










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Epigallocatechin-3-gallate (EGCG) is the most abundant catechin contained in green tea (Camellia sinensis) and represents 30-40% of the tea leaves dry weight 1. During recent years, an increasing number of in vitro and in vivo studies have confirmed the beneficial effect of EGCG against several chronic diseases in humans, such as obesity, cancer and diabetes 2.
Different hypothesis try to explain the anti-obesity mechanism of EGCG. For example, catechins have been associated with brown fat positive thermogenesis stimulus 3 and positive insulin secretion 4. Furthermore, biochemical studies showed the role of EGCG on hepatic lipid metabolism 5 and appetite modulation 6 and suppression 2. On the other hand, recent evidence has shown inhibitory effects of catechin on tumors growth 7. In cell culture studies, many mechanisms have been assumed to activity of such as anti-oxidant activity, inhibition of NF-B transcript factor and regulation of cell cycle 8.
Despite all the evidences on the role of green tea in combating obesity and cancer, exact molecular mechanisms remain elusive. In this context, this study was designed to improve the understanding of the EGCG anti-obesity and anti-cancer action. For this purpose, we selected hypoxia inducible factor 1 alpha subunit 1A (HIF1-α), phosphoinositide-3-kinase regulatory subunit 1 (PI3KR1) and rapamycin-insensitive companion of mTOR (RICTOR) genes as potential targets and examined the EGCG effects on gene expression in blood, considering that tissue reflects the systemic response to metabolic alterations.
MATERIAL AND METHODS
SUBJECTS
This study enrolled a subsample of severe obese (body mass index [BMI] > 40 kg/m2) female subjects aged 18-60 years that were submitted to green tea extract supplementation in a previous interventional study of our research group 9. Exclusion criteria included history of a metabolic disease, such as diabetes mellitus, hyper or hypo-thyroidism, and Cushing syndrome; current smokers; prescribed medications, such as antidepressants, anti-obesity, or hormonal therapy; patients who underwent bariatric surgery and individuals with alterations in liver biomarkers. All of the subjects gave their written informed consent. The study was approved by Research Ethics Committee of the Clinical Hospital of Ribeirão Preto Medical School, University of São Paulo, SP, Brazil (CAAE: 30247414.6.0000.5440).
GREEN TEA SUPPLEMENTATION
Thirty decaffeinated green tea capsules (single lot), formerly polyphenols capsules (Solaray(r) tablets, United States), were purchased from the United States and the quantitative analysis of green tea extract was performed 9. Each capsule contained 1,009.6 mg of green tea extract and 450.7 mg of EGCG. Other components included in the capsule were celluloses, magnesium stearate and silica. According to the established protocol 9, all individuals were oriented to ingest two capsules/time/day in morning fasting during eight weeks. Other modifications regarding diet or therapeutics were not allowed until the end of the study. If some medical procedures were needed, the subjects were excluded from the study.
To ensure the green tea effect and control possible bias, patients were instructed not to change dietary and physical activity pattern habits. Patients were weekly contacted by telephone as a form of control of the capsules ingestion and maintenance of dietary intake.
PHENOTYPIC CHARACTERISTICS
Anthropometric and body composition measurements (body weight [kg], height [m], BMI [kg/m2] and fat mass [FM, kg]) were collected before (one day before starting supplementation protocol) and eight weeks after the intervention. Weight was measured with an electronic platform Filizola(tm) scale with precision of 0.1 kg and maximum capacity of 300 kg; height was measured with a vertical shaft with 0.5-cm graduation. BMI was calculated with the formula BMI = weight/height2. Body composition was evaluated with a monofrequency Quantum BIA 101 q-RJL Systems analyzer (Clinton Township, MI, USA).
GENE EXPRESSION ANALYSIS
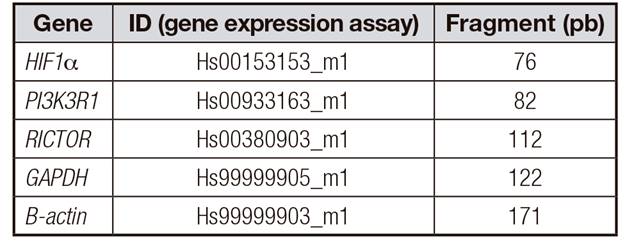
Blood samples were collected after 12-h fasting. RNA extraction from peripheral blood mononuclear cells (PBMCs) was performed using a phenol-chloroform extraction method modified 10. The RNA was transcribed to cDNA using high-Capacity cDNA Reverse Transcription1 kit (Life Technologies) according to the manufacturer's instructions. Gene expression for each selected gene (Table 1) was conducted by real-time PCR using 7500 Fast Real PCR System (Applied Biosystems(tm)). Relative quantification of gene expression, toward the pooled sample, was calculated by using the comparative delta-delta-Ct method 11. The expression level of each target gene is shown as the amount relative to GAPDH and β-actin (reference genes). These analyses were performed in triplicates for each sample.
