










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.15 no.42 Murcia abr. 2016
ADMINISTRACIÓN - GESTIÓN - CALIDAD
Implications of Psychological Harassment on Witnesses: An Observational Study in Nursing Staff
Implicaciones del hostigamiento psicológico (mobbing) sobre los testigos: Un estudio observacional en enfermería
Cardoso, Meiremar*; Fornés-Vives, Joana** and Gili, Margalida**
*RN, PhD. Hospital Universitario Son Espases, Palma de Mallorca. E-mail: meiremar.cardoso@gmail.com
**MSSc, PhD. Departamento de Psicología de la Universidad de las Islas Baleares. Palma de Mallorca, España.
ABSTRACT
Psychological harassment at work (mobbing) is considered a worldwide problem of great magnitude for nursing staff. Although hostility is described as a subjective behavior, the large number of witnesses suggests a reflection on the phenomenon.
The aim of this study is to analyze the problem of psychological harassment from the point of view of the witnesses, and to find out the psychological impact of this phenomenon on them.
We performed a cross-sectional study using self-administered questionnaires. The sample consisted of 204 nurses who were non-victims of mobbing. 28.4% (n = 58) of them reported to have observed hostile behavior toward coworkers. The most observed behaviors were professional discrediting, professional humiliation, rejection, scorn, and professional isolation. It was found that the witnesses of mobbing had significantly more symptoms of stress than non-witnesses, a greater desire to leave the profession, and a greater perception that nursing is an undervalued profession.
The results indicate that mobbing in nursing is an objective behavior and its impact reaches observers thereof, who may be secondary victims of the phenomenon. The results indicate that mobbing in nursing is an objective behavior and its impact reaches observers thereof, which could be considered secondary victims of the phenomenon.
Key words: Nursing; psychological harassment (mobbing or bullying); witnesses.
RESUMEN
El hostigamiento psicológico en el trabajo (mobbing) es un problema de considerable magnitud para el personal de enfermería a nivel mundial. Aunque el maltrato psicológico laboral esté basado en comportamientos subjetivos, el elevado número de personas que lo testifica plantea, como mínimo, una mayor reflexión sobre este tema.
El objetivo de este estudio es analizar la problemática del mobbing desde el punto de vista exclusivo de los testigos y conocer las repercusiones psicológicas del fenómeno sobre los mismos.
Se realizó un estudio descriptivo transversal, usando cuestionarios autoadministrados. La muestra está compuesta de 204 profesionales de enfermería, de los cuales el 28.4% reportaron haber testificado conductas hostiles hacia sus compañeros de trabajo. Las conductas más observadas fueron el desprestigio profesional, la humillación, el rechazo profesional, el ninguneo y el aislamiento profesional.
Los resultados demostraron que los testigos de hostigamiento psicológico, aunque no se percibían víctimas de ello, presentaban significativamente más síntomas de estrés que los no testigos, así como un mayor deseo de abandonar la profesión y una mayor percepción de que la enfermería es una profesión poco valorada. Los resultados indican que el mobbing en enfermería es un comportamiento objetivable y que su impacto repercute negativamente en los observadores del mismo, convirtiéndolos en víctimas secundarias del fenómeno.
Palabras clave: Enfermería; hostigamiento psicológico; testigos.
Introduction
Psychological harassment at work, also known as mobbing or bullying, is currently considered one of the main sources of work-related stress(1), worldwide. Mobbing, which is basically characterised by hostile behaviours, carried out at intervals and over a prolonged period of time, perpetrated by one or more people against another person, leads to a progressive isolation of the victim, who is unable to defend him or herself. The sustainability and progression of such behaviours have a negative repercussion on the wellbeing and mental health of workers(2), making them especially vulnerable to aggression. In theory, psychological harassment is conditional upon the victim's perception of it, so it could be contextualised within the transactional model of stress-coping(3), where the person's reaction and behaviour may be determined by their subjective appraisal of the event.
