sciences) V.18.0 software for Windows. The data were cross checked for data entry errors. Findings were described in terms of proportions and their 95% confidence intervals. Continuous data were summarized using the mean and standard deviation or median and interquartile range depending on the skewness of the data. A chi-square test was applied to find the association, and a p-value < 0.05 was considered statistically significant.
ETHICAL CONSIDERATIONS
The study did not involve any potential risks to the participants. The participants were screened for peripheral neuropathy using a non-invasive screening instrument, and the screening helped in its timely diagnosis and management to prevent patients from developing diabetic foot ulcers and amputation and to help improve their quality of life. The data collected from the participants were kept confidential, and the study protocol was approved by the Institute Ethical Committee (IEC), PGIMER, Chandigarh (Vide letter No. PGI/IEC/233/18).
RESULTS
The study included a total of 100 consecutive type 2 diabetes patients aged 31 to 85 years with a mean age of 59.76 years (SD = 19.82). More than half (58.0%) of the participants were females, 41.0% were unemployed/retired and 73.0% were found to be physically inactive. The mean BMI of the study participants was 33.2 kg/m2 (SD = 7.63). The mean duration of diabetes was 9.24 years (SD=3.45 years); almost half of the participants had diabetes for more than 10 years, and only 34.0% had controlled diabetes. Microvascular complications in the form of retinopathy and nephropathy were present in 6.0 and 12.0%, respectively. The majority (56.0%) of the study subjects had dyslipidemia. Moreover, 24.0% and 78.0% had cardiovascular disease and uncontrolled blood pressure, respectively (Table 1).
Table 1. Sociodemographic, clinical and laboratory characteristics of the study participants and their association with the presence of DPN (N=100)
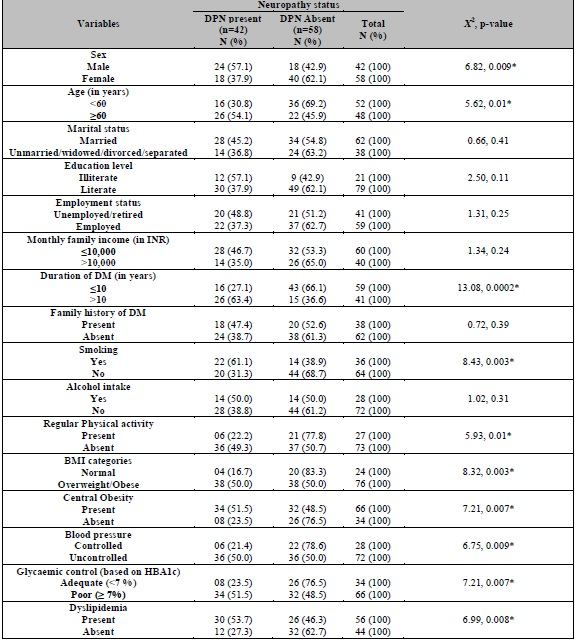
DM: Diabetes mellitus; DPN: Diabetic peripheral neuropathy; *statistically significant.
PREVALENCE OF DPN
The overall prevalence of DPN among study participants based on the MNSI score was 42.0% (Table 2). Based on the MNSI assessment, 46.0 and 42.0% of study participants had a score of ≥ 7 in the history questionnaire and a score of ≥ 2.5 in the physical examination section of the MNSI, respectively. Of those detected with DPN based on a cut-off score of 2.5 on physical assessment (42 patients), 97.6% had a score of ≥ 7 in the history questionnaire of the MNSI, whereas out of 46 patients scoring ≥ 7 in the history questionnaire, 89.1% had a score of 2.5 or above on physical assessment.
Table 2. Scores of the study participants based on history and physical assessment by MNSI questionnaire (N=100)

MNSI: Michigan Neuropathy Screening Instrument.
The history questionnaire of the MNSI assessment showed that most of the participants had at least one of the symptoms of DPN. The most frequently reported symptoms in DPN patients were numbness and pain with walking, which was present in 81.0% and 74.0% of study participants, respectively, while the least frequently reported symptoms were and loss of sensation in legs/feet while walking and history of one or more toes amputation, which was present in 16.0% and 2.0% of patients, respectively (Table 3).