STATISTICAL ANALYSIS
Results were expressed as mean ± SD. Data normality was verified by the Shapiro-Wilk test. The paired t test or Mann-Whitney test was used to determine the statistical significance of the differences between periods (pre- and post-supplementation). A p value equal or less than 0.05 was considered to be statistically significant. The Statistical Package for the Social Sciences (SPSS) for Windows (version 15.0; SPSS Incorporated, Chicago, IL, 2006) was used for data analysis.
RESULTS
A total of eleven individuals were enrolled in the study. One subject was withdrawn because RNA extraction was not possible, and our final sample was composed with ten women (mean age 35.1 ± 7.3 years). Comparing anthropometric and body composition measurements pre and post-supplementation periods, no significant differences were noted in weight (114.9 ± 14.3 versus 115 ± 13.8 kg), BMI (44.1 ± 3.7 versus 44.1 ± 3.9 kg/m2) or fat mass (47.6 ± 3.3 versus 47.3 ± 3.4 kg) (Fig. 1). The gene expression analysis showed that EGCG upregulated RICTOR and HIF1-α; however, PI3K expression did not change after green tea supplementation (Fig. 2 and Fig. 3).

Figure 1.No significant changes on anthropometric and body composition data were observed after green tea supplementation.

Figure 2 Boxplot for gene expression before and after green tea supplementation in obese subjects. A. HIF1-α. B. RICTOR. C. PI3K. *p < 0.05. Boxplot represents mean, first/third quartile and lower/higher value.

DISCUSSION
Our results showed an upregulation of RICTOR/mTORC2 and HIF1-α after eight weeks of green tea supplementation. This study presents novelties on this theme, and it is important to note that until the present moment, there are no studies in the literature evaluating the effect of EGCG on RICTOR/mTORC2 and HIF1-α expression in severe obese subjects. Besides, many studies conducted in rats models and cell culture have suggested that green tea polyphenols mimic insulin action 12 and, in addition, the literature presents conflicting results with regard to the EGCG molecular effect on obesity and cancer development 13.
In numerous studies demonstrated a negative association with obesity and cancer and green tea has been pointed out as a potential chemo-preventive food 14. In vitro, in vivo and epidemiological studies have demonstrated cancer may promote a downregulation of proteins involved in growth and proliferation of cancer cells 14.
Considering these aspects, previous revision showed that compounds derived from natural products can function as HIF1-α activators 15. HIF1 is a heterodimeric transcription factor, composed of two subunits: alpha subunit that is an oxygen-labile protein, which becomes stabilized under hypoxic conditions, and beta subunit, which is constantly expressed 16. Upon activation, HIF1-α controls the transcription of many target genes and its protein products play crucial roles in acute and chronic adaptation to oxygen deficiency, including glycolysis, angiogenesis and energy metabolism, promoting adaptation and survival under hypoxic conditions 17.
In normoxic conditions, oxygen (O2-) and iron (Fe2+) radicals promote the degradation of HIF1-α subunit. However, conditions of hypoxia, as in obesity for example in which oxygen becomes scarce, promote an inhibition of hydroxylation and the consequent stabilization of the HIF1-α protein and its rapid accumulation 16. In line with this, EGCG were shown to induce HIF1-α activity through activation of enzyme systems and signaling pathways, such as mitogen-activated protein kinase (MAPK), with the consequent increase of mRNA expression levels targets genes 18,19. Contradictorily, evidences suggested an important role of HIF-1α in triggering the inflammatory response. Higher levels of free fatty acids and reduced oxygen perfusion due to excess of body weight stimulate HIF-1α expression and consequently, the synthesis of inflammatory cytokines 20.
Although the control of genes involved in cancer by EGCG remains contradictory, we first identified an increase in HIF1-α expression in PMBCs after eight weeks green tea supplementation in severe obese women. However, some authors postulate that an effect of green tea on cellular survival programs by means HIF-1α expression may represent a negative effect on chemoprevention, in addition to explaining many contradictory results found in the literature. In this way, the literature indicates various roles of HIF-1α in many tissues 21. For this reason, specific-tissue manipulation is difficult to translate into the organism as a whole. There are few studies evaluating an expression of HIF-1α in peripheral blood, bringing this fact as a limitation of the present study.
