










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
The prevention of cardiometabolic diseases is a priority due to their relationship with serious COVID-19 complications. Among diverse risk factors for cardiometabolic diseases, behavior is the most closely associated and unhealthy lifestyles, characterized by inadequate diet and physical inactivity, are the cornerstone (1). High rates of childhood obesity are of particular concern worldwide, and Mexico is not the exception since from population aged 12 to 19 years, 38.5 % have either overweight or obesity (2). Obesity is a risk factor for hypertension, insulin resistance, and type 2 diabetes, among other conditions that are increasingly present in childhood and can persist into adulthood (1).
In children and adolescents, the most commonly measurements to diagnose obesity are body mass index (BMI) and BMI percentile, weight-for-height ratio calculated by z-scores, and body fat (3). Recently, body fat has gained a particular importance in clinical settings. Fat mass quantification in youth is a priority due to its different effects on insulin sensitivity and energy availability, which predicts cardiometabolic risk more accurately (4). However, its use is limited by the lack of reference data for specific child populations (5).
The debate about which food groups are beneficial or detrimental to cardiometabolic health has recently been renewed (6). In adults, several studies indicate that certain dietary and physical activity (PA) components play an important role in body fat regulation (7). However, in adolescents this association is not entirely clear (6). Studies have identified sugar-sweetened beverages (SSB) as a group strongly associated with adiposity and cardiometabolic risk in adolescents (8,9). Some authors have mentioned the “fast-food group”, characterized by a high content of saturated fatty acids (SFA), as the most important food group related to changes in body composition (8). Despite these findings, other studies found no association between intake of SSB and fast food with body composition (10). Trumbo and Rivers (10) carried out a systematic review analyzing the association between SSB and obesity, and concluded that the relationship was inconsistent. Moreover, an association of the group of whole foods has been found (7), so as fruits and vegetables (F&V) (11-13), with body composition.
Mexico has a very extensive gastronomy, which means that the country has very diverse dietary patterns. Ponce et al. (14) reported differentiated intakes of total fats and SFA by regions. Furthermore, these authors evaluated the quality of diet and found different amounts of consumption of F&V by different age groups. In addition, the Mexican diet has been modified in recent years by the introduction of foreign food patterns due to globalization (15). Due to these disparities, it may be inappropriate to generate general scientific conclusions in different age groups about the traditional Mexican diet and its relationship with body composition. Therefore, it is necessary to evaluate the actual diet in Mexican adolescents and its association with body fat as the main determinant for obesity, to make recommendations accordingly.
Due to the inconsistency of studies, it is not clear which food group is most strongly associated, either positively or negatively, with body composition in adolescents. Few studies have investigated the role of specific eating and PA behaviors, and their association with body fat (7,16,17). Furthermore, as far as we know, the research is almost null in Mexican adolescents. Therefore, this study aimed to examine whether there is an association between lifestyle factors such as diet and PA components with body fat in Mexican adolescents.
METHODS
STUDY DESIGN
The study design was cross-sectional, carried out from August to December 2018 at the Technological Institute of Sonora (ITSON), Cd. Obregon, Sonora, Mexico. Data collection was carried out at the Laboratory of Preventive Nutrition and Healthy Eating. The study protocol and materials were approved by the ITSON Research Ethics Committee. Data from participants were confidential.
RECRUITMENT AND STUDY POPULATION
The inclusion criteria were freshman under 20 years of age. Exclusion criteria included having a pre-diagnosed cardiometabolic disease, taking medication, being pregnant or breastfeeding, or having a mental illness that affected their ability to participate. At the beginning of the semester, face-to-face talks were held by trained staff, in which the objective, protocol, and procedures of the study were explained. Those interested were given a written summary of the study and asked to inform their parents. Written informed consent from the parents and written assent of adolescents who agreed to participate were obtained.
Participants were scheduled through phone calls or text messages. As an incentive, participants were offered academic credits for participation as part of an agreement with the university staff in the Healthy Lifestyle University Program to which each student must enroll. The study protocol included demographics and health history, anthropometric and blood pressure measurements, food consumption and PA registries.
DEMOGRAPHIC DATA COLLECTION
Demographic data, personal and family health history, smoking habit, and socioeconomic level were collected through questionnaires applied in person.
