










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.16 no.48 Murcia oct. 2017 Epub 14-Dic-2020
https://dx.doi.org/10.6018/eglobal.16.4.267971
Revisiones
Antibullying interventions developed by nurses: integrative review
1Ribeirão Preto College of Nursing. University of São Paulo, Brazil.
2Federal University of Pernambuco. Brazil.
3University of Minho. Portugal.
Method
Integrative review conducted in six databases using descriptors related to the phenomenon and nursing. The guiding question was: “What are the anti bullying interventions developed in schools by nurses?”
Results
Five papers composed the corpus of analysis. The results indicate a variety of types of interventions (dramatization/role-playing, support group, multidimensional and videos).
Conclusions
This review presents knowledge that can support anti bullying practices and intervention programs to be developed by nurses or health teams in Brazil
Keywords Bullying; Early Intervention; Pediatric Nursing; School Health
INTRODUCTION
Bullying corresponds to a type of violence between peers characterized by intentionality, repetitiveness of aggressions and imbalance of power between aggressor and victim1. It is a phenomenon that undermines the healthy development and psychosocial well-being of school-age children and adolescents. Recent studies have shown that victims are at risk for depression, suicidal ideation, anxiety, psychosis, poor school performance and suicide2)(3)(4. Some possible causes for victimization are differences in physical appearance (skin color, overweight, thinness or some deficiency, for example), low socioeconomic status, learning difficulties or poorly developed social skills5)(6. Issues involving moral development, empathy, and relationship dynamics based on discrimination are also associated with the occurrence of bullying7)(8.
In terms of prevalence, the worldwide estimate of the number of students involved in bullying as victims is 7% to 43%, and as perpetrators, 5% to 44%9. In Brazil, the estimate is approximately 20.8% as attackers and 7.2% as victims2. In this scenario, there is a need for planning and implementing antibullying interventions effectively. Furthermore, an interface between some areas of knowledge regarding the complexity of the problem is perceived. For example, there are problems related to education and the teaching-learning process, health and illnesses, as well as problems of psychological nature that affect the integral development and socialization process of students. This perspective shows the importance of contextual and intersectoral approaches to understand the phenomenon and, consequently, to create proposals and lines of care in different directions. This is endorsed mainly by considering that bullying is not a problem confined to the environment or to the school trajectory, but a situation that affects the development and the future life of the students. Thus, this study emphasizes the contributions of health and, specifically, of nursing actions to face bullying.
Summarily, the change in the conceptual paradigm of health, which goes beyond the health/disease dichotomy and includes aspects related to the production of life in a holistic, multi-determined, procedural and social-rights-based conception, is enough to cause a problematization of care and a break with individual models of attention (10. Based on these paradigmatic changes, violence has been included in the debate agendas of the area and indications are given on the importance of articulated and intersectorial intervention models, based on the principles of health promotion, as well as aiming to improve the quality of life through integral care11.
In the school context, specifically, the interface between health and education can promote the construction of a theoretical-practical body capable of articulating the importance of integral care, by integrating the development of healthy life habits and practices and the educational process11. It is about (re)structuring health care and education practices, as well as the advent of new ways of acting in the capillarity of territories that are marked by socioeconomic conditions, especially at present due to issues of violence12)(13. Furthermore, in the case of Brazil, promoting health at school represents a possibility of interdisciplinary action whose results can be efficient and successful to guarantee emancipation and individual and collective empowerment, especially when contributing to break with cycles of violence experienced in the school.
Based on these concepts, the Health in School Program is an example of public policy on school health that was established in 2007 by the Ministries of Health and Education. Its objective is to increase the access of the students of Brazilian public schools to specific health actions, managed and conducted by primary care, through the work of professionals of this level of attention (nurses, doctors and health technicians)14. This is one of the possible starting points to think about the possible contributions of nursing to stimulate healthy behaviors, live with differences, promote quality of life, autonomy, emancipation, among others. Concerning bullying, nurses can cooperate in the planning and implementation of prevention programs and/or reducing the occurrence in schools, as well as working alongside the families of the students and the community in general (13. However, questions about the role and relevance of the nurses' work before bullying and school violence are still recurrent: Are nurses trained to deal with these issues? Are these objects of nursing care? And above all, what can nurses do?15.
