










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkAnales de Psicología
versión On-line ISSN 1695-2294versión impresa ISSN 0212-9728
Anal. Psicol. vol.33 no.3 Murcia oct. 2017
https://dx.doi.org/10.6018/analesps.33.3.263751
The effects of anticipatory fatigue and emotional symptomatology on perceived physical and cognitive fatigue
Efectos de la fatiga anticipatoria y la sintomatología emocional en la percepción de fatiga física y cognitiva
Sandra Fuentes-Márquez1, Cristina Senín-Calderón2, Juan F. Rodríguez-Testal3 and Miguel A. Carrasco4
1 Hospital Juan Ramón Jiménez de Huelva (Spain).
2 Departamento de Psicología. Universidad de Cádiz (Spain).
3 Departamento de Personalidad, Evaluación y Tratamiento Psicológicos. Universidad de Sevilla (Spain).
4 Departamento de Personalidad, Evaluación y Tratamientos psicológicos. Universidad Nacional de Educación a Distancia (UNED) (Spain).
ABSTRACT
The two fold aim of this study was first, to analyze the effects of anticipatory fatigue, emotional symptomatology and belonging to a clinical group on the physical and cognitive perception of fatigue, and second, to explore the potential moderating effect of anticipatory fatigue on the relationship between symptomatology or clinical condition and perceived fatigue. The conditional and partial effects of independent variables were analyzed by hierarchical regression in an ex-post-facto correlational design. The sample was composed of 317 participants (29% from a clinical population). Anticipatory fatigue (by an ad hoc scale), and perception of fatigue (by the Chalder Fatigue Scale) were measured. Emotional symptoms were assessed by Goldberg's GHQ-28 questionnaire. Anticipatory fatigue and emotional symptoms (mainly depressive) had significant effects on cognitive and physical fatigue. Belonging to the clinical group significantly and exclusively predicted cognitive fatigue. Furthermore, anticipatory fatigue moderated between-group effects (clinical versus general) and cognitive fatigue. In brief, emotional symptoms (mainly depressive) and anticipatory fatigue significantly predicted perceived cognitive and physical fatigue. Anticipation of fatigue moderated the effect of clinical group on cognitive fatigue after controlling for depressive symptomatology.
Key words: Anticipatory fatigue; depressive symptoms; somatic and anxiety symptoms; cognitive and physical fatigue.
RESUMEN
El objetivo de este estudio fue doble, primero, analizar los efectos de la fatiga anticipatoria, la sintomatología emocional y la pertenencia a un grupo clínico sobre la percepción de fatiga física y mental; segundo, explorar el potencial efecto moderador de la anticipación de la fatiga en las relaciones entre la sintomatología o la condición clínica y la sensación percibida de fatiga. Se analiza mediante un diseño ex post facto y correlacional los efectos parciales y condicionados de las variables predictivas mediante diferentes análisis de regresión jerárquica. Participaron 317 sujetos (29% procedentes de población clínica). Se evaluó la fatiga anticipatoria (Escala elaborada ad hoc), la experiencia percibida de fatiga (Escala de Fatiga de Chalder et al., 1993), y la sintomatología emocional (GHQ-28 de Goldberg, 1996). Los resultados mostraron efectos significativos de la fatiga anticipatoria y la sintomatología emocional, predominantemente de la sintomatología depresiva sobre la percepción de fatiga física y mental. La pertenencia a un grupo clínico predecía de forma significativa y exclusiva la fatiga cognitiva. Además, la fatiga anticipatoria moderaba el efecto del grupo (clínico versus general) sobre la fatiga cognitiva. En conclusión, la sintomatología, principalmente la depresiva, y la fatiga anticipatoria, tienen un valor predictivo significativo en la experiencia percibida de la fatiga física y mental. La anticipación de fatiga moderaba el efecto del grupo clínico sobre la experiencia de fatiga cognitiva una vez controlada la sintomatología depresiva.
Palabras clave: Fatiga anticipatoria; síntomas depresivos; somáticos y ansiosos; fatiga física y cognitiva.