Psychological harassment in nursing has been identified as a problem of a considerable magnitude(4). Its impact not only affects professional, service or user dynamics (5,6), but also administrative costs(7), when it becomes associated with job dissatisfaction(8), changes from one unit to another(9), high rates of absenteeism and the wish to leave the profession(10). Scientific publications on this topic appear to have been influenced, to a certain extent, by these consequences, since the majority of studies focus their attention mainly on the victims of workplace abuse, and/or on its influence on the working environment. In this respect, few studies have analysed the impact of psychological harassment on witnesses(11), which makes it difficult to perform a more detailed analysis of how observers are influenced by the psychological abuse of another person. Furthermore, the contribution of information by these observers, provided that they do not consider themselves to be direct victims of the aggression(12), may represent an advance with regard to a more objective approach to workplace hostility. The accounts of witnesses may offer a certain degree of impartiality when quantifying and categorising hostile behaviours in the workplace, since they perceive themselves as mere spectators of these behaviours.
Although it may be difficult to affirm the neutrality of the witnesses with regard to their condition of non-victim, their presence should not be disregarded(13,14) since they represent a high percentage. In this respect, evidence points to between 17.3%(13) and over 80%(8,15). Other studies emphasise that nursing supervisors had already been witnesses of mobbing before taking up their positions(16), or that even nursing students and recently graduated nurses were victims or observers of psychological abuse(14).
Consequently, the scientific literature suggests that aggressive behaviours in nursing can often be objectified since they are perpetrated in front of other people, which leads to feelings of degradation and weakness(6), reinforcing the theory that this is a socialised behaviour(17).
Furthermore, the data show that witnesses of psychological harassment at work feel themselves to be indirectly affected and intimidated by the behaviours observed(1,18). In this respect, previous studies show that witnesses suffer from more physical and mental problems than non-witnesses, as well as from high levels of stress(2,8), lower levels of job satisfaction and reduced productivity, which has a negative repercussion on the performance of their duties(5) and consequently on the care given to users(18).
Aim of the study
The general aim of this study is to analyse the problem of mobbing from the point of view of witnesses and to discover the physical and/or psychological repercussions that the phenomenon has on them. The specific objectives are as follows:
1. To determine the percentage and the profile of the witnesses of psychological harassment of the nursing staff of a public hospital in Mallorca (Spain).
2. To identify the types of hostile behaviours most frequently observed by the witnesses.
3. To analyse the psychological impact of the harassment at work on those who observe it.
Materials and methods
A descriptive, cross-sectional study has been performed. The sample comprises nursing staff of a public hospital in Mallorca. All those surveyed were randomly selected. As a criterion for inclusion, all the participants were required to have been working in the unit for at least 4 weeks, in order to ensure that they had been exposed to different types of work-related stress factors, such as psychological harassment(19). All those who stated that they considered themselves to be victims of harassment were excluded from the sample. Total anonymity of the data has been guaranteed for all participants.
Participants
The initial study sample comprised 285 nursing professionals, whose mean age was 38.8 years (SD = 10.2), ranging from 22 to 63 years. Of the professionals surveyed, 244 were women and 41 (14.4%) were men. 186 (65.3%) of the participants were nurses, 74 (26.0%) were nursing auxiliaries and 25 (8.7%) had supervisory positions. The majority of the participants stated that they were permanent (38.6%) or temporary (45.1%), and that their work was organised in rotating shifts (69.8%). The mean professional experience of the sample was 15.2 years (SD = 10.1), whilst the length of time they had worked at the institution and in their current job was 12.6 years (SD = 10.0) and 7.3 years (SD = 7.7), respectively.
Instruments
1. Questionnaire on Sociodemographic and Employment Data prepared ad hoc for the study. This questionnaire collects sociodemographic and employment variables potentially related to psychological harassment.
2. Questionnaire on Psychological Harassment at Work - Revised Version (HPT-R)(20). This instrument is divided into 2 parts. The first part comprises 35 items and assesses the frequency of harassment behaviours of a strictly psychological nature, where those surveyed use a Likert scale of 0 to 6 points to answer. The second part includes dichotomous questions, the aim of which is to identify the perception of harassment in the previous 6 months and/or at the time of the study. In addition to identifying the origin of the mobbing, the HPT-R enquires whether or not the person surveyed has witnessed hostile acts in their workplace. The instrument has a reliability of 0.96 and its items are grouped under 5 factors (Humiliation and Personal Rejection, Professional Discrediting, Professional Rejection and Invasion of Privacy, Professional Degradation, and Scorn or Professional Isolation) which explained the variance (50.6%).