Aiming at responding especially to this last questioning and considering that the policies of school health promotion in different countries, as well as social determinants of health, offer a broader perspective for nursing action, projecting it beyond the health focus, the purpose of this study was to identify and describe the antibullying interventions carried out by nurses or involving them. It is hoped that the presentation of practical experiences collaborate with care models in Brazil based on the leading role of Nursing and nurses.
METHOD
This is an integrative literature review. An integrative review allows for the formulation of global conclusions based on investigations analyzed, reflections about future research and the practical implications of the identified knowledge16. This review involved six phases: 1. formulation of a guiding question; 2. establishment of inclusion and exclusion criteria; 3. data collection; 4. critical analysis of the included studies; 5. discussion of results; 6. presentation of the integrative review17.
The guiding research question was: "What are the antibullying interventions developed in schools with the participation of nurses? ". The bibliographic search occurred in November, 2015, in the databases: PUBMED, CINAHL (Cumulative Index to Nursing and Allied Health Literature), LILACS (Latin American and Caribbean Literature on Health Sciences), PsycINFO (Psychological Information Database), SciELO (Scientific Electronic Library Online/Brasil) and Web of Science. In all databases, the following crossings were carried out: bullying AND school nursing; bullying AND school nurse; bullying AND intervention AND nursing; bullying AND school based intervention AND nursing; bullying AND prevention AND nursing. In SciELO, the Portuguese equivalente words were used.
The inclusion criteria were articles published in English, Portuguese and Spanish. All papers addressing antibullying interventions carried out in schools and that were planned, coordinated or developed by nurses were included in the study. Studies published in other languages or with interventions not performed with the participation of nurses were excluded. There was no temporal cut in the selection of the studies, in order to cover all works produced on the theme until the present day. The search and selection process was performed by an independent non-nurse researcher, and was reviewed by another non-nurse researcher. Doubts or inconsistencies were discussed until reaching a consensus.
The selected studies were summarized considering the information regarding the title, authorship, name of the journal, date of publication, country in which data were collected, intervention objectives, methods employed, main results and conclusions. The results of the review were presented in a descriptive way and critically analyzed. This treatment of data provided an overview of the scientific production in the researched topic and of the role of Nursing and nurses before the problem. At this stage of the study, the review team was interdisciplinary, composed of nurses and psychologists.
The reviewed studies were also evaluated according to methodological quality criteria. A version of the Critical Appraisal Skills Program (CASP), adapted and validated for use in Brazil, was applied in this stage18. The CASP is composed of 10 scoring dimensions and evaluates the rigor, credibility and relevance of the study under analysis. The dimensions assessed include: 1) Purpose of the study; 2) Adequacy of the methodological design to the study question; 3) Description of methodological procedures; 4) Selection criteria of the sample; 5) Details of the data collection; 6) Relationship between researcher and researched subjects; 7) Considerations on ethical aspects; 8) Rigor in the data analysis, 9) Property in the presentation and discussion of the results; 10) Research value: notes of contributions, limitations and needs of new researches18. After this evaluation, the studies were classified into two categories according to the score obtained by applying the instrument: category A - studies with good methodological quality and minimal bias, filling at least nine of the dimensions evaluated; Category B - studies with satisfactory methodological quality but with increased potential bias, including only part of the evaluation criteria adopted, at least five of the dimensions evaluated18. It is observed that this type of evaluation helps in the interpretation of the scientific evidence available and published specifically in the area of health.
Notably, all ethical principles related to the process of constructing a literature review were observed. Authorship of all the studies reviewed and of those that were incorporated into the manuscript was guaranteed, using both quotations and references. The authors also observed the guidelines of the Code of Good Scientific Practices of the Foundation for Research Support of the State of São Paulo (FAPESP)19.