Introduction
Fatigue is a frequent complaint in primary care (10-22%) (Lindeberg, Rosvall, & Östergren, 2012). A distinction is made between the perception of fatigue (hereinafter fatigue), an aspect of central fatigue (divisible in turn into physical and cognitive fatigue), and fatigability (objective changes in execution) (Chaudhuri & Behan, 2004). Psychological factors, such as perception of effort, (Sáez-Francàs, Hernández-Vara, Corominas-Roso, Alegre-Martín, & Casas-Brugué, 2013), mood or motivation (Kluger, Krupp, & Enoka, 2013) are involved in cognitive fatigue.
The association between fatigue and depressive or anxious symptomatology is well-known (Brown & Kroenke, 2009; Demyttenaere, De Fruyt, & Stahl, 2005; Doyle, Conroy, McGee, & Delaney, 2010). The perception of fatigue may come from feedback from these emotional states, favoring anticipation of more fatigue. Anticipation of fatigue is similar to the process of apprehensive expectation in anxiety as described by Barlow (2002), or expectation of failure in depression (Koval, Kuppens, Allen, & Sheeber, 2012; Lo, Ho, & Hollon, 2008; Rochat, Billieux, & Van der Linden, 2012). Other symptoms appear in depression and anxiety (desperation, rumination, automatic thinking, etc.), strengthening functional deterioration (Helbig-Lang, Lang, Petermann, & Hoyer, 2012; Nitschke et al., 2009; Ruscio, Seitchik, Gentes, Jones, & Hallion, 2011). As Rief, Glombiewski, Gollwitzer, Schubo, Schwarting and Thorwart (2015) suggest, cognitive expectation usually has a main role in psychopathology, however, unlike expectation in anxiety and depressive disorders, the roll of expectation or anticipation of fatigue has not been studied in depth.
Finding the presence of anticipated fatigue may be relevant because of its possible effect on the perception of fatigue itself and/or on behavior, e.g., avoidance behaviors. Certain anxiety, depressive or somatic manifestations may maintain or aggravate the general state of functioning (Goldstein et al., 2013). This includes the perception of fatigue, either the emotional states which intervene in the relationship of anticipation and perception of fatigue, or how these emotional states are moderated by anticipation of fatigue. Thus, recent studies have found a relationship between anticipation and the perception of fatigue (physical and cognitive) but mediated by emotional symptomatology (Fuentes-Márquez, Senín-Calderón, Rodríguez-Testal, Carrasco-Ortiz, 2015; Rodríguez-Testal, Fuentes-Márquez, Senín-Calderón, Carrasco-Ortiz, 2016). The first objective of this study is to analyze the predictive value of apprehensive expectation of fatigue (anticipation of fatigue), emotional symptomatology (i.e. depressive, anxiety and somatic) and belonging or not to a clinical group (clinical condition) on the physical and cognitive fatigue experience itself. In view of the significant relationships reported in the literature between symptomatology and cognitive expectation of fatigue and its perception, it is hypothesized that anticipatory fatigue, the presence of emotional symptomatology or belonging to a clinical group contribute significantly to greater perception of both physical and cognitive fatigue. Pertaining to a clinical group is an indicator of severity in the presence of symptomatology interfering in a person's daily functioning and could therefore be a predictor of the perceived fatigue experience. The second objective is to analyze the possible moderating effect that anticipatory fatigue has on the relationships between emotional symptomatology or belonging to a clinical group and the perception of physical or cognitive fatigue. That is, it is intended to explore how apprehensive expectation of fatigue can amplify or lessen the effect that emotional symptomatology or its severity (belonging to a clinical group) has on perceived fatigue. Thus it is hypothesized that the effects of depressive, anxiety and somatic (in order of importance) symptomatology on the perception of fatigue, mainly on cognitive (congruence of symptomatology) and in a group of patients (severity of the symptomatology) are moderated by its level of anticipation. In other words, the moderating effect of anticipation of fatigue has a greater impact on cognitive fatigue because of the congruent cognitive component shared by these variables (cognitive fatigue and apprehensive expectation of fatigue) and when the person's symptomatology is more severe (in the clinical group). Knowledge of the predictive and moderating role of apprehensive expectation of fatigue and the presence of symptomatology on perceived fatigue would alert to the need to design interventions focused on this cognition to reduce the fatigue experience. Knowledge of its interaction with the symptomatology would enable us to approach understanding of the relationships among these variables and the function of anticipation of fatigue augmenting or lessening emotional symptomatology in a clinical or general population when suffering from physical or cognitive fatigue.
