










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.108 no.1 Madrid ene. 2016
LETTERS TO THE EDITOR
Hemoperitoneum secondary to an spontaneous rupture of the spleen mimmicking a duodenal perforated ulcera: A case report
Hemoperitoneo por rotura espontánea de bazo no patológico en paciente fumador, simulando una perforación de ulcus duodenal: a propósito de un caso
Key words: Spontaneous rupture of the spleen. Splenomegalia. Smoking habit. Acute abdomen.
Palabras clave: Rotura espontánea de bazo. Esplenomegalia. Tabaquismo. Abdomen agudo.
Dear Editor,
Spontaneous rupture of the spleen without traumatic antecedent is a rare entity and it is usually related with the presence of pathological spleens, mainly associating with tumor, infectious or inflammatory diseases (1). We report a case of spontaneous rupture of a non-pathologic spleen in a patient with splenomegalia attributed to smoking habit.
Case report
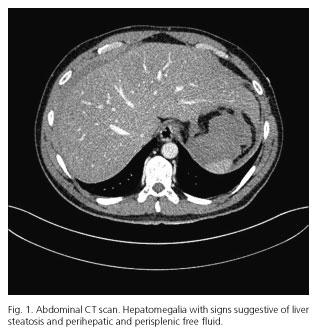
A 40-years old male was admitted to the Emergency Department of our institution for acute pain located in epigastrium and left hypochondrium during the last 12 hours before admission. The patient complained of usual epigastric pain, which improved after taking omeprazole. The patient did not refer traumatic events in the last weeks. He smoked 2 packs a day and presented a previous clinical history of polyglobulia that has been already studied and attributed to smoking habit, having ruled out polycythemia vera after bone marrow study. The patient did not refer alcoholic habit. On physical examination, the patient presented a body mass index (BMI) of 23.8 kg/m2, a heart rate of 115 bpm and the abdominal examination showed a pain located in the left upper quadrant with signs of peritonism. Laboratory data revealed a white blood cell count of 18,540 x 103 /µl, hemoglobin of 17.2 g/dl, C-reactive protein of 2.12 mg/dl and lactate 41 mg/dl, as only relevant findings. An abdominal CT scan showed hepatomegaly with steatosis and perihepatic and perisplenic free fluid (Fig. 1). Despite there was no evidence of pneumoperitoneum, the history of heartburn, abdominal examination with generalized peritonitis and free fluid observed at CT scan, perforation of duodenal ulcer was considered as the first diagnostic option. It was decided to perform an exploratory laparoscopy, aiming abundant hemoperitoneum and splenomegaly with spontaneous rupture of the inferior and medial pole of the spleen. A splenectomy was performed with stapling and section of the splenic vessels through Echelon Flex stapler® (Ethicon EndoSurgery®). The resected piece was extracted through a small left subcostal incision and a Blake drain was placed in the splenic bed. The patient recovered satisfactorily and was discharged on the 4th postoperative day. Pathologic examination showed a normal spleen.
Discussion
Spontaneous rupture of the spleen without a traumatic history is an infrequent entity, but it is usually related with the presence of pathologic spleens, mainly associated with neoplastic, infectious or inflammatory pathologies. The etiopathogenic mechanism of spontaneous splenic rupture has not been elucidated yet, but it has been postulated that many mechanisms are involved, being probably splenomegaly the most important of them, as happens in our patient. Other factors associated with spontaneous rupture of the spleen are splenic infarction, neoplastic or hematological splenic affection, cytoreductive chemotherapy... (1). It has been estimated in less than 7%, the rate of spontaneous ruptures of the spleen appearing in histologically normal visceras (2). Spontaneous rupture of a pathologic spleen is much more frequent and may occur in all the disorders that induce splenomegaly: hematological (policitemia vera, hemolytic anemia, coagulation disorders, hemofilia, Waldenström macroglobulinemia), infectious (infectious mononucleosis, cytomegalovirus, paludism, bacterian endocarditis, typhoid fever, Q fever, splenic tuberculosis, brucellosis, acute viral hepatitis, rubella, amebiasis), tumoral (leukemia, lymphoma, angiosarcoma, hamartomas), miscellaneous: Sarcoidosis, acute pancreatitis, Gaucher disease, Ehrles-Danlos disease, Niemann-Pick disease, portal hypertension, pregnancy, postendoscopia, dialysis, spleen alterations (cysts, hemangiomas, infarction, abscess, splenic artery aneurysms, cavernous hemangioma) (1).