ANTHROPOMETRIC AND BLOOD PRESSURE MEASUREMENTS
Participants attended after an overnight fast (> 10 hours) in light clothing. Weight and body fat were measured without shoes or metal accessories with a TANITA model BC-533 scale with electrical bioimpedance. Reference values for body fat were for men ≤ 20 % and for women ≤ 25 % (18). Height was measured without shoes or hair or head accessories, with a SECA stadiometer. BMI (weight in kg divided by height in m2) was used to calculate BMI percentiles according to CDC growth charts for age and sex. Waist circumference was measured at the umbilicus position using a Lufkin tape measure. For height and waist circumference, the average of three measurements was used.
Blood pressure was measured in the right arm with an Omron baumanometer (Omron Healthcare, Inc., Bannockburn, IL) with the participant in a sitting position after resting quietly for five minutes. Measurements were taken at one-minute intervals and a three-measurement average was used.
ASSESSMENT OF DIETARY INTAKE
Dietary data were obtained through the 24-hour recall (24 h R) with two repetitions, applied in person. To calculate nutrients, the dietary data were captured on a web page using the Mexican System of Equivalent Foods (19), and those not found were verified in the United States Department of Agriculture (USDA) food database (20).
The 24 h R were captured in a Microsoft Excel spreadsheet (Microsoft Co., Redmond, WA, USA). Equations with serving sizes were used to calculate daily or weekly intake of individual foods, and then summed for each food group. The ideal intakes for food and nutrient groups were defined according to the American Heart Association Healthy Diet Pattern (21), which is characterized by five primary metrics: F&V ≥ 4.5 cups/d, fish and shellfish ≥ 200 g/wk, sodium < 1,500 mg/d, SSB ≤ 36 oz/wk, and whole grains ≥ 3 oz/wk; and three secondary metrics: nuts/seeds/legumes ≥ 4 serving /wk, processed meat ≤ 100 g/wk, and SFA < 7 % total kcal/d (22). Outliers defined by ± 3 standard deviation (SD) were removed.
EVALUATION OF PHYSICAL ACTIVITY
PA was assessed using the IPAQ, previously validated in Spanish (23). This questionnaire has questions referring to the intensity (type), duration (minutes/wk) and frequency of activity (days/wk) that participants performed during the last week. Activities were described as vigorous, moderate, light, and sedentary. Answers were used to calculate minutes per week that participants dedicated to each activity. Regarding the ideal PA, recommendation is ≥ 420 min/wk of moderate or vigorous (22).
STATISTICAL ANALYSIS
The normal distribution of data was verified according to the asymmetry, kurtosis, and the Kolmogorov-Smirnov tests. Means and SD were calculated for continuous variables, and percentages for categorical measures. The Chi-squared test was used to compare the difference in prevalence of demographic variables. The t-test for independent samples was used to evaluate the differences by sex in anthropometric, dietary, and PA variables.
Potential association was evaluated by univariate linear regression (p < 0.02 and biological plausibility) to identify the variables associated with body fat. The possible associated variables such as socioeconomic status, family history, smoking, blood pressure, dietary components, and physical activities were included in the univariate analysis. Multiple models were built by a combination of the univariate analyses and forward stepwise model selection using p ≤ 0.05 and biological plausibility. Preliminary models were evaluated for possible interactions (p ≤ 0.1) between sex/gender with the other variables included in the model, where no interaction was obtained (results not shown). Preliminary models were also tested for collinearity (variance inflation factor [VIF] < 10) and linear regression assumptions (linearity, normality, and homoscedasticity) using residual plots. Results were considered as significant with a value of p ≤ 0.05. The statistical software package Stata version 14.1 was used.
RESULTS
DEMOGRAPHIC AND ANTHROPOMETRIC CHARACTERISTICS
A total of 342 first-year college students were invited to participate. From these, 250 students were recruited, and finally a total of n = 230 completed the protocol (126 men and 104 women), with a mean age of 18.5 ± 0.4 y. Table I shows demographic data by sex; no significant difference was found in age, socioeconomic level, most inherited-family diseases and smoking (p > 0.05). Men presented higher prevalence in work status (p = 0.002), family history of hypertriglyceridemia (p = 0.01) and sports practice (p = 0.001). Table II shows anthropometric characteristics, in which men presented higher height, waist circumference, systolic and diastolic blood pressure (p < 0.001). Conversely, body fat was higher in women as it was expected according to the biological differences by sex (p < 0.001). There were no significant differences for the rest of the variables (p > 0.05). Regarding body fat, the data obtained in the study showed that men had 18.1 ± 6.6 % body fat, with 38.1 % participants with values greater than 20 % body fat; while women had 25.6 ± 6.6 % body fat; with 46.2 % participants with values greater than 25 % body fat.
Table I. Demographic variables in Mexican adolescents.

*Chi-squared test.
†T-test for independent samples.
‡Significant at p < 0.05.