Method
Participants
The sample was made up of 317 participants, 92 (29%) from the clinical population and 225 (71%) from the general population. Those in the clinical group (CG) were from a Community Mental Health Unit and a private psychology clinic. This group had 31 men and 61 women aged 18 to 76 (mean age = 38.87 years, SD = 14.31). The nonclinical group (NCG) had 90 men and 135 women aged 17 to 70 (mean age = 32.45, SD = 12.94).
The gender distribution (χ2 (1) = 1.10, p = .31) and social class (t (315) = 1.17, p = .24), evaluated using the Hollingshead Index (Hollingshead, 1975), were similar in the two groups. However, there were differences in age (t (315) = -3.88, p < .001). Both groups were predominantly high-middle social class. The CG had a higher mean age (Mean = 38.87, SD = 14.31) than the general group (Mean = 32.45, SD = 12.94). Variance in the age variables (FLevene = 1.120, p = .291) and social class (FLevene = .938, p = .334) was homogeneous.
Diagnoses were made by specialized psychologists with accredited clinical experience in treating patients with severe mental disorders following the criteria of the Diagnostic and Statistical Manual of Mental Disorders DSM- IV-TR (APA, 2000). The diagnoses of patients in the CG were grouped in the following categories: mood disorders (27.2%), anxiety disorders (25%), adjustment disorders (17.4%), psychotic disorders (7.6%), personality disorders (6.5%) and somatoform disorders (11.9%). Therefore, the group variable is indicative of the presence of clinical symptomatology in different alterations, mainly anxiety and depression.
Design
An ex post facto cross-sectional design was used. The sample was recruited by a non-probabilistic procedure. Patients were found by convenience sampling, and the snowball procedure was used to recruit the general population group.
Instruments
- Clinical and Demographic Information Sheet (ad hoc). Selfreport designed to collect sociodemographic data, medical history, and personal and family background.
- Anticipatory fatigue. This scale evaluates apprehensive cognition about the expectation of experiencing fatigue. The scale is based on the sum of the scores on three items ("Before starting to do anything it goes through my head that it will tire me", "I don't feel strong enough to do anything", "I get tired easily") each of which was answered on a five-point Likert-type scale: 1 "Never", 2 "Rarely", 3 "Sometimes", 4 "Often", and 5 "Always". The items were selected ad hoc by judgment of two experts from a list of items on fatigue under criteria of representativeness and relevance to the apprehensive expectation of fatigue construct. The scale was significantly correlated with other measures pertaining to the nomo-logical network of the construct such as depressive, anxiety and somatic symptomatology and has shown significant predictive values for this symptomatology (Rodríguez-Testal et al., 2016). The ordinal alpha according to Elosua and Zumbo (2008) was α = .97 for the CG and α = .98 for the NCG.
- The Fatigue Scale (Chalder et al., 1993) evaluates perceived fatigue as the set of subjective feelings of tiredness, increased effort or difficulty in starting and maintaining physical (physical fatigue) and mental (cognitive fatigue) activities which require motivation. The scale has 14 items which evaluate the severity or intensity of perceived fatigue by means of two factors, physical and cognitive fatigue. Each item refers to the last 15 days before taking the test scored on a four-point Likert-type scale. The sample in this study had internal consistency of α = .88 for the physical scale in the CG and α = .82 in the NCG; and for the mental or cognitive scale α = .85 in the CG and α = .79 in the NCG. This scale is a valid scale for discriminating between clinical and nonclinical fatigue (with 14 or 11 items: 96-100%), with a sensitivity of 75.5% and specificity of 74.5% and adequate concurrent validity with a social adaptation scale (Chalder et al., 1993; Cella & Chalder, 2010).
