










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Despite a higher survival rate, 50% of preterm low birth weight (LBW) babies in particular are reported to have developmental problems at later ages, including motor, cognitive, and behavioural disorders [1]. Brain damage that may occur in preterm children and its impact on neurodevelopment is assessed by classifying this patient population into specific subgroups. There are two accepted valid classifications. These;
According to the United States of America data, preterm births account for 1-5% of all live births, and this rate is increasing day by day [4]. Because preterm babies are born at a critical time when their brain structure is not fully developed, 25-50% of these babies have psychiatric problems, including neurodevelopmental disorders, socialization problems, and attention deficits [5, 6, 7].
Our aim was to evaluate the cognitive functions of preterm children according to the week of gestation by comparing the scores of the Wechsler Intelligence Scale for Children-Enhanced Form (WISC-R) in childhood with this study.
MATERIAL AND METHODS
This prospective study was conducted in 2011 between May 2011 and September 2011 at Istanbul University-Cerrahpasa, Cerrahpasa school of Medicine Department of Pediatrics. The ethical Committee approval was obtained from the local ethics committee for the conduct of the study (based on Resolution No. 16405 of the Ethics Committee of the Medical Faculty of our university dated May 9, 2011).
The study included children with a history of preterm birth who were hospitalized in the neonatal intensive care unit (NICU) of the center of the study between 1998 and 2004 because of intraventricular hemorrage, patent ductus arteriom (PDA), bronchpulmonary dysplasia, fetal hydrothorax, necrotising enterocolitis, meconium aspiration and diaphragm hernia. The eligibility criteria for the research were birth between 27-36 weeks and age 6-13 years.
The parents were reached by telephone. Parents were informed of the procedures associated with the study, and the children of parents who agreed to these conditions were included as 'volunteers' in the research sample. After this interview, families were asked to complete a demographic data form. Families were informed of the results of the applied tests after the calculations had been performed.
The children of the families who met the inclusion criteria and agreed to participate voluntarily formed the case group. One hundred seventy-five children were included in the study.
The control group was consisted of children of the same age and sex with the case group chosen from a local primary school. They were reported as term children, and their families gave a written consent to participate in the study. The inclusion criteria for the control group was to be born preterm and not received any psychiatric diagnosis until the time of the study. The exclusion criteria was to be born preterm and have become the diagnosis of any psychiatric disease at any time of their lifespan.
Exclusion criteria: Children with severe neurological sequelae, blindness, deafness, and children whose parents refused to participate in the study were not included.
THE WECHSLER INTELLIGENCE SCALE-ENHANCED FORM FOR CHILDREN (WISC-R)
The Wechsler Intelligence Scale-Enhanced Form for Children (WISC-R) test was administered to children participating in the study to evaluate cognitive functions by psychologists [8].The age range in which this test can be used is between 6 and 16 years. The standardization study of the WISC-R was conducted by Savaşır and Şahin [9] on a sample of 1639 children selected from 11 urban centers in our country and adapted to Turkish culture. The WISC-R consists of a total of 10 subtests and 2 backup tests, namely 6 verbal subtests (general knowledge, similarities, arithmetic, comprehension, vocabulary, number sequence) and 6 performance subtests (picture completion, picture editing, pattern with cubes, piece assembling, password, labyrinth). In addition to the standard scores for these subtests, verbal intelligence departments (IQ), performance IQ and total IQ coefficients are also obtained. In our country, the scale was found to provide reliable and valid results in both the clinical sample [10] and the normal sample [11]. The mean value for these ZB coefficients is 100 and the standard deviation is 15. The mean of the standard values obtained for each subtest is 10 and the standard deviation is 3.
All the children (preterm group and the control group) participating in the study were examined by child psychiatrists to complete the K-SADS, and the CBCL scales, under clinic conditions. In addition, clinical psychologists administered the WISC-R test to these patients to evaluate cognitive functions.
SCHEDULE FOR AFFECTIVE DISORDERS AND SCHIZOPHRENIA FOR SCHOOL-AGE CHILDREN PRESENT AND LIFETIME VERSION (K-SADS-PL)
This semi-structured interview was administered to all adolescents and their parents by a child and adolescent psychiatrist to determine depressive and anxiety disorders and comorbid psychiatric disorder in the control group. K-SADS-PL is a valid and reliable instrument for Turkish children and adolescents [12].
