










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Obesity is a global problem in public health. The World Health Organization (WHO) showed in 2014 that 39% of the adult world population had overweight and 13%, obesity 1. Currently, obesity is considered as an epidemiological emergency in Mexico 2,3. The prevalence of overweight and obesity in adults increased and body fat excess is responsible for heart disease, cerebrovascular events, diabetes mellitus, ulcers, retinopathy, renal failure, peripheral vascular disease, osteoarthritis and cancer 4,5,6,7. Iodine deficiency induced hypothyroidism, making the thyroid unable to produce enough hormones to maintain the normal metabolism of the body 8,9,10. Adipose tissue from rats express the mRNA of sodium/iodide symporter (NIS), and iodine can be stored in fat tissue 11,12. However, the role of iodine per se in obesity is unknown. Previous studies report an antioxidant role of iodine in extrathyroid tissues that concentrate iodine; for example, iodine-deficient rats exposed to potassium iodide increase a total antioxidant in the retina 13. In vivo studies show an increase of enzymatic activity as glutathione peroxidase in patients after drinking cures with iodine brine 14. In contrast, total antioxidant status (TAS) is low in pregnant women with iodine deficiency, while oxidative stress increases 15. Iodine is part of the T3 hormone, which participates in the regulation of temperature homeostasis and is responsible for almost 30% of resting energy expenditure. Previous studies have shown a correlation between thyroid hormones and changes in weight in chickens 16. Recently, it has been shown that thyroid hormones may access the arcuate nucleus and hypothalamus to regulate appetite 17, and hypothyroidism induces reduced basal energy expenditure with weight gain 10,18. However, thyroid hormone levels are inconsistent in obese adults 19,20,21,22.
Obesity is a chronic inflammatory process characterized by an increase of adipose tissue, which modifies serum levels of adipokines as leptin, adiponectin and ILs. Adiponectin is a hormone secreted in the adipose tissue which circulates in healthy subjects in concentrations ranging from 5 to 30 μg/ml. This hormone regulates the metabolism energy by stimulating the oxidation of fatty acids and decreasing plasma triglyceride levels; it also improves glucose metabolism, increases insulin sensitivity and inhibits early phases of atherosclerosis 23,24,25). Meanwhile, cytokines of the IL-1 family have been described to be elevated in obese adults. This family includes, among others, IL-1α, IL-1β, IL-1 receptor antagonist (IL-1ra) and IL-18 26,27. The IL-1ra binds to the IL-1 receptor competing with the proinflammatory IL-1 and were shown to be elevated in obese adults, indicating anti-inflammatory function 28. However, there are no data related to levels of adiponectin, IL-1, oxidative stress and ioduria with BMI in healthy adult population. This study was done to establish a possible association between these variables.
METHODS
DESIGN AND ANTHROPOMORPHIC PARAMETERS
A cross sectional study was carried out in users of the healthy life unit (UVISA) from Xalapa, Veracruz, Mexico. The UVISA is a unique institution at a national level, which addresses health care in a comprehensive way through the promotion of healthy lifestyles. The study was approved ethically by the UVISA Ethics Committee, the Bioethical Committee of the Health Institute of the University of Veracruz, from Teaching, Research and Training of the Department of Postgraduate and Research of the Secretary of Health of the State of Veracruz, Mexico, and complies with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. Each user signed an informed consent letter and questionnaires were applied in order to known the sociodemographic (sex, age, school level and employment) and clinical characteristics. The subjects with morbid obesity, degenerative chronic disease, pregnant and pharmacological treatment were excluded from this study. Blood samples were drawn from October 2016 to November 2016 in UVISA from Xalapa, Veracruz. Five milliliters of fasting venous blood were collected in a BD vacutainer; they were preserved using packs of ice blocks and were later transported to the laboratory. The blood samples were centrifuged at 5,000 rpm for five minutes to separate plasma. The layer of white blood cells above the packed erythrocytes was discarded. The erythrocyte pellets were washed three times with 0.15 HCL, diluted in 33% of phosphate buffer saline (mM; NaCl, 136.9; KCl, 2.68; KH2PO4,1 .47; Na2 HPO4, 6.62; and pH 7.4), and kept at 4 °C until use. Similarly, urine samples of 24 hours were preserved in frozen-capped plastic tubes with 20% of formalin to minimize iodine volatilization; then, they were frozen and analyzed. All blood samples were preserved in refrigerator. Body mass index (BMI) was calculated by dividing body weight in kilograms by height in square meters (BMI = kg/m2).
Anthropomorphic parameters showed that 47 had normal weight, of which 12.5% were men and 87.5% were women.