- The Goldberg General Health Questionnaire (GHQ-28), Spanish version (Goldberg, 1996) evaluates a wide number of symptoms related to different psychological alterations. It is a screening test which makes an overall evaluation of health and social dysfunction. It consists of 28 items grouped in four subscales on somatic, anxiety and insomnia, social dysfunction and severe depression symptoms. Internal consistency and test-retest reliability are high (α = .78 α .90) (Robinson & Price, 1982) and interevaluator reliability is excellent (high .90-.95) (Failde & Ramos, 2000). This study used three of the scales: somatic symptoms (αGC = .80, αGNC = .75), anxiety symptoms (αGC = .84, αGNC = .80), and depressive symptoms (αGC =.77, αGNC = .70).
Procedure
Before starting the study, the participants were selected by the procedures mentioned above. All of them received information on the purposes of the study and authorized the use of their data by written informed consent. Participation was voluntary and not remunerated. The CG was given the evaluation instruments in the first or second therapy session and filled it in either afterwards or at home. Diagnoses were made during clinical interview by specialized psychologist following the Diagnostic and Statistical Manual of Mental Disorders DSM- IV-TR (APA, 2000). This research was approved by the corresponding hospital bioethical committee.
Statistical analysis
First preliminary exploratory analyses, such as descriptive, comparisons of means and intercorrelation of the study variables, were done. Cohen's d was calculated to measure the effect size (Cohen, 1988). According to this author, d ≤ .20 is considered a small effect size, around .5 is a medium effect size and d ≥ .8 is a large effect size. Later the partial and interactive effects were analyzed by six hierarchical multiple regression analyses. The first step included the covariates (age and gender) as control variables, in the second step, the potential moderating variable (anticipation), in the third step the rest of the predictors (Symptomatology and population group), and finally, the product of the potential moderating variable and the predictors to find any possible interaction effects. Steps 2 and 3 of the regression analyses made it possible to explore the predictive value of anticipatory fatigue, the presence of emotional symptomatology or belonging to a group (Objective 1 and Hypothesis 1 of the study). The last step analyzed the potential interactive or moderating value of anticipation of fatigue (Objective 2 and Hypothesis 2 of the study). The minimum sample size required for a hierarchical regression analysis with medium effect size, a statistical power of 80% (Beta = .20) and risk of 95% (α = .05) is 72 subjects. Given the sample analyzed (n = 317), the statistical power achieved was 99%. All the variables were previously centered and each type of symptomatology (depressive, anxiety, and somatization) was analyzed separately for each of the dependent variables (physical fatigue and cognitive fatigue). The interaction effects found were confirmed by the procedure proposed by Hayes (Hayes, 2013).
The statistical significance was established for a 95% confidence interval and p < .05 as the criterion. All statistical analyses were done with SPSS v.19 for Windows.
Results
Preliminary exploratory analyses
A correlation analysis was done to explore the relationships among the variables (Table 1). Both physical and cognitive fatigue were significantly related to depressive, anxiety and somatic symptomatology. In first place of these correlations was the outstanding absolute value of the correlation of depressive symptomatology and perception of fatigue. In second place was somatic symptomatology and fatigue, and anxiety symptomatology and fatigue were in third place. Anticipatory fatigue was also significantly correlated with the measures of perception of fatigue (physical and cognitive) and the symptomatology evaluated, especially somatic. Age was significantly positively related to several variables. The different types of symptomatology were highly and significantly correlated. Table 1 also shows the means and standard deviations of the variables analyzed.
The differences in means between men and women were not significant except for somatic symptomatology (t (315) = -3.01, p = .03, d = -0.40, CI 95% [-3.22, -0.67]). Women (M = 8.18, DT = 4.85) showed more somatization than men (M = 6.23, DT = 4.31). The clinical group showed significantly higher levels of physical fatigue (t (127.53) = -6.29, p < .001, d = -1.12 , CI 95% [-4.74, -2.62]) and cognitive fatigue (t (117.30) = -8.81, p < .001, d = -1.63, CI 95% [-4.97, -3.15]), depressive (t (111.60) = -11.21, p < .001, d = -1.53, CI 95% [-9.30, -6.50]), anxiety (t (189.11) = -11.38, p < .001, d = - 1.51, CI 95% [-8.67, -6.11]) and somatic (t (148.82) -9.62, p .001, d = -1.58, CI 95% [-6.50, -4.35]) symptomatology, and higher levels of anticipation (t (134.45) -6.20, p < .001, < d= -1.32, CI 95% [-1.29, -0.75]).
