










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.105 no.9 Madrid oct. 2013
https://dx.doi.org/10.4321/S1130-01082013000900015
LETTERS TO THE EDITOR
Massive upper gastrointestinal bleeding secondary to gastrosplenic fistula
Hemorragia digestiva alta masiva secundaria a fístula gastro-esplénica
Key words: Upper gastrointestinal bleeding. Gastrosplenic fistula. Gastric lymphoma.
Palabras clave: Hemorragia digestiva alta. Fístula gastro-esplénica. Linfoma gástrico.
Dear Editor,
Upper gastrointestinal bleeding (UGIB) secondary to gastrosplenic fistula (GSF) is an uncommon condition (1). We report a case of massive UGIB in the setting of a primary gastric lymphoma that infiltrated and eroded the splenic artery.
Case report
A 55-year old male presented at the emergency room with epigastric pain radiating to left hemithorax that worsened with deep breathing. In his history a recent weight loss of 5 kg stood out. He was hemodynamically stable on arrival, with low-grade fever, and the examination revealed epigastric pain with abdominal guarding and no signs of peritoneal irritation. No palpable peripheral adenopathies were observed.
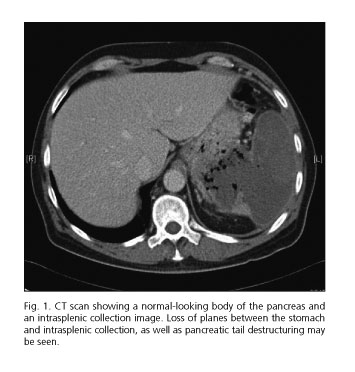
Chest X-rays demonstrated elevation of the left hemidiaphragm, and ultrasounds revealed splenomegaly with patchy, heterogeneous echo structure, which suggested an abscess. In view of these findings an abdominopelvic CT scan was performed, which showed a thickened gastric wall at the fundus level and small gas bubbles within the spleen with suspicion of intrasplenic collection (Fig. 1).
He was initially managed with antibiotics and parenteral nutrition with positive results. However, after 72 hours massive hematemesis developed, and emergency surgery was indicated. A tumor-like lesion was seen in the gastic fundus that involved the splenic hilum and parenchyma, with the tail of the pancreas being also included within the process. A gastrostomy was performed on the anterior aspect of the gastric body with clot aspiration, and arterial bleeding was unveiled as coming from the fundus, which led to an en bloc resection of the fundus of the stomach, the spleen, and the tail of the pancreas. Following surgery the patient had a favorable course; pathology was informed as a gastric large B-cell lymphoma with splenic infiltration. A bone marrow study found no neoplastic involvement.
Discussion
Malignant lymphomas of the gastrointestinal tract are uncommon conditions and represent approximately 10% of all primary lymphomas. The stomach is their most common location within the gastrointestinal tract, where they make up for 3-6% of all gastric malignancies (2-3). Management is based on both chemotherapy and radiation therapy, which obtain outcomes comparable to those of surgery in terms of survival and disease-free survival at 5 years. Surgery is reserved for medical treatment failures or associated complications (4).
GSF was first described by De Scoville et al. in 1962 as a tomographic image characterized by air in the splenic parenchyma in association with splenomegaly, which they designated as "aero-splenomegaly" (5).
Primary gastric lymphomas have a transmural, radial growth pattern. Spontaneous GSFs, as in the present case report, are extremely rare and develop in advanced disease as a result of tumor necrosis and infection arising from rapid growth; bleeding usually results from erosion of the splenic artery. Nevertheless, most GSF cases described in the literature were associated with chemotherapy onset (secondary etiology). Lastly, while bleeding cases secondary to primary gastric lymphoma have been reported, this complication is much more common in patients with primary splenic lymphoma (6,7). Thus, a patient with gastric lymphoma and bleeding should prompt consideration of potential complications as the one reported in this paper.
Julián Favre-Rizzo1, Eudaldo López-Tomassetti-Fernández1, José Ceballos-Esparragón1,
Luciano Santana-Cabrera2 and Juan Ramón Hernández-Hernández1
Departments of 1General and Digestive Surgery, and 2Intensive Medicine.
Hospital Universitario Insular de Gran Canaria. Las Palmas de Gran Canaria, Spain
References
1. García Marín A, Bernardos García L, Vaquero Rodríguez A, Menchén Viso L, Turégano Fuentes F. Spontaneous gastroesplenic fistula secondary to primary gastric lymphoma. Rev Esp Enferm Dig 2009;101:76-8. [ Links ]
2. D'Amore F, Brincker H, Gronbaek K, Thorling K, Pedersen M, Jensen MK, et al. Non-Hodgkin's lymphoma of the gastrointestinal tract: A population-based analysis of incidence, geographic distribution, clinicopathologic presentation features and prognosis. Danish Lymphoma Study Group. J Clin Oncol 1994;12:1673-84. [ Links ]
3. Arenas R. gastric lymphoma. In: Posner M, Vokes E, Weichselbaum R, editors. Cancer of the Upper Gastrointestinal Tract. London: BC Decker, Inc; 2002. p. 322-35. [ Links ]
4. McCulloch P, Ward J, Tekkis PP. Mortality and morbidity in gastro-oesophageal cancer surgery: Initial results of ASCOT multicentre prospective cohort study. BMJ 2003;327:1192-7. [ Links ]
5. De Scoville A, Bovy P, Demeester P. "Aerosplenomegalie' radiologique par lymphosarcome splenique necrosant a double fistulation dans le tube digestif. Acta Gastroenterol Belg 1967;30:841-7. [ Links ]
6. Bird MA, Amjadi D, Behrns KE. Primary splenic lymphoma complicated by hematemesis and gastric erosion. South Med J 2002;95:941-2. [ Links ]
7. Dellaportas D, Vezakis A, Fragulidis G, Tasoulis M, Karamitopoulou E, Polydorou A. Gastrosplenic fistula secondary to lymphoma, manifesting as upper gastrointestinal bleeding. Endoscopy 2011;43:E395. [ Links ]