RESULTS
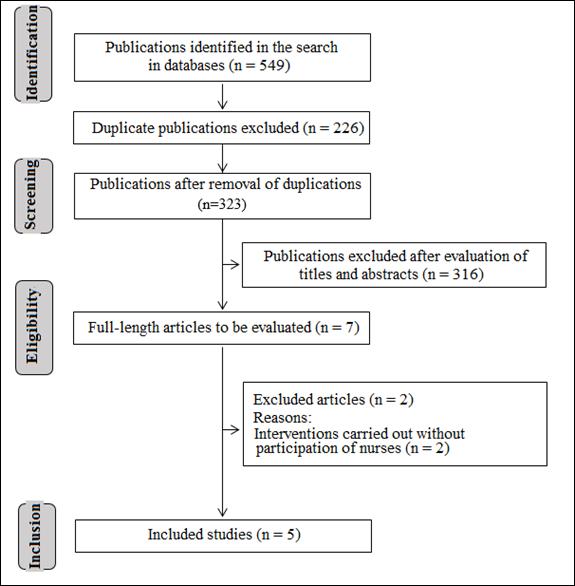
In the bibliographic search, 549 publications were found, of which 226 were excluded because of duplication due to the different crossings between the search terms and between the databases. After the analysis of titles and abstracts, eight studies were selected and, after reading the contents in full length, five met the inclusion criteria and were kept in the present review, as presented in Figure 1.
The characteristics presented by the selected articles and some bibliometric indicators are presented in Figure 2.
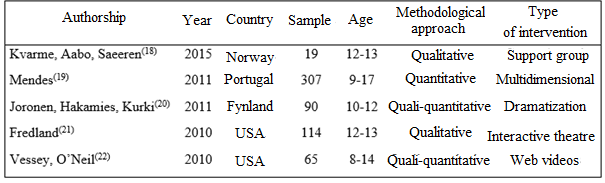
Although a temporal cut was not established in the bibliographic search, it was noticed that the studies represent recent productions, all published in the last five years. The interventions were carried out in four different countries: the United States, Finland, Norway and Portugal. No interventions with the participation of nurses in Brazil were identified. Regarding the means of dissemination, the researches were published in three journals of the Nursing area and one of the health area, namely, Journal of Community Health Nursing, Journal of the School of Nursing of USP, Scandinavian Journal of Caring Sciences and The Journal of School Nursing. English was the prevailing language. An article was published in Portuguese but also in English. The methodological approach varied between the studies (qualitative, quantitative and qualitative-quantitative). The interventions were performed with male and female participants. The size of the investigated samples varied between 19 and 307 participants, with ages ranging from 8 to 17 years. In all the studies, students participated in different forms of participation in bullying (victims, offenders and non-involved), although one focused its attention on victims and another on students with disabilities.
Figure 3 summarizes the interventions reported in the reviewed studies, their main results and the role played by nurses.
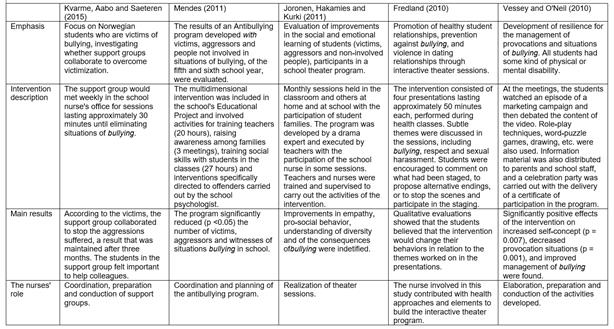
Some studies used different strategies to evaluate interventions. Following the follow-up model, Kvarme, Aabo and Saeteren20 interviewed the victims individually right after the intervention and three months later. The members of the support group participated in three focus group meetings after the intervention. Although the emphasis of one of the articles - Freeland23 - was on the establishment of partnerships with the community, a qualitative assessment was also carried out to identify, along with the students, if there would be a possibility of behavior changes in relation to the themes worked on the presentations in the school setting (adopted intervention model). After intervention activities, Joronen, Hakamies and Kurki (22 held focus groups to assess their impact and changes in the students' perspective or behavior. This strategy was also used by Vessey and O'Neil24. Mendes21 used self-report instruments with students.