Predictive analyses: partial and conditional effects
The study of the partial and interactive effects of the predictors on perception of fatigue was done using three groups of hierarchical regression. In each of the groups, the effects of depressive (Table 2), anxiety (Table 3) and somatic symptomatology (Table 4) were analyzed separately for physical and cognitive fatigue. Anticipatory fatigue was included separately (single effect/no partial, see Step 2 in Tables 2, 3 and 4) and combined with emotional symptomatology (partial effect, see Step 3 in Tables 2, 3 and 4) in order to analyze their contribution with and without its effect.
In all the analyses, anticipatory fatigue (total effect) contributed significantly to physical and cognitive fatigue. Perception of fatigue rose with anticipatory fatigue levels. However, the significance of this variable (partial effect) was conditioned by inclusion of one or another type of symptomatology. While anticipation remained significant after inclusion of anxiety and depressive symptomatology (physical fatigue), the first disappeared when somatic symptomatology was included. The contribution of anticipatory fatigue decreased when anxiety or depressive symptomatology was entered in the model.
Symptomatology (depressive, anxiety or somatic) showed a significant partial effect on perception of fatigue (physical and cognitive) and depressive symptomatology provided the most robust perception of fatigue, mainly physical. Somatic and anxiety symptoms also predicted perception of fatigue significantly, but to a lesser extent. Being in the clinical group was another significant predictor of perception of fatigue, but only for cognitive fatigue, not physical. This significance was similar regardless of the type of symptomatology analyzed. These results seem to show that being in the clinical group, and therefore with symptomatology, predicts a significant increase in cognitive fatigue.
The percentages of variance in fatigue explained by the models varied from 28% to 43%. In all the models explored, the highest percentage of variance was explained by the one which predicted perception of fatigue based on depressive symptomatology and being in the clinical group (41% for cognitive fatigue and 34% for physical fatigue).
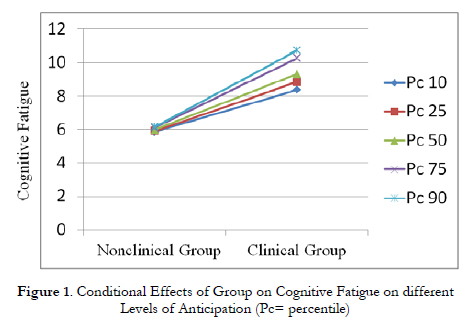
In the analysis of the moderating effect of anticipatory fatigue on the relationship between emotional symptomatology and the perception of fatigue (see Step 4 in Tables 2, 3 and 4), the regression only showed an interaction effect between group and anticipatory fatigue when the depressive symptomatology was controlled for (Table 2). To confirm and interpret this moderating effect, the interaction on cognitive fatigue was analyzed in detail. The effect of isolated interaction on cognitive fatigue was confirmed (B= .41, t (315) = 2.38, p = .01). The conditional effects of group on cognitive fatigue on anticipatory fatigue levels (10th, 25th, 50th, 75th and 90th percentiles) showed significant increase in this effect as anticipation increased only in the clinical group (β = .28, p = .008), but not in the general population group (Figure 1). The highest levels of anticipatory fatigue among the nonclinical participants did not cause significant changes in cognitive fatigue levels (β = .04, p = .53). According to the Johnson-Neyman technique, the group effect was significant when anticipation was below 3.05 on the scale.
Discussion
The double objective of this study was first to analyze effects of anticipatory fatigue, emotional symptomatology and belonging to a clinical group on the physical and cognitive perception of fatigue, and second, to analyze the possible moderating effect that anticipation of fatigue has on the relationships between emotional symptomatology or belonging to a clinical group and the perception of physical or cognitive fatigue.