DIETARY INTAKE AND PHYSICAL ACTIVITY
Dietary intake and PA by sex are summarized in table III. Men had significant higher total energy intake (p < 0.001), sodium (p = 0.008), SSB (p = 0.001), whole grains (p = 0.002), nuts/seeds/legumes (p = 0.012), processed meat (p = 0.005), and SFA (p = 0.006), while women had a significant higher intake of fish and shellfish (p = 0.027). In addition, men showed more time dedicated to moderate (p = 0.030) and vigorous PA (p < 0.001). Table III shows the percentage of participants who met the recommendation for each food and nutrient group, and for PA.

ASSOCIATIONS OF DIET AND PHYSICAL ACTIVITY WITH BODY FAT
Univariate linear regression analyses revealed that being male was associated with lower body fat (standardized beta coefficient [β] = -7.48, p ≤ 0.001). Dietary total fat intake (β = 0.20, p = 0.006) and SFA intake (β = 0.38, p = 0.016), separately, were significantly associated with higher body fat, while intakes of whole grains (β = -3.33, p = 0.034) and nuts/seeds/legumes (β = -2.22, p = 0.049), and vigorous PA (β = -0.01, p < 0.001) were significantly associated with lower body fat (Table IV).
Table IV. Variables associated with body fat in Mexican adolescents through univariate analysis.
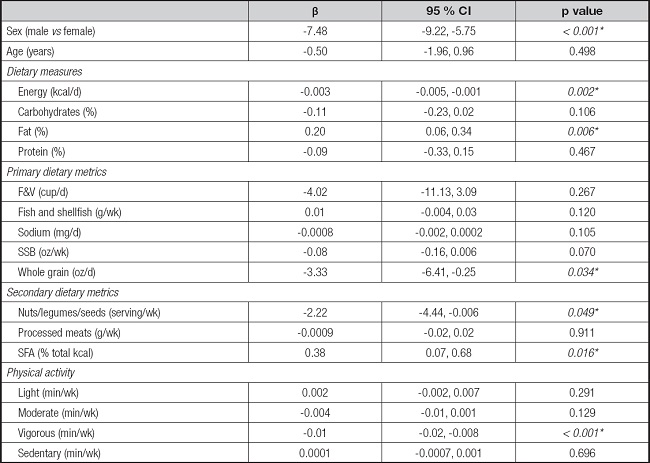
F&V: fruits and vegetables; SSBs: sugar-sweetened beverages; SFA: saturated fatty acids.
*Significant at p < 0.05.
When evaluating by sex, the consumption of F&V (β = -13.09, p = 0.011) was also significantly associated with lower body fat for men, while no other variable was added as significant for women (Table IV).
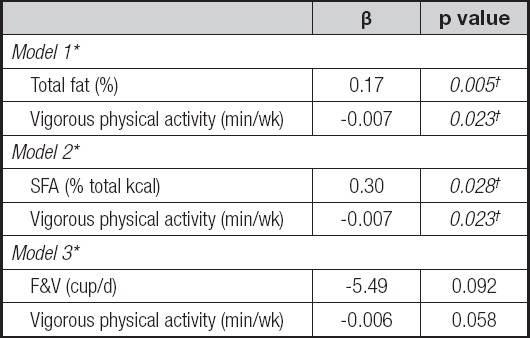
Table V shows the multiple models. All models met all the assumptions of multiple linear regression. In model 1, variables associated with body fat were total dietary fat (β = 0.17, p = 0.005) and vigorous PA (β = -0.007, p = 0.023), while in model 2 were SFA (β = 0.30, p = 0.028), as well as vigorous PA (β = -0.007, p = 0.023). Model 3 included vigorous PA (β = -0.006, p = 0.058) and F&V intake (β = -5.49, p = 0.092), although both variables with a trend towards significance. All models agreed that performing vigorous PA was a protective factor against body fat. As a secondary analysis, logistic regression showed similar results (data not shown).
DISCUSSION
Adolescence is a stage in which the individual is still growing, and body changes become stable at the end of this stage (24). According to this, participants in our sample still tend to have a low content of fat percent, which could also be maintained due to the physical activities they still practice. Different studies have evaluated the association of lifestyle factors with body fat. However, there are variations in the analyzed components that do not allow generalizations to be made. For instance, there are multiple methods/markers to measure body fat that make comparisons to be difficult, as well as some that reduce the accuracy of results (25). BMI as an estimator of body fat is one of the most widely used methods, due to the fact that it is easy to calculate, no specialized equipment is required to measure its components and, therefore, they can be easily measured in field (9). Despite these advantages, the use of BMI to assess body fat is questionable since some studies indicate the absence of a correlation between BMI and body fat (9) since BMI is an indicator based on body weight, and does not distinguish lean mass from fat mass. Therefore, using BMI to assess body composition or body fat distribution may lead to misclassification (26). In our study, BMI, waist circumference, and body fat were independently analyzed using linear regression; however, only body fat was significant associated with the lifestyle variables (diet and PA) (data not shown for BMI and waist circumference).