DISCUSSION
Around 42.0% of type 2 diabetic patients were found to suffer from peripheral neuropathy in our study. This is similar to the findings of other studies on diabetic peripheral neuropathy (DPN) [10, 13-16]. However, this contrasted with the findings of Kaewput et al. [17] and Perrin et al. [18], in which the prevalence ranged from 3.0% to 16.6%. The possible reasons for this difference could be different study settings and different classification systems used to diagnose DPN in these studies. The prevalence of DPN found in the present study was lower than that found in studies conducted by Yang Q et al. [19] and Qin L et al. [20], in which the prevalence of DPN was close to 71.0% and 80.0%, respectively, due to similar reasons as they used the neuropathy symptom score (NSS) and neuropathy disability score (NDS) to assess DPN in their study population. A high prevalence of DPN is a matter of concern for clinicians and public health specialists working with diabetic patients, as this may lead to ulceration, amputation, life-long disability, and poor quality of life [21]. DPN can also increase the risks of future cardiovascular events and the associated mortality [22].
In the present study, it was found that the prevalence of DPN was significantly higher among males than females. This was similar to the results of some other studies [15, 17] but different from the findings of Sendi RA et al. [14], who observed no gender difference in DPN prevalence. The higher prevalence of DPN among males in our study could be due to the fact that health-seeking behavior among women is poor in most of the developing countries and hence have a lower chance of being detected with DPN, especially in rural areas.
Being older (Age ≥ 60 years) was found to be significantly associated with the presence of DPN in the study. This was in line with the observations of other authors [14, 15, 20]. As age advances, nerve function deteriorates, even in the absence of DM. With increasing life expectancy, the population of the elderly is bound to increase due to the demographic transition, and the prevalence of non-communicable diseases is also on rise as a result of the epidemiological transition occurring in India. Their concurrent occurrence complicated by complications of NCDs such as diabetes is worrisome.
The prevalence of DPN was also found to be higher among DM patients who had diabetes for more than 10 years in our study. This was in line with the results of previous studies [13, 14, 17, 20]. As the duration of DM increases, the risk of complications advances and this accelerates if glycemic control is also poor. This was supported by the findings of the present study in which patients with poor glycemic control were found to have a higher prevalence of DPN, similar to findings by other studies [10, 14, 15, 20, 23].
Smoking was also found to be associated with DPN, with a higher percentage of smokers having detected with DPN compared to non-smokers. This was similar to the findings of a study by Van der Velde et al. [23], in which smoking was found to be associated with reduced nerve function. Smoking causes atherosclerosis, elevates blood pressure, and causes nerve injury due to inflammation, which collectively leads to impaired nerve functioning.
Uncontrolled blood pressure and dyslipidemia were also found to be more prevalent in diabetic patients suffering from DPN. This was similar to findings from some other studies [14, 15]. In another study, DPN was found to be associated with elevated systolic blood pressure and problems in the management of hypertension among patients with type 2 DM [24]. This finding needs further exploration, as the exact mechanism behind the coexistence of DPN and uncontrolled blood pressure is still not completely known. The cause-effect studies could help in better understanding this interaction.
Obesity was another modifiable factor that was found to be associated with the presence of DPN in the present study. This was in line with findings of other studies conducted globally [15]. DPN originating among DM patients cannot solely be attributed to increased blood sugar levels but to the complex interplay of increasing age, deranged lipid profile, obesity, and hypertension [25].
CONCLUSIONS
The prevalence of diabetic peripheral neuropathy (DPN) is alarmingly high among patients with T2DM from rural northern India. Early detection and appropriate intervention are mandatory among patients with male gender, long-standing DM, higher BMI, central obesity, advancing age, dyslipidemia, uncontrolled hypertension, and poor glycemic control. There is a need for essential screening for early detection of neuropathic complications in patients with type 2 diabetes at primary and secondary levels of care.
COMPLIANCE WITH ETHICAL STANDARDS
Approval was sought from the Institutional Ethics Committee (IEC) of Postgraduate Institute of Medical Sciences & Research (PGIMER), Chandigarh before commencement of the study. During the study, informed written consent was obtained from all participants after clearly explaining the study objectives in a language known to them. If the participant was unable to read/write, informed consent was obtained from a Legally Authorized representative or next of kin.
ETHICAL APPROVAL AND INFORMED CONSENT
Prior to the commencement of the study, the study protocol was submitted for approval to the Institutional Ethics Committee (IEC) of Postgraduate Institute of Medical Sciences & Research (PGIMER), Chandigarh. Thereafter, permission was obtained from the Senior Medical Officer of the concerned hospital for conduction of the study. Study objectives were clearly explained to the participants in a language familiar to them. Anonymity and discretion of the information given by the patients were maintained with utmost care, and written informed consent was obtained from the participants.