For the first objective, the results showed the significant contribution that apprehensive anticipation of fatigue and presence of anxiety, somatic and especially depressive symptomatology have on perception of cognitive and physical fatigue. In agreement with the hypothesis, as a person anticipates suffering from fatigue and emotional symptomatology becomes stronger, the risk of experiencing physical or cognitive fatigue increases significantly. This risk is also increased for cognitive fatigue (not physical) in patients or clinical group, among whom symptomatology is most severe. The model including depressive symptomatology predicted perception of fatigue the best, then somatic and finally, anxiety. This alerts to the relevance of depressive symptomatology to the perception of fatigue. Anticipatory fatigue only showed a significant partial effect in combination with anxiety, although its effect disappeared when depressive or somatic symptomatology was considered, as this type of symptomatology was what was really responsible for the percentage of variance explained in the perceived feeling of fatigue.
Although these relationships have not been well explored in the literature, the results are related to studies which have observed, for example, the importance of expectation of symptoms and distress in presurgical condition on pain and postsurgical fatigue (Schnur et al., 2007), or in the context of Chronic Fatigue Syndrome (CFS), that expectation of the appearance of more symptoms with more fatigue has been corroborated and has repercussion on physical and emotional symptoms and social functioning (Priebe, Fakhoury, & Henningsen, 2008). It is relevant that when CFS patients carried out a physical activity, such as climbing stairs, anticipation of fatigue explained 21% of variance during this action (Heins et al., 2013). Catastrophism and focusing on symptoms influence this anticipation of fatigue more than disproportional fear of movement and its consequences, another indicator usually shown among CFS patients (Silver et al., 2002).
Our expectations for the second objective of this study on the moderating role of anticipatory fatigue were partially fulfilled. An interaction effect appeared between group (clinical versus nonclinical) and anticipatory fatigue on cognitive fatigue. However, this effect only emerged when the depressive symptomatology and group effect were controlled for. According to these results, being a patient and anticipating fatigue are two important variables in predicting cognitive fatigue, mainly when depressive symptomatology is controlled for. Therefore, in patients, showing a growing tendency of anticipatory fatigue predicts cognitive fatigue, however, this is not so in the general population. Nevertheless, this interaction effect did not have a relevant impact on the prediction of fatigue given the scant increase in explained variance provided the model. Again, the results impact on the main role of symptomatology in predicting perception of fatigue with special mention of depressive symptomatology.
The relationship between fatigue and anxiety and depressive symptomatology is well-known. CFS cases with depression involve more inappropriate cognitions and behaviors (Cella, White, Sharpe, & Chalder, 2013). However, a recent review on CFS emphasized cognitive biases in processing information related to the disorder's symptoms regardless of anxiety and depression symptoms, attentional and interpretive biases from the effort of assimilating and organizing the information on the illness (Hughes, Hirsch, Chalder, & Moss-Morris, 2016). All in all, in this study we referred to a component of expectation which could have a different function in outset and maintenance of general fatigue symptoms. The absence of studies found in our review which have explored the moderating effect of anticipation of fatigue impedes comparison of these results and encourages future researchers to replicate these effects.
It is important to point out the possible mediating role of symptomatology between anticipatory fatigue and its perception, according to the loss or decrease in significance it shows in the presence of such symptomatology. Therefore, this would suggest that anticipatory fatigue could increase levels of symptomatology which in turn would result in an increase in the perception of fatigue. However, this effect of mediation would require confirmation in future, more specific, analyses.