3. Questionnaire on Symptoms of Stress(21). With a reliability of 0.96, this instrument consists of 30 possible symptoms of stress that the person may experience in the light of a stressful situation. Their frequency and intensity are measured by means of a Likert scale of progressive intensity.
Statistical analysis
The statistical analyses were performed using the computer package Statistical Package for Social Sciences (SPSS) version 19 for Windows. Descriptive and inferential analyses were performed on the dependent variables and their relationship with psychological harassment in the workplace and the symptoms of stress. Student's t test was used for comparisons of means. For significant differences a probability of 0.50 was considered.
Results
To respond to the aim of the study and increase the reliability of the results, only the data reported by non-victims were analysed, whether they were witnesses or non-witnesses of hostile acts. In this respect, the sample was reduced from 285 to 204 people, of whom 32 were men and 172 women.
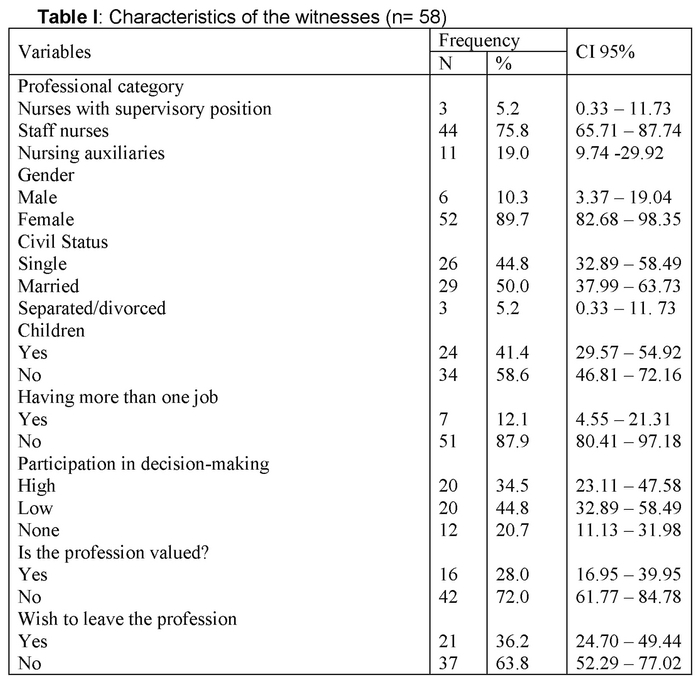
According to that proposed in the first aim of the study, the analyses of frequencies show that 28.4% of the participants (n = 58) indicated that they had witnessed the harassment of their colleagues, with staff nurses being the most habitual witnesses of hostile acts (75.9%), followed by auxiliaries (19.0%) and nurses with a supervisory position (5.2%). The majority of the witnesses were women (89.7%), were married (50.0%) and did not have children (58.6%) and only 12.1% of them also worked in another institution. Many of the witnesses indicated little (44.8%) or no (20.7%) participation in decision-making and the immense majority stated that nursing is a poorly-valued profession (72.0%). Moreover, 36.2% expressed the wish to leave their profession (Table I).
Regarding the second objective, the results indicate that the majority of the hostile behaviours observed by the witnesses in their workplace were related to problems of communication and interpersonal relationships. It was observed that behaviours such as "Negative statements or expressions of doubt regarding their responsibility or professional capacity", "Exposure to criticism by the group" or "Receipt of direct criticism regarding their way of working", were widely mentioned.
For a better understanding of the results, we chose to group the hostile behaviours observed according to the factors (F) of the HPT-R questionnaire. Thus, the hostile behaviours that comprise F1, Humiliation and Personal Rejection, were observed on average 5.4 times (SD = 4.0). F2, Professional Discrediting, presented a mean of 8.3 (SD = 7.8), F3, Professional Rejection and Invasion of Privacy, 3.6 (SD = 2.2), F4, Professional Degradation, 2.5 (SD = 3.1) and F5, Scorn or Professional Isolation, a mean of 5.7 (SD = 3.0) hostile behaviours observed (Figure 1).

Regarding the consideration of the third objective, the results show that witnesses suffer from significantly more symptoms of stress than non-witnesses. Thus, we observe that the witnesses presented higher means for the immense majority of the stress symptoms analysed. Symptoms of stress such as Nervous (M = 1.67; SD = .96), Tired, lack of energy (M = 1.36; SD = .81), Worried (M = 1.43; SD = .94), Think that people disapprove or think badly of me (M = .57; SD = .92), or Restless, jumpy (M = 1.12; Sd = .94), were those most mentioned by the observers of mobbing (Table II).

