










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Physical fitness could be defined as the ability to perform not only various aspects of sports but also occupational and regular daily activities. Numerous studies have identified it as an important marker of health and well-being both in childhood and in adulthood 1,2. Particularly, low level of physical fitness in childhood and adolescence is associated with future risk of chronic diseases such as cardiovascular disease or skeletal health and mental health disorders 3,4,5,6. As a consequence, assessment of physical fitness starting at the early childhood has been promoted particularly through the Physical Education curriculum not only as a tool to point out some limitations and weaknesses in physical performance but also as an efficient way to identify these potential health related risk factors 2.
Besides the cardiorespiratory fitness as the most frequently evaluated fitness component, in the last years numerous studies have identified other fitness components such as flexibility, muscular fitness and speed/agility as additional determinants of health and well-being 7. However, these monitoring strategies could only be fully efficient if associated with well-established age and gender normative values, which is also region/country-specific 8. This has led to presenting numerous datasets on physical fitness levels among children worldwide 1,2,9,10,11,12,13,14. However, although some of these studies have reported fitness levels aggregated from datasets collected in different regions, there is still a lack of reference values for schoolchildren from specific countries, which does not allow a correct evaluation and interpretation of the collected measurements of particular fitness components.
Other important determining risk factors that affect children's health are overweight and obesity 4,15,16,17,18. The increase in child obesity has been reported by the World Health Organization (WHO), arguing that the proportion of overweight and obese children in European countries is still increasing 19, but also that this trend varies from country to country 18,20. Nevertheless, further country-specific monitoring has been highlighted as important in order to both understand particular trends and changes in the occurrence of overweight and obesity and identify these factors which are mostly responsible for this worrisome trend 2,8,21.
Taking this into account, the aims of the present study were: a) to explore physical fitness levels of the Serbian nine to 14-year-old schoolchildren; (b) to report gender- and age-specific physical fitness levels of Serbian schoolchildren; and c) to estimate the prevalence of overweight and obesity at the national level. We expect that the obtained findings could support current efforts to improve not only the Physical Education curriculum in order to reduce obesity incidence in childhood, but also the development of more effective public health strategies.
MATERIAL AND METHODS
DESIGN AND PARTICIPANTS
The data for this study were collected as a part of a national cross-sectional school-based study aimed to construct nationally based health-related physical fitness standards. For the purpose of this study, 12,211 schoolchildren (boys n = 6,188 and girls n = 6,023), aged nine to 14 years, who at the time of the study attended elementary schools on the territory of the Republic of Serbia, were included. There are approximately 1,300 elementary schools in Serbia, and they are all divided into 18 school districts. The schools that were included (n = 98) were randomly selected from all school districts of the Republic Serbia and stratified by geographical location (urban and rural).
DATA COLLECTION
All data were collected during the spring semester of the 2012/13 school year. Selected schools agreed to participate in the study. All measurements were performed by physical education teachers who were specially trained for this purpose. The study was approved by the institutional review board of the Faculty of Sport and Physical Education, University of Belgrade, Serbia, and a signed consent form (by parent or legal guardian) was obtained prior to participation in the study.
MEASURES
Anthropometrical measurements
Body height (BH) was measured to the nearest 0.1 cm using a Seca(r) Stadiometer 208 (Seca(r), Hamburg, Germany). The subjects were barefoot, minimally dressed (shorts and T-shirts), and the head was positioned using the Frankfurt method (Frankfurt plane parallel to the floor). Body weight (BW) was measured to the nearest 0.1 kg using the pre-calibrated portable weighting scale Tanita(r) Inner Scan BC 587 (Tanita Europe GmbH, Sindelfingen, Germany). For estimating the prevalence of obesity, body mass index (BMI = weight/height2) was calculated. The international gender and age-specific BMI cut-off points for children developed by the Childhood Obesity Working Group of the International Obesity Task Force were used to define subjects as normal (optimal) weight, overweight or obese 22. These cut-off points were derived from a large international sample using regression techniques by passing a line through the health-related adult cut-off points for 18-year-old subjects (Cole et al., 2000). Children with BMI values that corresponded to an adult BMI under 25 were classified as normal-weight (NW), those whose BMI corresponded to an adult BMI between 25 and 30 were considered as overweight, and children with a BMI corresponding to an adult BMI of ≥ 30 were categorized as obese.
Physical fitness tests
The physical fitness battery was developed through the National Fitness Project of Serbia aimed to establish a standardized test battery for regular monitoring of health-related physical fitness of Serbian schoolchildren. The battery consists of six commonly used standardized field-based physical fitness tests for assessing flexibility (sit and reach test [S&R]), agility (4 x 10 m shuttle run [4 x 10 m]), muscular fitness (standing long jump [LJ], 30 sec sit-ups [SU] and bent arm hang [BAH]), and cardiorespiratory endurance (20-m shuttle run [SR]). All tests are described in more detail elsewhere 23.