CHILD BEHAVIOR CHECKLIST FOR AGES 6-48 YEARS (CBCL 6-18)
This parent-rated CBCL provided information on the index subject's behaviors in the past 6 months (0–2) grouped under subscales. The reliability and validity of the Turkish version of CBCL 6-18 is well established [13].
EXPECTED OUTCOMES
To determine the frequency of behavioural and psychopathological problems in preterm and low birth weight children followed up in our Intensive Care Unit (ICU),
To evaluate cognitive functions,
To determine a possible association between the psychiatric disorders detected and the events and morbidities that occurred during the prenatal and postnatal process (such as preeclampsia, multiple pregnancy, use of assisted reproductive techniques, intraventricular hemorrage, sepsis, necrotisan enterocolitis).
STATISTICAL ANALYSIS
The collected data were analysed using SPSS 21.0 software. Numbers, percentages, and averages were given in the list of data, and data were analysed using the Mann-Whitney U test and chi-square tests when appropriate. The Shapiro-Wilk test was used for normality tests and it was observed that the normality assumption was met. Independent samples t-test was used to detect differences between groups, and Pearson correlation tests were used for correlation between continuous variables. A p-value of < 0.05 was considered statistically significant at the statistical significance level.
RESULTS
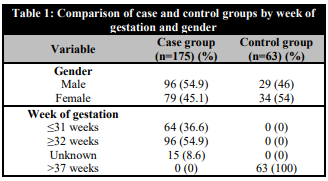
Two hundred thirty-eight children were enrolled in the study. One hundred seventy-five children (54.9% male) formed the case group and 63 children formed the control group. When the case group was examined by gestational age, 36.6% were born at less than 31 weeks (extremely preterm), 32% were born between 32 and 35 weeks (moderately preterm), 22.9% were born between 36 and 37 weeks (borderline preterm), and 8.6% were preterm and born at an unknown week. All in the control group were born at term (Table 1). The problems preterm babies face in the neonatal period are summarized in Table 2. Rates of mechanical ventilation, steroid use, and surfactant use were statistically higher in preterm babies ≥32 weeks and above. There were no significant differences between groups in terms of other risk factors.

A comparison of the WISC-R scores of the case and control groups showed that the WISC-R Verbal Score and WISC-R Total Score were statistically significant between the case and control groups, whereas the WISC-R Performance Score and age were not statistically significant (Table 3).

When analysed by gestational age, no statistical significance was found between the WISC-R Verbal, WISC-R Performance, and WISC-R Total scores as a function of gestational age (Table 4).

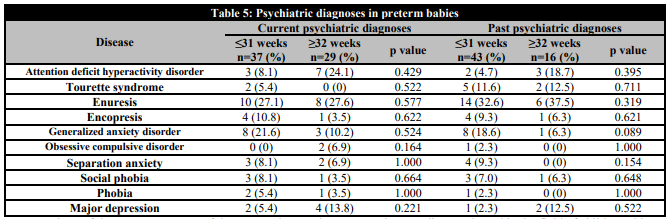
No statistically significant difference was found between previous and current psychiatric diagnoses compared with week of birth for preterm babies. The most common psychiatric diagnoses in preterm babies were enuresis and generalized anxiety disorder (Table 5).
DISCUSSION
Ensuring that preterm babies have lower morbidity, higher functionality, and participate in society as healthy individuals in the long term is an important public health issue. Cognitive function is also among the issues that form the cornerstone of functionality in this sense. In addition, it is very important to identify and find solutions to neurodevelopmental problems that may develop with close observation. In developed countries, preterm babies are regularly monitored after discharge with a multidisciplinary approach (pediatrician, neurologist, physiotherapist, psychologist, psychiatrist, etc.) and general health problems affecting development, including neurodevelopmental areas, are identified so that these children have the chance to adapt to society and become healthy individuals. Therefore, there are many studies in the literature with long-term results on neurodevelopmental monitoring published in developed countries [11]. However, the data from our country are limited. The reason that led us to conduct research on this topic was to follow the social developments by evaluating the cognitive functions of preterm babies in our country.
