










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.101 no.12 Madrid dic. 2009
PICTURES IN DIGESTIVE PATHOLOGY
Endoscopic resection of rectal gastrointestinal stromal tumor (GIST) using band ligation
Resección endoscópica de tumor del estroma gastrointestinal (GIST) rectal utilizando bandas elásticas
A. Ledo-Rodríguez, J. L. Ulla-Rocha1, R. Baltar-Arias1, S. Vázquez-Rodríguez1, W. Díaz-Saa1, V. González-Carrera1, L. Ledo-Barro1 and E. Vázquez-Astray1
Service of Gastroenterology. Ramón y Cajal Hospital. Madrid, Spain. 1Service of Digestive Health. Complejo Hospitalario Universitario de Pontevedra. Pontevedra, Spain
Case report
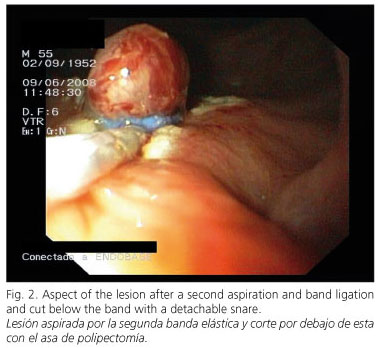
A 52 year-old male patient was referred for endoscopic resection of a 10 x 6-mm hypoechoic lesion on the anterior wall of the distal rectum. It derived from the "muscularis propria", and was deemed to be a gastrointestinal stromal tumor (GIST) from its characteristic appearance and localization as shown during endoscopic ultrasonography (EUS) (Fig. 1). An extension study proved negative. Band ligation was chosen for resection. Firstly, the tissue over the lesion was vacuumed with one band, and then a cut was performed under the band using a detachable snare. Thus, the lesion was thoroughly exposed. Afterwards, the lesion was vacuumed and a second band was placed. A new cut below the band was performed (Fig. 2), which dissected the lesion producing a perforation on the rectal wall that was sutured with Resolution clips (Boston Scientific, Natick, Mass). No further complications took place. The patient needed neither hospitalization nor prescribed antibiotics. Pathology confirmed the suspected tumor type. After six months an axial computerized tomogram (CT scan) and a EUS procedure showed no evidence of lesion relapse (Fig. 3).


Discussion
GISTs are rare tumors that arise in the digestive tract. Only about 5% originate in the rectum (1,2). Although data are scarce, it is normally accepted that complete surgical resection with negative margins is the procedure of choice for primary and non metastatic tumors (1). The endoscopic resection of gastric and duodenal lesions has been described (3,4). Resection using band ligation could represent a less aggressive alternative as compared to traditional surgery in the treatment of small sized GISTs sited in the distal rectum. However, further studies should be carried out to confirm it.
References
1. Grassi N, Cipolla C, Torcivia A, Mandalà S, Graceffa G, Bottino A, et al. Gastrointestinal stromal tumour of the rectum: Report of a case and review of literature. World J Gastroenterol 2008; 14: 1302-4. [ Links ]
2. Tran T, Davila JA, El-Serag HB. The epidemiology of malignant gastrointestinal stromal tumors: an analysis of 1,458 cases from 1992 to 2000. Am J Gastroenterol 2005; 100: 162-8. [ Links ]
3. Sun S, Ge N, Wang C, Wang M, Lü Q. Endoscopic band ligation of small gastric stromal tumors and follow-up by endoscopic ultrasonography. Surg Endosc 2007; 21: 574-8. [ Links ]
4. Sun S, Ge N, Wang S, Liu X, Lü Q. EUS-assisted band ligation of small duodenal stromal tumors and follow-up by EUS. Gastrointest Endosc 2009; 69: 492-6. [ Links ]