Moreover, another plausible mechanism responsible for the increased risk of cancer in obese patients is through PI3K action. The PI3K signaling pathway is a regulator of physiological and cellular processes including cell proliferation, growth, migration and metabolism. It is already well described that hyperactivation of PI3K/Akt signaling is related to several types of cancer in humans 22. However, despite in vitro studies identified downregulation of PI3K pathway after EGCG treatment 23,24, the gene expression did not change after green tea supplementation in our obese individuals sample. Knowing that PI3K is regulated by several factors such as insulin, growth factors, leptin, and others, the no alteration identified in the expression of this gene after treatment with EGCG for eight weeks cannot be explained in this study.
On the other hand, our results also showed an upregulation of RICTOR expression. RICTOR is an essential subunit of mTORC2 complex that facilitates both the assembly of mTORC2 and the interaction of mTORC2 with its substrates and regulators 1,25. However, the mechanism by which mTORC2 is activated, as well as its exact function, are not entirely clear 26, though alterations in mechanism of mTOR pathway are found to be implicated in the oncogenesis of different tumor types. In line with this, overexpression of RICTOR in several cancers has been found and associated with poor survival and potential cancer therapy target 27. Thus, considering obesity and cancer treatment, it should be noted that our results demonstrate an increase in RICTOR expression and that the functions of mTORC2 in the various tissues are not yet fully elucidated 28. No conclusion can be drawn regarding the role of EGCG in increasing its expression in severe obese women. Indeed, we have to highlight that there are some reports in the literature showing that benefits of EGCG occur in dose- and time-dependent manner 29.
Nevertheless, we can hypothesize the mechanisms by which EGCG could change RICTOR expression. Despite it is described in the literature that mTORC2 activation is via the PI3K/Akt pathway 30, data of the present study indicate that RICTOR can also be stimulated by other factors. One possible mechanism is the activation of another pathway, different of insulin/growth factors signaling pathway, like the increase of cAMP levels by catecholamines and activation of β2-adrenoceptors, for example. The cAMP activates cAMP-dependent protein kinase (PKA), which phosphorylates mTORC2 at Ser2481 and activates this protein. mTORC2 activated causes translocation and insertion of GLUT4 to the plasma membrane of skeletal muscle cells and stimulates glucose uptake without the involvement of PI3K, Akt or AS160 31. It has been suggested that the EGCG can inhibit an enzyme that degrades norepinephrine (catechol-O-methyltransferase), thereby prolonging the action of norepinephrine released by sympathetic neurons 32. In addition, it has been observed that EGCG supplementation increases plasma concentrations of norepinephrine and epinephrine in humans 33 and, together, the increase observed in mTORC2 expression in the EGCG group may be associated to increased sympathetic activity and activation of β2-adrenoceptors, stimulated by the EGCG.
Moreover, authors reported that RICTOR has the function of controlling carbohydrate response element-binding protein (ChREBPβ) expression by adjusting glucose uptake, and without impairing AKT signaling. In this context, the upregulation of RICTOR/mTORC2 pathway by polyphenols present in green tea may lead to activation of target genes involved in glucose and lipid metabolism and may improve insulin resistance in obese subjects 34. RICTOR overexpression has already been show in obese women after gastric bypass. The authors understood that, because mTORC2 is related to lipogenic genes expression and de novo lipogenesis (DNL) control 2,34, its overexpression after surgery may lead to improvement of insulin resistance and lipolysis, both evidenced 35.
In view of the number of studies that seek to understand the molecular pathways related to obesity and its comorbidities, such as the use of green tea catechins as a treatment of chronic diseases, despite our limitation in relation to the small sample number of the study, we speculated that green tea may not directly address weight loss but could be used as a coadjutant treatment of obesity-associated comorbidities. However, this study was a pioneer in identifying HIF-1α and mTORC2 modifications after green tea supplementation in obese humans, and more studies with a larger population group should be conducted to evaluate other EGCG concentrations as time of supplementation and tissue-specific action.
CONCLUSION
In conclusion, the supplementation of 450 mg of EGCG with green tea capsules during eight weeks in obese women modulated the PMBCs expression of HIF1-α and RICTOR-mTORC2. Despite the limitations of the study, these findings suggest that green tea catechins have a potential role in the control of obesity and cancer, and studies with a larger population group and other doses of EGCG and times of ingestion should be performed to confirm these effects.