Discussion
The bibliographical review performed prior to this study revealed the lack of studies that analyse psychological harassment in nursing from the exclusive perspective of witnesses, so this could be described as a ground-breaking study. Furthermore, the results found also cast doubt on the principal characteristic of mobbing, its subjectivity, not only because the percentage of witnesses is high, but because the hostile behaviours perpetrated in the work environment can be obvious and even quantifiable.
The results of this study show that approximately a third of nursing staff are witnesses of psychological abuse suffered by their co-workers, women being the most frequent observers of such abuse. This could be attributed to the fact that nursing is predominantly a feminine group, or that female nurses are more sensitive to aggressions suffered by their colleagues.
With regard to the most widely-observed hostile behaviours, the results show that the direct attack on the nursing profession, verbal abuse and professional rejection were the most frequently observed hostile behaviours. These results corroborate previous studies(4,8,22) by revealing that psychological harassment in nursing basically consists of personal attack, the erosion of competence and professional reputation and the hindering of work(6,23). The majority of these attacks are perpetrated in public, which causes feelings of degradation and weakness(5,6), including in those who observe them. In this respect, evidence indicates that the witnesses face a difficult dilemma in view of the scope of the acts observed and their own powerlessness, which leads them to behave passively, seeking self-protection(16). This behaviour may not only fuel justification of the behaviours observed, but also contribute to a higher level of tolerance of injustice and, in short, complicity in the abuse(10). As some authors point out(18), the witnesses are afraid to confront the aggressors, which leads them to leave the victims to their own devices, thus few witnesses stand up for the victim. This feeling of powerlessness and defencelessness may justify the fact that most of the witnesses participating in this study indicated little or no participation in decision-making with regard to their work; that nursing is poorly valued or, most important, the high percentage of people who are considering leaving the profession.
Regarding the low level of participation in decision-making, this may be associated, among other things, with the employment situation that has accompanied this group throughout its history(18,24). In this respect, previous studies suggest that management in nursing is based more on fear than on respect(5,23), where changes in employment or professional dynamics do not usually take into account the training or the experience of the professional(25). Furthermore, the technical role of nursing staff is usually subordinate to medical practice, that is, to a historically more powerful group(23,26), which accentuates its tendency to adopt submissive and dependent behaviours(4). This whole context, associated with an academic education that is lacking in the development of critical thinking in the light of workplace hostility(23), makes the nursing profession very vulnerable to daily conflicts which become, in many cases, situations of complex hostility.
Regarding the perception that nursing is poorly valued and the widespread wish to leave the profession expressed by the witnesses, the results found corroborate previous studies(1,18). Thus, it was seen that the witnesses were indirectly affected by the behaviours observed, which were tolerated and even favoured by the organisation(17,23,27). The literature shows that healthcare institutions give little importance to reports of psychological abuse made by nursing staff(23,24). Furthermore, these organisations base their policy on productive efficiency and cost containment (6), and not on responding to the concerns voiced by their personnel(1,23). In this respect, there is evidence that some nursing supervisors advocate the use of intimidation as a method to attain the established targets(15,23). This makes witnesses feel powerless against the power of the harassers(17) since, not only do the latter not receive effective sanctions as a result of their behaviour(5), but they may even benefit from promotions or favourable treatment(27). Moreover, it has been revealed(27) that the witnesses perceive little support from the supervisors and the working environment is too permissive. The perception of belonging to a group that is vulnerable to such abusive behaviours and the powerlessness in this respect are factors that may justify the fact that a high percentage of witnesses is considering leaving the profession(10), especially the younger ones(23).