STATISTICAL ANALYSIS
Descriptive statistics (mean, standard deviation) was calculated for all test outcomes separately by gender. The participants were divided into six age groups: 9 to 10, 10 to 11, 11 to 12, 12 to 13, 13 to 14 and 14 to 15 years and marked as 9, 10, 11, 12, 13 and 14, respectively. Two-factor ANOVAs were used separately for each test to explore potential differences in physical fitness level between boys and girls ("gender" factor) and different age ("age" factor). Additionally, a post-hoc analysis (t-test with Bonferroni) was performed for the tests where significant main effect of factor or their interactions were found. The level of significance was set to p < 0.05. Finally, the effects size was estimated via partial eta squared (ηp2) and, according to Cohen, it was considered as either small (0.01), medium (0.06) or large (0.15) (Cohen, 1988). All data were analyzed using SPSS 18.0 (SPSS Inc. Chicago, IL).
To provide percentile values separately for boys and girls, all components of physical fitness level were analyzed with the LMS statistical method (Cole et al., 2000). Smoothed centile charts were derived using the LMS method. This estimates the measurement centiles in terms of three gender-age specific cubic spline curves: the L curve (Box-Cox power to remove skewness), M curve (median) and S curve (coefficient of variation). The 5rd, 25th, 50th, 75th, and 95th smoothing percentiles were chosen as the gender and age-specific reference values. For the construction of the percentile curves, data were imported into the LmsChartMaker software (V. 2.3; 24,25)) and the L, M and S curves were estimated for all tests except for S&R and BAH, where centile values were calculated using standard procedures.
RESULTS
The overall descriptive statistics of all test results separated by gender are presented in Table 1.
Table I Descriptive statistic for anthropometric characteristics and physical fitness parameters sampled by sex
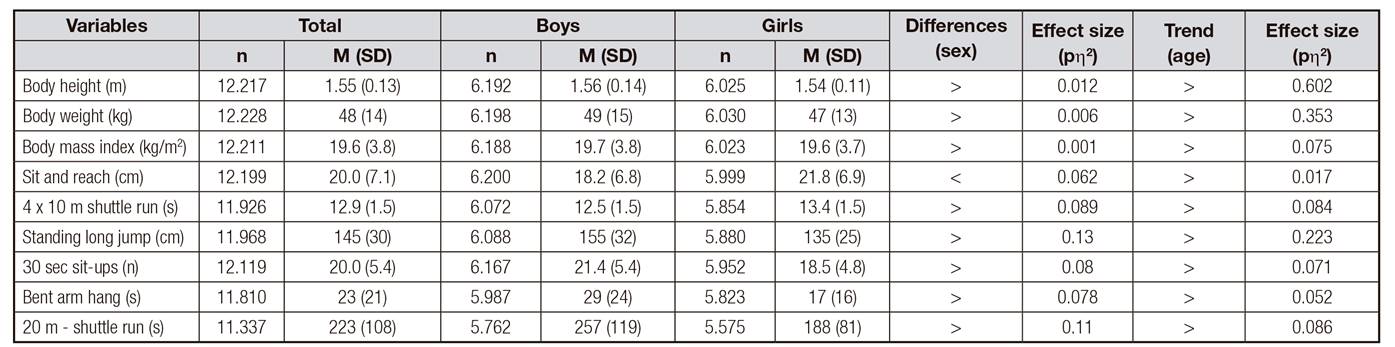
M (SD): mean (standard deviation); n: number; >: the variable is significantly (p < 0.05) higher in boys than in girls; <: the opposite; >: age trend.
Regarding physical fitness, both factors (gender and age) were significant for all tests due to higher physical fitness level in boys, except for the S&R test (ηp2 = 0.06), in which girls performed better. Test results separated by gender and age and expressed in percentiles from 5 to 95 are depicted on Figure 1.

Figure 1 Smoothed (LMS method) centile curves for anthropometric characteristic and physical fitness tests S&R, 4 x 10 m, LJ, SU, BAH and SR (from the bottom to the top: P5, P25, P50, P75, P95) among Serbian boys and girls of 9-14 years of age (BH: body height; BW: body weight; BMI: body mass index; S&R: sit and reach test; 4 x 10 m: 4 x 10 m shuttle run; LJ: standing long jump; SU: 30 sec sit-ups; BAH: bent arm hang; SR: 20-m shuttle run).
For all indices except for flexibility, within the same age groups, percentile curves indicated higher values in boys than in girls. In addition, an age-related incremental trend could be seen for almost all indices.