Other methods and metrics used to measure adiposity are DEXA, bioelectrical impedance (9), adiposity index (16) and equations derived from skinfolds thickness (12). In the present study, bioelectrical impedance was used to assess body composition, which is a safe, portable, inexpensive, simple, rapid and non-invasive equipment to distinguish between fat mass and fat-free mass (5). Although this technique provides slightly less accurate data than other methods, bioelectrical impedance has a great practical advantage in measuring body fat in clinical and population-based settings (5).
Regarding dietary intake, in multiple model 1 from the present study, a higher consumption of fat was associated with a higher body fat. Similarly, Mistretta et al. (13) found that higher fat intake was associated with overweight/obesity in men (OR 1.55; 95 % CI: 1.10-2.18) and women (OR 1.41; 95 % CI: 1.05-1.89). Likewise, Labayen et al. (27) explored dietary fat intake in adolescents and reported no association with body fat in those with fat intake lower than 30 % of energy (%E). In contrast, in adolescents with fat intake between 30 and 35 %E, there was a positive association with body fat (95 % CI: 0.39, 3.33; p < 0.05); and in those with fat intake greater than 35 %, this variable was associated with 32 % more body fat compared to the group with 30-35 %E from fat intake (95 % CI: 1.27, 4.43; p < 0.001) (27).
Results from multiple model 2 indicated that a higher consumption of SFA was associated with a higher body fat. Among the studies that have evaluated diet and body fat, Ambrosini et al. (16), in children and adolescents, found that a greater adherence to a pattern of elevated consumption of high-SFA foods such as confectionery, cakes and cookies, was significantly associated with a higher body fat (95 % CI: 0.01-0.07, p = 0.017) (19). In addition, Fernandez et al. (17) studied the prospective associations between diet and changes in body composition in European children. Children who obtained higher scores for the so-called “processed” pattern, which consisted of a greater consumption of fast food with a high content of SFA, and less consumption of foods high in fiber, presented greater body fat gain over time (β = 0.052; 95 % CI: 0.014, p = 0.090), compared to children who obtained higher scores for the “healthy” pattern, which consisted of elevated consumption of low-fat foods, vitamin-rich foods and whole foods, and less consumption of products with high content of SFA and sugar (17). Results obtained from the present study and those reported in the literature suggest that the SFA nutrient is associated with a high body fat.
Studies in different age-populations such as middle-aged individuals found that SFA were positively associated with body fat, impacting in a variety of metabolic diseases such as type 2 diabetes, inflammatory diseases, and cancer (28). SFA have biological activities that act either positively or negatively on the metabolism, depending of the level of intake. They influence the biosynthesis of cholesterol, fatty acids and triacylglycerol (29); lipoprotein assembly, secretion and clearance (30); and inflammatory processes (31). These processes occur through effects on the regulation of transcription factors involved in lipid metabolism (SREBP, LXR/RXR, HNF4) and inflammation (NF-κB). Therefore, adequate intakes of SFA play a very important role in metabolism, but excessive intake is a risk factor for cardiometabolic disease, since the induced negative health effects such as increases in insulin resistance, blood lipids, inflammation, etc. (8).
In multivariate model 3, a higher consumption of F&V was strong but not significantly associated with low body fat. Among the few published studies is the one carried out by Anyżewska et al. (7), in which results were similar to ours when observing that the fruit consumption is a protective factor against the increase in body fat in soldiers of the Polish air cavalry units. Unlike our study, they evaluated the consumption of F&V separately, obtaining a negative association between fruit consumption and body fat (β = -0.23, p = 0.022) with no significant associations with vegetable consumption (7).