Our results confirm previous findings(1) by revealing that witnesses of harassment suffer from significantly more symptoms of stress than non-witnesses. The symptoms of anxiety, such as nervousness, tachycardia, restlessness, jumpiness or hopelessness, were mentioned significantly more by the witnesses than by the non-witnesses. Other symptoms that also showed significant differences between witnesses and non-witnesses were the difficulty in thinking clearly or concentrating on their work, the feeling of failure and the loss of interest in things. Thus, it could be said that the cumulative effect of harassment(6) extends beyond the victims, also reaching those who observe it. In fact, the symptoms presented by the witnesses are very similar to those mentioned by the victims of psychological abuse at work(1,23), which has a negative repercussion on their performance(5,8) and, as a consequence, on the care given to users(18). However, although the results obtained in this study seem to establish a clear relationship between witnessing psychological harassment of others and considering oneself to be affected by it, caution is necessary with regard to these interpretations, since not all witnesses are affected by the behaviours observed which some may interpret as a casual or even amusing behaviour(2). In many cases, only the victim and the perpetrators know the true nature of the hostility.
Conclusions
The study in question may be ground-breaking, since it collects information exclusively from the witnesses of psychological harassment at work, when they do not consider themselves to be victims of it. Furthermore, the sample in question belongs to one of the groups most affected by it: nursing.
The results obtained cast a doubt regarding the foundation on which the definition of psychological harassment in the workplace is built: its subjectivity. The high number of witnesses found and the information they provide suggest that this is a phenomenon based on socialised behaviours and that they are favoured by multiple organisational factors. The hostile behaviours witnessed by nursing personnel corroborate the account of many victims, by revealing that problems of communication and interpersonal relationships, such as, for example, verbal abuse or direct criticisms, are a constant factor in the setting of hostile behaviours.
The symptoms of stress presented by the witnesses lead us to think that this is a profession that is very vulnerable to psychological abuse. The negative repercussions of mobbing extend beyond the victims or, in our case, the witnesses, and may reach the users of the healthcare system. The high percentage of witnesses considering leaving nursing is also notable.
The results of this study may contribute to a better understanding of the phenomenon, to propose new challenges as to how to deal with it. One of the possible proposals would be the introduction of university training whereby the students become aware of the phenomenon and learn effective techniques with which to confront it.
Another proposal would be addressed to the professional and trade union institutions, to encourage them to make professionals aware of the importance of team spirit and of the many benefits that can be obtained. Ongoing training and the perception of support by colleagues could also be worked on more persistently. In short, the possibilities for putting a stop to workplace abuse could be a mere matter of common sense. This fact becomes more relevant when we consider that numerous studies warn that hostility against this group is a worldwide problem.
Received: January 13, 2015;
Accepted: February 28, 2015
References
1. Hansen AM, Hogh A, Persson R, Karlson B, Garde AH, Ørbaek P. Bullying at work, health outcomes, and physiological stress response. J Psychosom Res. 2006; 60(1): 63-72. [ Links ]
2. Einarsen S, Hoel H, Zapf D, Cooper C L. The concept of bullying and harassment at work: The European tradition. En: S. Einarsen, H. Hoel, D. Zapf, & C. L. Cooper (Eds.), Bullying and Emotion Abuse in harassment in the Workplace (pp. 3-40). Taylor & Francis: London, 2011. [ Links ]
3. Lazarus R S, Folkman S. Estrés y procesos cognitivos. Martínez Roca: Barcelona, 1986. [ Links ]
4. Barbosa R, Labronici LM, Sarquis LMM, Mantovani MF. Violência psicológica na prática profissional da enfermeira. Rev Esc Enferm USP. 2011; 45(1): 26-32. [ Links ]