Any cause that increases the pressure in the splenic venous territory and determines splenomegalia might favor the splenic rupture, considering this a risk factor for spontaneous rupture by itself (3). It is noted that any cause favoring splenic compression, such as the contraction of the diaphragm or the abdominal muscles, as in the mechanism of Valsalva or cough, might favor the spontaneous rupture of the enlarged spleen (1). In a smoker patient cough is a common phenomenon, simply because of irritation of the upper airway, and this could have been one of the causes that might trigger the spontaneous rupture of the spleen in the patient we present.
The association of polycythemia, splenomegaly and hepatomegaly, is characteristic of polycythemia vera, but in our patient this entity was ruled out by bone marrow study and finally all these signs were attributed to be secondary to the smoking habit. Polycythemia is defined as an increase in the red cell mass. It is characterized by an increase in the number of erythrocytes and / or the amount of hemoglobin. Poliglobulia is diagnosed when the hemoglobin level overcomes 18.5 g/dL in males and 16.5 g/dl in females. Tobacco causes tissular hypoxia secondary to carboxyhemoglobin and this triggers an increase in erythropoiesis and secondarily an increase in the red cell mass, which in turn stimulates the splenic hemocatheresis, determining the splenomegalia (4). Smoking has been also associated with non-alcoholic fatty liver disease, causing hepatomegaly and hepatic steatosis (5). Moreover, it is well known that smoking reduces the pressure of the lower esophageal sphincter, favoring the appearance of gastroesophageal reflux disease (6).
The occurrence of sudden epigastric abdominal pain with signs of peritonism, in a patient with clinical history suggestive of gastritis, should continue to guide drilling of duodenal ulcer as the first diagnostic option, even though free intraperitoneal fluid is observed at the imaging tests, but no pneumoperitoneum. However, spontaneous rupture of the spleen should be included in the differential diagnosis of this condition, especially in patients with previously known splenomegaly, but also in smokers.
Jaime Ruiz-Tovar, Gustavo Díaz, David Alias,
Montiel Jiménez-Fuertes and Manuel Durán
Department of General Surgery and Digestive Diseases.
Hospital Universitario Rey Juan Carlos.
Móstoles, Madrid. Spain
References
1. Castaño Yubero C, Perez Martin R, Mancebo Rojo Y, et al. Rotura espontánea de bazo: a propósito de un caso. SEMERGEN 2007;33:485-7. DOI: 10.1016/S1138-3593(07)73948-5. [ Links ]
2. Renzulli P, Hostettler A, Schoepfer AM, et al. Systematic review of atraumatic splenic rupture. Br J Surg 2009;96:1114-21. DOI: 10.1002/bjs.6737. [ Links ]
3. López-Tomassetti Fernández EM, Delgado Plasencia L, et al. Rotura atraumática de bazo; experiencia de 10 casos. Gastroenterol Hepatol 2007;30:585-91. DOI: 10.1157/13112586. [ Links ]
4. Pearson TC. Apparent polycythaemia. Blood Reviews 1991;5:205-13. DOI: 10.1016/0268-960X(91)90010-A. [ Links ]
5. Athyros VG, Katsiki N, Doumas M, et al. Effect of tobacco smoking and smoking cessation on plasma lipoproteins and associated major cardiovascular risk factors: A narrative review. Curr Med Res Opin 2013;29:1263-74. DOI: 10.1089/rej.2009.0840. [ Links ]
6. Rubenstein JH, Chen JW. Epidemiology of gastroesophageal reflux disease. Gastroenterol Clin North Am 2014;43:1-14. DOI: 10.3748/wjg.v21.i3.815. [ Links ]