References
1. American Psychiatric Association. (2000). Diagnostic and Statistical Manual of Mental Disorders, Text Revision. DSM-IV-TR. Diagnostic and Statistical Manual of Mental Disorders - 4th Ed (Vol. 4). Washington DC: APA. [ Links ]
2. Barlow, D. (2002). Anxiety and Its Disorders. The Nature and Treatment of Anxiety and Panic (2nd ed.). New York: Guilford Press. [ Links ]
3. Brown, L., & Kroenke, K. (2009). Cancer-Related Fatigue and Its Associations With Depression and Anxiety: A Systematic Review. Psychosomatics, 50, 440-447. [ Links ]
4. Cella, M., White, P. D., Sharpe, M., & Chalder, T. (2013). Cognitions, behaviours and comorbid psychiatric diagnoses in patients with chronic fatigue syndrome. Psychological Medicine, 43(2), 375-80. https://doi.org/10.1017/S0033291712000979. [ Links ]
5. Chalder, T., Berelowitz, G., Pawlikowska, T., Watts, L., Wessely, S., Wright, D., & Wallace, E. P. (1993). Development of a fatigue scale. Journal of Psychosomatic Research, 37, 147-153. [ Links ]
6. Chaudhuri, A., & Behan, P. O. (2004). Fatigue in neurological disorders. Lancet, 363, 978-988. https://doi.org/10.1016/S0140-6736(04)15794-2. [ Links ]
7. Demyttenaere, K., De Fruyt, J., & Stahl, S. M. (2005). The many faces of fatigue in major depressive disorder. The International Journal of Neuropsychopharmacology / Official Scientific Journal of the Collegium Internationale Neuropsychopharmacologicum (CINP), 8, 93-105. https://doi.org/10.1017/S1461145704004729. [ Links ]
8. Doyle, F., Conroy, R., McGee, H., & Delaney, M. (2010). Depressive symptoms in persons with acute coronary syndrome: Specific symptom scales and prognosis. Journal of Psychosomatic Research, 68, 121-130. https://doi.Org/10.1016/j.jpsychores.2009.07.013. [ Links ]
9. Fuentes-Márquez, S., Senín-Calderón, C., Rodríguez-Testal, J.F., Carrasco-Ortiz, J.F. (2015). Perceived Experience of Fatigue in Clinical and General Population: Descriptors and Associated Reactivities. Spanish Journal of Psychology, 18, 1-8. [ Links ]
10. Goldberg, D. (1996). Cuestionario de Salud General de Goldberg. Barcelona: Masson. [ Links ]
11. Goldstein, A. N., Greer, S. M., Saletin, J. M., Harvey, A. G., Nitschke, J. B., & Walker, M. P. (2013). Tired and apprehensive: anxiety amplifies the impact of sleep loss on aversive brain anticipation. The Journal of Neuroscience: The Official Journal of the Society for Neuroscience, 33, 10607-15. https://doi.org/10.1523/JNEUROSCI.5578-12.2013. [ Links ]
12. Hayes, A. (2013). Introduction to mediation, moderation, and conditional process analysis. New York, NY: Guilford. https://doi.org/978-1-60918-230-4. [ Links ]
13. Heins, M., Knoop, H., Nijs, J., Feskens, R., Meeus, M., Moorkens, G., & Bleijenberg, G. (2013). Influence of symptom expectancies on stairclimbing performance in chronic fatigue syndrome: Effect of study context. International Journal of Behavioral Medicine, 20, 213-218. https://doi.org/10.1007/s12529-012-9253-2. [ Links ]
14. Helbig-Lang, S., Lang, T., Petermann, F., & Hoyer, J. (2012). Anticipatory Anxiety as a Function of Panic Attacks and Panic-Related Self-Efficacy: An Ambulatory Assessment Study in Panic Disorder. Behavioural and Cognitive Psychotherapy, 40, 590-604. https://doi.oig/10.1017/S1352465812000057. [ Links ]
15. Hollingshead, A. A. (1975). Five factor index of social position. Yale University: New Haven.C.T. [ Links ]
16. Hughes, A., Hirsch, C., Chalder, T., & Moss-Morris, R. (2016). Attentional and interpretive bias towards illness-related information in chronic fatigue syndrome: A systematic review. British Journal of Health Psychology, 21, 741-763. https://doi.org/10.1111/bjhp.12207. [ Links ]