5. Efe SY, Ayaz S. Mobbing against nurses in the workplace in Turkey. Int Nurs Rev. 2010; 57(3): 328-334. [ Links ]
6. Hutchinson M, Vickers MH, Wilkes L, Jackson D. A typology of bullying behaviours: the experiences of Australian nurses. J Clin Nurs. 2010; 19(15-16): 2319-2328. [ Links ]
7. Hoel H, Sheehan M, Cooper C, Einarsen S. Organisational effects of workplace bullying. En: S. Einarsen, H. Hoel, D. Zapf, & C. L. Cooper (Eds.), Bullying and Emotion Abuse in harassment in the Workplace (pp. 3-40). Taylor & Francis: London, 2011. [ Links ]
8. Bambi S, Becattini G, Giusti GD, Mezzetti A, Guazzini A, Lumini E. Lateral hostilities among nurses employed in intensive care units, emergency departments, operating rooms, and emergency medical service. Dimens Crit Care Nurs. 2015; 33(6): 347-354. [ Links ]
9. Hogh A, Hoel H, Carneiro IG. Bullying and employee turnover among healthcare workers: a three-wave prospective study. J Nurs Manag. 2011; 19(6): 742-751. [ Links ]
10. Vessey JA, Demarco RF, Gaffney DA, Budin WC. Bullying of staff registered nurses in the workplace: A preliminary study for developing personal and organizational strategies for the transformation of hostile to healthy workplace environments. J Prof Nurs. 2009; 25(5): 299-306. [ Links ]
11. Sims RL, Sun P. Witnessing workplace bullying and the Chinese manufacturing employee. J Manag Psychol. 2012; 27(1): 9-26. [ Links ]
12. Agervold M. Bullying at work: A discussion of definitions and prevalence, based on an empirical study. Scand J Psychol. 2007; 48(2): 161-172. [ Links ]
13. Berry PA, Gillespie GL, Gates D, Schafer J. Novice Nurse Productivity Following Workplace Bullying. J Nurs Scholarsh. 2012; 44(1): 80-87. [ Links ]
14. Simons SR, Mawn B. Bullying in the workplace - A qualitative study of newly licensed registered nurses. AAOHN. 2010; 58 (7): 305-311. [ Links ]
15. Lewis MA. Nursing bullying: Organizational considerations in the maintenance and perpetration of health care bullying cultures. J Nurs Manag. 2006; 14(1): 52-58. [ Links ]
16. Lindy C, Schaefer F. Negative workplace behaviours: an ethical dilemma for nurse managers. J Nurs Manag. 2010; 18(3): 285-292. [ Links ]
17. Katrinli A, Atabay G, Gunay G, Cangarli BG. Nurses' perceptions of individual and organizational political reasons for horizontal peer bullying. Nurs Ethics. 2010; 17(5): 614-627. [ Links ]
18. Johnston M, Phanhtharath P, Jackson BS. The bullying aspect of workplace violence in nursing. Crit Care Nurs Q, 2009; 32(4): 287-295. [ Links ]
19. EScribà V, Más R, Cárdenas M, Burguete D. Fernández R. Estresores laborales y bienestar psicológico. Rev Rol Enfer. 2000; 23(7-8): 506-511. [ Links ]
20. Fornés J, Martínez-Abascal MA, García de la Banda G. Análisis factorial del cuestionario de hostigamiento psicológico en el trabajo en profesionales de enfermería. Intern J Clin Health Psychol. 2008; 8(1): 267-283. [ Links ]
21. Manassero MA, Vázquez A, Ferrer VA, Fornés J, Fernández MC. Estrés y burnout en la enseñanza. Universitat de les Illes Balears (UIB): Palma de Mallorca, (2003). [ Links ]
22. Fornés J, Cardoso M, Castelló JM, Gili M. Psychological harassment in the nursing workplace: An observational study. Arch Psychiatr Nurs. 2011; 25(3): 185-194. [ Links ]
23. Castellón AM. Hostigamiento laboral: amenaza permanente para enfermería. Enferm. Glob. 2012; 11(28): 120-136. [ Links ]
24. Castellón AM. Occupational violence in nursing: Explanations and coping strategies. Rev Lat Am Enferm, 2011; 19(1): 156-163. [ Links ]
25. Pérez-Andrés C, Alameda A, Albéniz C. La formación práctica en enfermería en la escuela universitaria de enfermería de la Comunidad de Madrid. Opinión de los alumnos y de los profesionales asistenciales. Un estudio cualitativo con grupos de discusión. Rev Esp Salud Públ. 2002; 76(5): 517-530. [ Links ]
26. Johnson S L, Rea R E. Workplace bullying. Concerns for nurse leaders. J Nurs Adm. 2009; 39(2): 84-90. [ Links ]
27. Hutchinson M, Wilkes L, Jackson D, Vickers M. Integrating individual, work group and organizational factors: testing a multidimensional model of bullying in the nursing. J Nurs Manag. 2010; 18(2): 173-181. [ Links ]
28. Domínguez V, Regidor E, de Juanes JR, Calle ME. Sistemas de información sanitaria, registros, encuestas de salud y sistemas de notificación. En: G. Piédrola. (Ed.), Medicina Preventiva y Salud Pública (pp. 51-60). Masson: Barcelona, 2002. [ Links ]