BIOCHEMICAL MEASUREMENT
Levels of adiponectin (Abcam® Human, United Kingdom), IL-1 (Sigma-Aldrich®, México) were measured by immune-enzymatic assays in a spectrophotometer at 450 nm. Plasma TBARs were measured fluorometrically using a Quantichrom(tm) TBARS Assay Kit. Serum TBARS are reported as µmol/l (Bioassay System). TAS was measured colorimetrically as reported 29, and hemoglobin, by the method previously described (Cable RG). Urinary iodine concentration (UIC) was obtained using a fast colorimetric method 2,15. Briefly, 0.2 ml of urine or iodine calibrator (50-300 μg/l) and 1.0 ml of ammonium persulfate solution were heated for one hour at 100 °C, after adding arsenious acid solution (10 g of As2C3, 50 g of NaCl, 400 ml of 2.5 mol/l H2SO4) to each tube. Then, fresh ferroin-arsenic acid solution (10.8 mol/l H2SO4, arsenious acid, 200 g/l sodium chloride, and 2 ml ferroin) was added. Finally, ceric ammonium sulfate solution was added with the multipipetter, and the content of each glass tube (150 μl) was then transferred to a sterile polystyrene microtiter plate, and iodine was determined by the rate of color disappearance at 504 nm of each well in a microplate reader (SpectraMax(r) Plus; Molecular Devices, Sunnyvale, CA). The UIC was determined by subtracting the OD of the blanks and is expressed as μg/l against a standard iodine concentration (50-300 μg/l).
STATISTICAL ANALYSIS
Data obtained from 114 users were analyzed statistically using SPSS 17 for Windows (SPSS Inc., Chicago, IL). The data were expressed as frequency, percentage and means ± SD. Kolmogorov-Smirnov o Shapiro Wilk tests were used to know the sample distribution. The Student's t-test and ANOVA test were used to compare the continuous variables with normal distribution in two or more independent groups, whereas the Mann-Whitney U test was used for continuous variables with non-Gaussian distribution. Differences with p < 0.05 were considered as significant. Correlation test between adiponectin, interleukin-1, oxidative stress and ioduria with BMI were done with Spearman's correlation test with SPSS and p < 0.05 were considered as significant.
RESULTS
ANTHROPOMORPHIC AND SOCIODEMOGRAPHIC CHARACTERISTICS
A total of 121 subjects entered the study, of which seven were eliminated due to lack of biological samples; 114 individuals were finally included, 33 men and 81 women. Table 1 presents data concerning sociodemographic characteristics of subjects. The average age was 32.03 ± 6.72 years, between 25 and 44 years. The average ages of men and women were 28.94 ± 4.44 and 33.28 ± 7.10, respectively.
Table I. Anthropomorphic and sociodemographic characteristics by sex
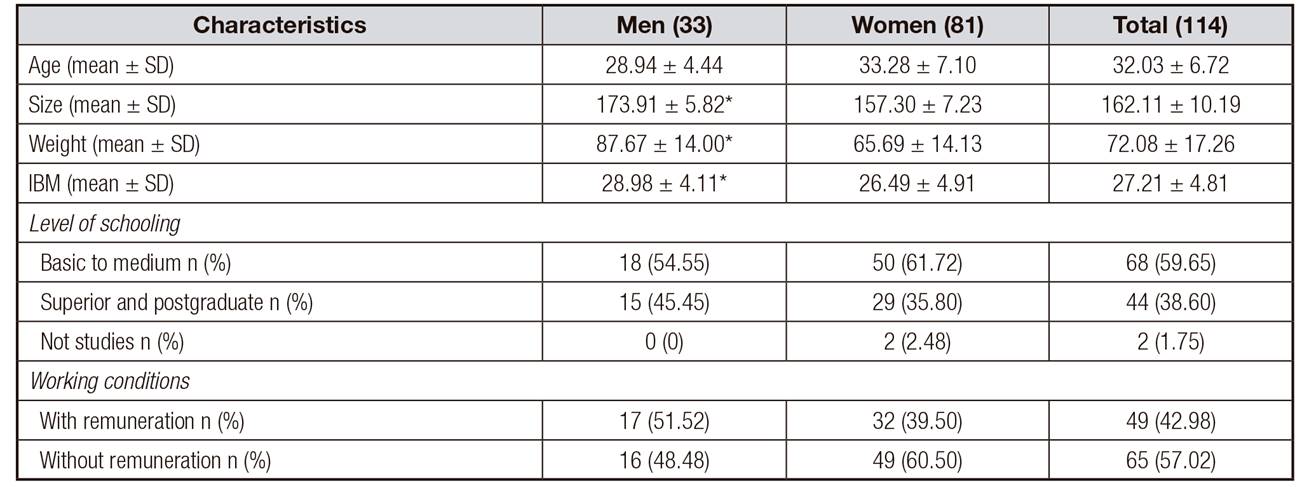
SD: standard deviation; BMI: body mass index. Age is expressed in years; size, in cm; and weight, in kg. Level of significance
*p < 0.05, for both sexes.
Anthropomorphic parameters showed that 35.1% had normal weight, of which 12.5% were men and 97.5% were women. The remaining 64.9% of subjects were found to be overweight and obese. Of these, 45 (39.5%) were overweight (33.3% were men and 66.6%, women). The remaining 29 subjects were obese (males 44.8% and females 55.2%).