17. Kluger, B. M., Krupp, L. B., & Enoka, R. M. (2013). Fatigue and fatigability in neurologic illnesses: Proposal for a unified taxonomy. Neurology, 80, 409-416. https://doi.org/10.1212/WNL.0b013e31827f07be. [ Links ]
18. Koval, P., Kuppens, P., Allen, N. B., & Sheeber, L. (2012). Getting stuck in depression: The roles of rumination and emotional inertia. Cognition & Emotion, 1-16. https://doi.org/10.1080/02699931.2012.667392. [ Links ]
19. Lindeberg, S. I., Rosvall, M., & Östergren, P. O. (2012). Exhaustion predicts coronary heart disease independently of symptoms of depression and anxiety in men but not in women. Journal of Psychosomatic Research, 72, 17-21. https://doi.org/10.1016/j.jpsychores.2011.09.001. [ Links ]
20. Lo, C. S. L., Ho, S. M. Y., & Hollon, S. D. (2008). The effects of rumination and negative cognitive styles on depression: A mediation analysis. Behaviour Research and Therapy, 46, 487-495. https://doi.org/10.1016/j.brat.2008.01.013. [ Links ]
21. Nitschke, J. B., Sarinopoulos, I., Oathes, D. J., Johnstone, T., Whalen, P. J., Davidson, R. J., & Kalin, N. H. (2009). Anticipatory activation in the amygdala and anterior cingulate in generalized anxiety disorder and prediction of treatment response. The American Journal of Psychiatry, 166, 302-310. https://doi.org/10.1176/appi.ajp.2008.07101682. [ Links ]
22. Priebe, S., Fakhoury, W. K. H., & Henningsen, P. (2008). Functional incapacity and physical and psychological symptoms: How they interconnect in chronic fatigue syndrome. Psychopathology, 41, 339-345. https://doi.org/10.1159/000152375. [ Links ]
23. Rochat, L., Billieux, J., & Van der Linden, M. (2012). Difficulties in disengaging attentional resources from self-generated thoughts moderate the link between dysphoria and maladaptive self-referential thinking. Cognition and Emotion, 26, 748-757. https://doi.org/10.1080/02699931.2011.613917. [ Links ]
24. Ruscio, A. M., Seitchik, A. E., Gentes, E. L., Jones, J. D., & Hallion, L. S. (2011). Perseverative thought: A robust predictor of response to emotional challenge in generalized anxiety disorder and major depressive disorder. Behaviour Research and Therapy, 49, 867-874. https://doi.org/10.1016/j.brat.2011.10.001. [ Links ]
25. Sáez-Francàs, N., Hernández-Vara, J., Corominas-Roso, M., Alegre-Martín, J., & Casas-Brugué, M. (2013). The association of apathy with central fatigue perception in patients with Parkinson's disease. Behavioral Neuroscience, 127, 237-44. https://doi.org/10.1037/a0031531. [ Links ]
26. Schnur, J. B., Hallquist, M. N., Bovbjerg, D. H., Silverstein, J. H., Stojceska, A., & Montgomery, G. H. (2007). Predictors of expectancies for postsurgical pain and fatigue in breast cancer surgical patients. Personality and Individual Differences, 42, 419-429. https://doi.org/10.1016Zj.paid.2006.07.009. [ Links ]
27. Rodríguez-Testal, J.F., Fuentes-Márquez, S., Senín-Calderón, C., Carrasco-Ortiz, J.F. (2016). Mediating role of emotional symptomatology between anticipatory fatigue and the perception of fatigue. Psicothema, 28, 187-193. [ Links ]
28. Silver, A., Haeney, M., Vijayadurai, P., Wilks, D., Pattrick, M., & Main, C. J. (2002). The role of fear of physical movement and activity in chronic fatigue syndrome. Journal of Psychosomatic Research, 52, 485-493. https://doi.org/10.1016/S0022-3999(01)00298-7. [ Links ]
![]() Correspondence:
Correspondence:
Juan Francisco Rodríguez-Testal.
Facultad de Psicología.
Departamento de Personalidad, Evaluación y Tratamiento Psicológicos.
Universidad de Sevilla.
C/Camilo José Cela, S/N.
41005. Sevilla (Spain).
E-mail: testal@us.es
Article received: 18-07-2016
revised: 14-10-2016
accepted: 16-12-2016