Table 2 shows gender- and age-specific reference values (P10, P20, P30, P40, P50, P60, P70, P80, P90 and P100) for the anthropometric characteristics and different fitness tests in Serbian schoolchildren. Centile values were estimated for the closest age; therefore, to compare someone's physical fitness level with the normative values from Table 2, data from the rows at the age closer to his/her current age (e.g., if eleven years and five months, look at eleven years) should be taken.
Table II Tabulated physical fitness centile values by sex and age for Serbian children
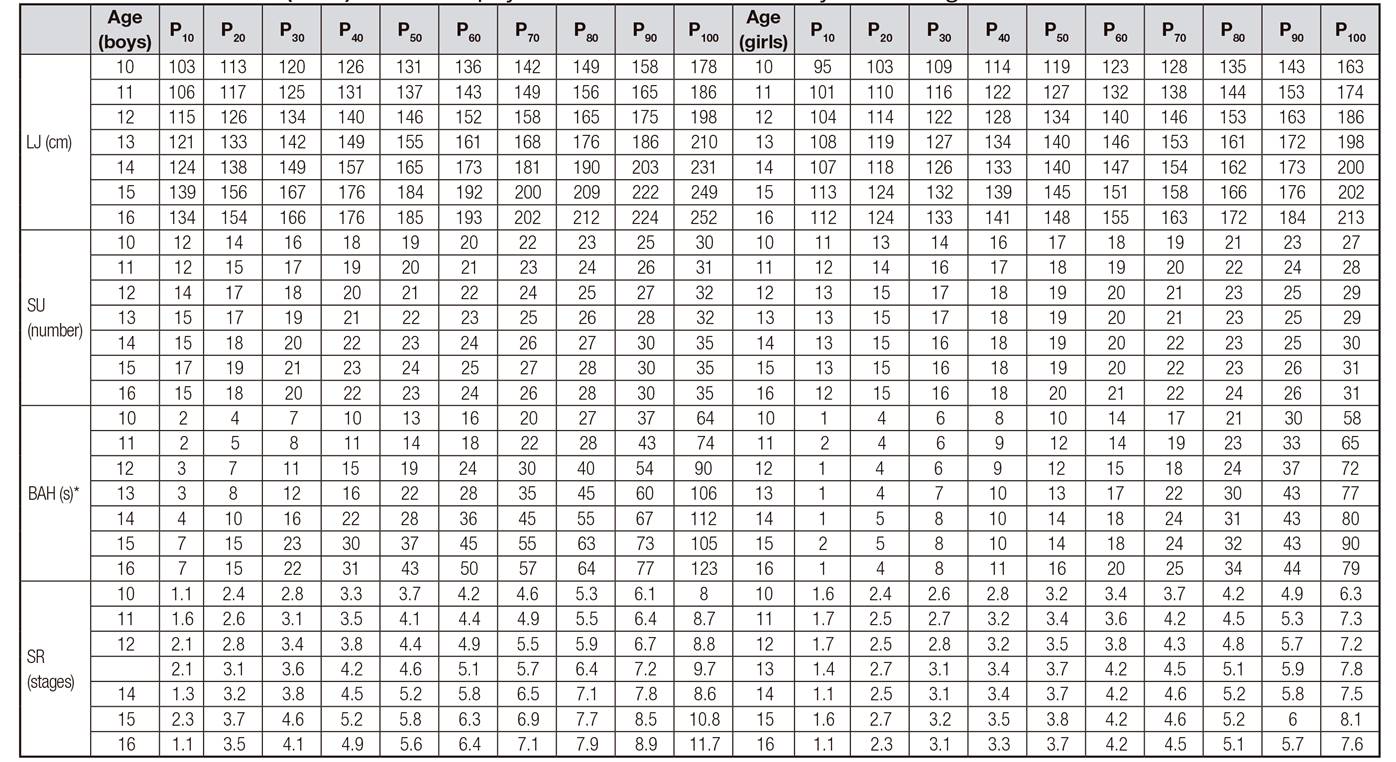
*The LMS method cannot be used when 0 values are observed. Since this is the case for this test, centile values were estimated using the standard procedure. BH: body height; BW: body weight; BMI: body mass index; S&R: sit and reach test; 4 x 10 m: 4 x 10 m shuttle run; LJ: standing long jump; SU: 30 sec sit-ups; BAH: bent arm hang; SR: 20-m shuttle run.
Results regarding prevalence of overweight and obesity of Serbian schoolchildren are in Figure 2. The boys had greater percent of overweight and obesity than girls in all age groups. The only exemption is percent of overweight at the age of nine, where the girls had a slightly higher percent (boys = 18.7%, girls = 20.7%). The results showed that schoolchildren at younger age groups (from nine to eleven) of both genders had higher prevalence of overweight and obesity than the older ones.