ADIPONECTIN, IL-1, UIC, TAS AND OXIDATIVE STRESS ARE ASSOCIATED WITH THE INCREASE OF BMI
Table II shows the concentration of circulating adiponectin levels for all samples 24.12 ± 6.23 μg/ml. A significant decrease in adiponectin levels between normal weight with overweight and obesity was found (p = 0.05 and 0.01, respectively). In contrast, a significant increase in IL-1, TBARS and TAS levels was found between overweight and obesity as compared to normal weight. In addition, overweight and obese subjects presented significant lower levels of UIC vs normal weight subjects. We have made an analysis of Spearman's correlation between BMI, with adiponectin, IL-1, UIC, TAS and TBARS which is shown in Table 3. A significant (p = 0.001) negative correlation between adiponectin and obesity was observed, as well as a significant positive correlation between IL-1 with overweight (r = 0.287, p = 0.050) and obesity (r = 0.515, p = 0.006). When correlating MDA with BMI, there was a significant (r = 0.787, p < 0.008) positive correlation only with obesity, while a positive correlation between TAS with overweight and obesity was established (r = 0.398, p = 0.049, and r = 0.448, p = 0.030). However, a negative correlation was observed between UIC and obese subject. All sociodemographic variables were correlated with BMI and we found only a significant but negative correlation with both sexes (r = -0.530, p = 0.002) for males and (r = -0.457, p = 0.001) for females.

DISCUSSION
The study sample showed an adult population with a high proportion of individuals presenting body fat excess, and where more than a half of the women were obese. Previous studies have shown that prevalence of overweight is higher in men than in females, while obesity prevalence is higher in women than in men 2. On the other hand, we found that overweight and obese subjects have low levels of ioduria vs normal weight subjects. Although there are few studies in obese subjects, it has been reported that ioduria is significantly lower in obese that in non-obese subjects 30. In addition, obese women showed a significantly low urinary iodine concentration in comparison with non-obese women 9. In another vulnerable group as pregnant women, iodine levels were below WHO recommendations 15,29,31, and in patients with diabetes mellitus type 2 decreased levels of iodine were found 32. These studies suggest that iodine deficiency is present in overweight and obesity, but further studies are required to confirm this data.
On the other hand, it has been reported that doses of iodide at similar levels as human breast milk decrease the expression of mRNA adiponectin levels, although doses of normal serum levels did not affect adiponectin levels 33. In this study, we found that overweight and obese subjects have lower iodine and adiponectin levels in comparison with normal weight subjects. This suggests that iodine could be contributing to the low production of adiponectin. Accordingly, an association between adiponectin decrease and iodine concentration in obese women vs no obese has been reported 34. Also, other studies have shown a decrease of adiponectin levels associated with the increase of BMI 23,24,25,34. Little is known about the association between iodine and overweight and obesity; however, in thyroid FRTL cells it was demonstrated that the administration of inflammatory cytokines as IL-6 and IL-1beta induced a 30% decrease of NIS RNA levels and IL-1beta suppressed iodide transport in approximately 25% 11,35. In this study we found an increase of markers of inflammation such as IL-1 and ROS, and also low levels of iodine in subjects with overweight and obesity. This suggest that IL-1 could affect the expression of the sodium/iodine symporter (NIS), contributing in low iodine levels in overweight and obese subjects, although this hypothesis needs to be demonstrated.
The antioxidant effects of iodine have been reported previously; for example, an antioxidant increase in the retina was found in iodine deficient rats exposed to potassium iodide 13. Clinical studies carried out in patients with diabetes mellitus type II showed an increase in the enzymatic activity of catalase and glutathione peroxidase after drinking brines with iodine 14. In rats intoxicated with alloxan monohydrate to induce diabetes, iodine treatment increased catalase and superoxide dismutase activities 36. In contrast, an increase of oxidative stress has been found in hypertensive women with iodine deficiency 15,29. Obesity is an inflammatory process characterized by an increase of oxidative stress. In this study, it was corroborated that obese subjects present a significant increase of oxidative stress and TAS vs overweight and normal weight subjects. In addition, a significant correlation between obesity and oxidative stress was found, although the increase of TAS was associated with overweight and obese subjects. The activation of these antioxidant enzymes in overweight and obese subjects may be to counteract the effect of oxidative stress generated by ROS. It would be interesting to analyze the prophylaxis with iodine, its effects on the REDOX status, and inflammatory markers in subjects with obesity.
Various limitations in this study could affect the results. One of these limitations is that subjects practice healthy lifestyles. This could be altering the values of IL-1, adiponectin, TAS and ROS. Another limitation is that the sample involved men and women and this hormonal condition could be associated with BMI. Another limitation is the lack of thyroid stimulating hormone (TSH) and T3 measurement to corroborate the pathological effects of iodine deficiency.
In conclusion, the current study provides novel evidence that BMI is associated with the increase of oxidative stress, IL-1 and decrease of TAS, adiponectin and ioduria. The association of ioduria levels with BMI and with the balance of the reduced and oxidized species requires further studies. All these data suggest the role of iodine and ROS in the etiopathogenesis of chronic disease related to the increase of BMI. It would be interesting to study iodine prophylaxis to determine its effects on overweight and obesity subjects.