Regarding vegetable intake, Howe et al. (6) analyzed a dietary pattern called “F&V” which consisted of a high consumption of fruits, vegetables, cheese and whole wheat bread. Results indicated that adolescents who scored higher for the “F&V” pattern had lower body fat (β = -2.55; 95 % CI: -5.12, 0.09) (6). Besides, Mistretta et al. (13) studied the association of different food groups with overweight/obesity in adolescents from southern Italy, finding that intake of vegetables was inversely associated with overweight/obesity (OR 0.91; CI 95 %: 0.86-0.96 for men and OR 0.86, 95 % CI: 0.79-0.94 for women) (13). Moreover, Cook et al. (11) found that vegetable consumers had 17 % less visceral adipose tissue compared to non-consumers (p = 0.01) in overweight Latino youth (11). Results from the present study and those reported in the literature suggest that F&V is a protective group against the increase in body fat. In addition, F&V are considered to be healthy foods that contribute to the protection of chronic non-communicable diseases, including obesity (12). Although the consumption of F&V by our participants was very low, its association in model 3 was the strongest compared to dietary variables from model 1 and 2, but non-significant. Due to the observed low intakes, it is crucial to promote the consumption of F&V among Mexican adolescents.
The pathways through which F&V influence health are still poorly understood (11). However, this group is characterized by their abundance in dietary fiber (32). Dietary fiber has viscous and gel-forming properties that help to decrease postprandial glucose responses, inhibit macronutrient absorption, beneficially influence certain blood lipids, and slow gastric emptying (11). Likewise, studies have reported associations of a high consumption of dietary fiber with low levels of indicators for cardiometabolic diseases, such as reduced risk of diabetes (32).
In the present study, the three models indicated that performing vigorous PA was associated with low body fat. PA has been reported as a protective factor against increases in body fat (33-36). Jiménez et al. (33) evaluated the association of PA with body components in European adolescents, finding that vigorous, moderate-vigorous, and moderate PA were negatively associated with BMI, skinfold thickness, body fat, and waist circumference (all p < 0.01). Similarly, Joensuu et al. (34) evaluated different activities within the level of moderate PA and its association with body composition in adolescents, finding that performing any of the proposed activities was associated with a lower body fat. Mielke et al. (35) studied the associations between PA and screen time with cardiometabolic risk factors in adolescents, and found that higher levels of PA appear to be more important than lower levels of screen time for cardiometabolic health in adolescents (35). Furthermore, Saunders et al. (36) conducted a systematic review and demonstrated that moderate to vigorous PA intensity is associated with positive health outcomes, conversely than sedentary behavior, in youth and adolescents. Finally, we can highlight that diet and PA are the most important behavioral determinants for body composition changes, especially in weight maintenance and prevention of weight and body fat gains (8). Experimental studies indicate that when diet and PA are administered together, they promote stronger effects on body composition (37).
Among the strengths of the present study is the use of body fat as a marker for body composition, since this tissue predicts the risk for cardiometabolic diseases with greater precision (4). The use of electrical bioimpedance to measure adiposity is another strength because it is a safe, portable, inexpensive, simple, fast and non-invasive method (5). A third strength is the sample size, since it is a relative representative sample size that is similar to other studies (7,11), in addition to the fact that it is a population group whose dietary habits associated with adiposity had not been studied. Additionally, the food and nutrient groups analyzed are recognized in the literature as important preventive factors for cardiovascular health (23). A final strength was that all measurements were performed by trained personnel, which reduced reporting bias and measurement errors.
Despite these strengths, the present study also had certain limitations. A causal link between consumption of a food group or nutrients, PA, and body fat cannot be highlighted, given the nature of the cross-sectional design; however, results do not contradict what was found in cohort and experimental designs. Second, participants estimated their daily PA based on a structured questionnaire (19), and self-reported measures of PA show a higher variability compared to objective measures (38). However, the IPAQ is a widely used instrument validated through the use of accelerometers (33). Another limitation was the use of only two repetitions of the 24 h R, which do not allow to distinguish variability between and within people, making it difficult to estimate the usual intake. Despite this, there are cross-sectional studies that found associations between diet and health outcomes using a single 24 h R (39). Last limitation is that all the participants were university students, with characteristics that cannot be extrapolated to other adolescents (i.e., those adolescents who do not study, who are married, etc.), since they may have a very different lifestyle. This group of participants experience the “freshman transition”, which is a critical transformational experience from high school exit to college entry that can create lifestyle changes (40). Weight gain in freshmen is common and reflects increased adiposity in approximately 75 % of freshmen (40).
In conclusion, this is the first study that reports current lifestyle patterns of Mexican adolescents, in which vigorous PA and dietary intake of total fat and SFA, and F&V although not significantly, are associated with body fat. These variables are critical lifestyle components needed to be included in programs promoting healthy lifestyles. Community-based prevention programs should be included in the public policies of Mexican adolescents, due to their impact on body composition, in which it is crucial to address increases in daily vigorous PA, promotion of protective food groups, and information about the risk of excessive consumption of certain foods associated with adiposity as an early cardiometabolic risk factor.