DISCUSSION
The aims of the current study were: a) to explore physical fitness levels of the Serbian nine to 14-year-old schoolchildren; b) to report gender- and age-specific physical fitness levels of Serbian schoolchildren; and c) to estimate the prevalence of overweight and obesity at a national level. To the best of our knowledge, this is the first research of this type performed on a representative sample consisting of schoolchildren from all school districts in the Republic Serbia and stratified by geographical location. This is the main strength of the current study since the findings obtained are not only relevant for getting a clear picture of the current state regarding fitness levels at a national level for the observed age groups, but it also allows a valid comparison of the fitness level of Serbian schoolchildren and their counterparts from different European countries (and worldwide).
Regarding the physical fitness level, the findings revealed higher scores in boys than in girls across all age groups in agility, lower- and upper-limb strength, hip flexor muscular endurance and cardiorespiratory endurance, and the only test that girls performed better was the one for flexibility. Furthermore, differences were found in all tests between consecutive age groups in both boys and girls as older children performed better than the younger ones. These results are consistent with most similar studies performed worldwide 1,6,21,26,27,28, and they were also expected since gender and age-related differences, particularly in cardiorespiratory and muscular fitness, could be attributed to normal development and growth 6,8.
Although physical fitness is well-known as an important health marker already in youth, which further highlights the need of meaningful and accurate physical fitness assessment in young people, consensus for applying unified standardized tests and protocols is still missing. This makes both comparisons of data from different studies and establishing unique gender and age-related reference values in order to assess someone's physical fitness level extremely difficult. Nevertheless, most of the tests applied in this study are identical to those applied in some major projects aimed to explore physical fitness levels in a number of European countries 1,6,26,28,29. Our findings are in line with those reported in recent studies from Poland 1, Greece 28 and findings presented in a large European epidemiological study (HELENA study) 29, where most of the same physical fitness tests were applied. Particularly, regarding the 4 x 10 m and SU, the median (50th percentile) values from our study were very close to those and slightly higher/lower in the S&R, LJ and SR tests.
Unfortunately, the BAH test was only performed in the HELENA study, but the results are not comparable due to differences in the methodology applied.
Physical fitness standards have already been reported in a number of countries worldwide 1,2,9,10,11,30. In addition, much effort toward proposing harmonized measurements and standards of physical fitness of schoolchildren at a European level has been made 26,29. These results are of great importance particularly in countries which have not developed their own standards. However, it is well known that physical fitness level could be influenced by a number of factors, with biological and environmental factors playing a particularly important role. Therefore, for more appropriate interpretation of the physical fitness level of children from a particular country, nationally based standards obtained from random and large representative samples are required. Considering all this, and given the fact that children from Serbia were not included in the aforementioned studies, findings reported in the current study could be an important contribution to current standards.
The overall prevalence obtained in this study was 24.8%, of which 19.8% were overweight and 5% obese. With respect to gender, the prevalence of overweight and obesity was higher in boys (27%) than in girls (22.4%) in almost all age groups except in the youngest ones. In addition, the percentage of overweight and obese children decreased with age in both genders. These findings are in line with those from a study reporting prevalence of overweight and obesity in children from the national capital city 16 and significantly higher than those reported more than twenty years ago 18,20 and those reported recently 31. In addition, when compared with the prevalence obtained from other countries worldwide 11,20,32, the results presented in this study rank Serbian schoolchildren among those with the highest percentage of overweight and obese schoolchildren. Given that being overweight or obese is closely related to a higher risk of chronic diseases such as cardiovascular disease or skeletal health and mental health disorders 19,33, the findings of the current study point out that there is a significant public health problem that should be systematically treated in order to suppress this trend and prevent further increase in prevalence of overweight and obesity. Therefore, the study represents one of the first steps toward creating effective programs and policies in the national combat against this growing public health crisis.
Although it might be argued that the obtained cross-sectional data could be a limitation of this study as well as the test selection, which slightly differs from the ones applied in similar studies, the amount and the methods of the study sample selection, the standardized protocols and the qualified measurers guarantee validity and usability of the revealed data. Therefore, we believe that the findings presented here are a valuable contribution to the growing body of information regarding fitness levels of children worldwide, and to the attempts to introduce physical fitness testing as an important tool in monitoring physical fitness at the early stage, when prevention measures could be more effective in suppressing health risk problems.
To conclude, the findings presented in this study not only enable insight in the overall physical fitness level of Serbian schoolchildren but also provide gender- and age-specific national health related fitness standards for nine to 14-year-old schoolchildren. In addition, we propose these standards to be used in the future as a benchmark for regular physical fitness testing in educational settings. Finally, data presented regarding prevalence and obesity indicate that Serbia is among the countries with the highest prevalence in overweight and obesity, signalizing that serious measures should be taken in order to stop this alarming trend.