In previous studies conducted in the field of child psychiatry in our country, it was found that there were more male cases (> 60%) [14, 15, 16, 17, 18, 19]. Tanrıöver et al. [14] based this on the fact that more boys are brought to the child and adolescent mental health and illness outpatient clinics. Although boys were more common in our study sample, the gender distribution was narrower than in other studies (male case rate 54.9%). The reason could be that the sample consisted of volunteers and that families with preterm babies are more sensitive about the follow-up of their children.
Functions such as attention, visual differentiation, serial memory performance, and visual-motor coordination are defined as cognitive functions. In a study that investigated the cognitive functions of preterm babies during childhood, it was found that these children fell significantly behind only in serial memory performance [20]. There are different opinions in different studies. Two studies similar to ours reported that preterm children scored significantly lower in intelligence than controls but still within normal limits, which is consistent with the fact that negative cognitive outcomes are more common in extremely preterm babies [21, 22].
It has been observed that the interaction of premature children with developmental risks, especially in the area of language, with the caregiver/people in their home environment, is effective in addressing developmental delays or risks because of premature birth [23]. In a study conducted in the Netherlands, neurological assessment was the best determinant of cognitive development in infants at one year of age, while home environment assessment along with neurological assessment was the best determinant of cognitive development in ELBW babies at two years of age. This study showed that children aged 12-42 months were able to catch up with a cognitive delay when provided with a stimulating home environment [24]. The association between home environment and cognitive function was not examined in our study.
In the study conducted by Arhan et al. in our country [25], it was found that the preterm group performed worse in the verbal and material ability scales compared with the control children, performed similarly poorly in the attention, and reasoning functioning scales, which is consistent with previous reports [26, 27, 28].
The WISC-R subtest scores showed that preterm children lagged far behind term children in general knowledge, language skills, processing speed, and working memory. Our study findings were similar to those of a follow-up study conducted with preterm babies by Fedrizzi et al. In that study, it was found that there were no differences in general knowledge, verbal, and performance subtests in low-risk preterm babies at age 7 years [29]. When comparing the WISC-R score, which was used to evaluate cognitive function in our study, no statistical significance was found between the preterm groups according to the week of gestation. However, comparison of the WISC-R scores of the case and control groups revealed that the WISC-R Verbal Score and WISC-R Complete Score were statistically significantly higher in the case group.
When the psychiatric diagnoses of the preterm babies who formed the study group were compared, no difference was found between the two groups because the week of birth was taken into account. In studies conducted in our country, the most common diagnoses were MBD, mental disability, and anxiety disorders [19, 30, 31, 32]. In the study by Sevgen et al. [33], children aged 0-5 years were studied. The most common diagnoses were stimulus deficiency, adjustment disorder, autism spectrum disorder, global developmental delay (GDD), attention deficit hyperactivity disorder (MBD), stuttering, abstinence disorder, limit-setting problem, articulation disorder, oppositional defiant disorder, and separation anxiety. It was also found that enuresis and anxiety disorder was the most common psychiatric diagnoses in our study.
In the study conducted by Çak Esen et al. [34] at Hacettepe University, attention deficit hyperactivity disorder and its associated prenatal risk factors were investigated in preterm children. The results of this study showed that children diagnosed with attention deficit hyperactivity disorder had a smaller birth week and birth weight, that these children were more likely to suffer from respiratory distress syndrome,. In addition, it was also observed an increased history of surfactant and mechanical ventilation therapy, a longer hospital stay in the neonatal period, and that they came from a family with a high socioeconomic level, which was associated with a lower number of diagnoses of attention deficit hyperactivity disorder. It was determined that the variable most strongly associated with a diagnosis of attention deficit hyperactivity disorder among all factors was week of gestation. In our study, the comparison between groups was made only by week of gestation and not by psychiatric diagnoses.
As a result, the WISC-R score, although not different for classification of preterm babies, was statistically significantly higher in the case group than in the term group. This situation differs from reports in the literature that preterm babies have a lower WISC-R score and indicates the need to investigate this situation through further studies and even with other tests.
STUDY LIMITATIONS
Our study, which was a single-center study, included only children born to families who consented to the study. The families who consented to participate in the study were aware families, which may generate bias. Only preterm children were evaluated with the WISC-R score in our study because of time and staff limitations. Studies can be planned to include more cognitive function tests and sociodemographic information about families.