Different modes of action of nurses were identified; one of them is as team leader, acting in the planning of actions or coordinating their execution. In another perspective, the nurse acts as a direct agent in the activities (when inserted in the school context as a professional) or as an interlocutor in the process of planning the actions, in a collaborative stance (when inserted in school health teams of certain localities). Attention was also drawn to the importance that studies attach to teamwork, not only with colleagues in the health area, for example, but also by including teachers and, in some cases, family and community resources.
Regarding the evaluation of the methodological quality of the studies, it was observed that only one study20 had good methodological quality and low risk of bias (category A) while the other four studies21)(24 presented satisfactory methodological quality, but with some potential risk of bias (category B). All the studies lost points in this evaluation because they did not consider the relationship between the researchers and the research participants as a potential risk element of bias in the sample selection or in the data collection process. One study21, however, did not present satisfactorily: the instruments of data collection; the rigor and the rationale of the analysis; results and discussion based on literature; and the contributions and limitations of the research (for practice, construction of knowledge, etc.).
DISCUSSION
The objective of this literature review was to identify and describe antibullying interventions carried out by nurses, since school institutions represent strategic locations for the promotion of learning in health, for healthy development of students, as well as intervention and prevention of violence and bullying25. The revised results allowed identifying what nurses have done in the international context regarding bullying at school. On the whole, it is observed that the nurses were involved in different moments of the interventions. The planning or coordinating of the proposed activities stood out, but interventions in which the nurse was the director of the activities were also seen.
Under an analytical dimension on bibliometric indicators, the small number of studies retrieved allows to infer that antibullying interventions developed by nurses have been little researched or disseminated in the scientific literature. This does not necessarily mean that they are not carried out in schools by these professionals, especially because this is a theme present in public health promotion policies of many countries, especially in the four countries where the studies analyzed in this review were developed: United States, Finland, Norway and Portugal21)(26. It is also worth noting that in the mentioned countries, the nurse is a professional who works in the school or composes school health teams responsible for actions in certain localities.
In Portugal, for example, interventions against school violence and bullying represent one of the priority health policies, ensured in the guidelines that make up the National School Health Program, whose execution is under the responsibility of multiprofessional teams, led by a nurse and a doctor21. Therefore, antibullying interventions are probably planned or implemented by nurses and/or other health professionals in other schools, but only one Portuguese study was published addressing the theme. Similarities can be identified with the Brazilian context, in which public policies also stimulate primary health care actions coordinated or performed by health teams, respecting the contextual, economic and political differences. As a rule, nurses are the coordinators of these teams or the professionals assigned for the elaboration of projects and interventions.
Thus, the low number of studies on antibullying intervention conducted by nurses and the non-occurrence of Brazilian studies can be interpreted from two perspectives. First, the editorial policies of journals must be considered, as, in general, they do not prioritize the dissemination of reports of experience. This difficulty can be overcome, as in the cases reviewed, by combining an analysis of the results of the intervention with the report of the practices. Second, the absence of national studies may indicate, in addition to this methodological aspect, a lack of understanding of bullying as an object of nursing care itself. This fact also impacts on the difficulties or facilities to publish an article with this approach and on the provision of subsidies for health teams to guide their practices.
This lack of understanding of bullying as an object of nursing care is associated with the field of some unexplored stresses. One of them is in the nurse's work at school, in the work of the health and nursing team, with the theme of violence in the perspective of health promotion. Another refers to the fact that, historically, issues of individual and curative attention in the school space have been priority to the detriment of processes of social transformation that combine the collective good. And finally, the normalized and banalized conception of peer violence, obscured by the dressing of educational styles and the behaviors supposedly expected, and by the tolerance to deviant or negative behaviors.
Regarding the form of interventions, it was noted that there were a variety of approaches. The drama/theater approach and, to a lesser extent, other modalities such as support group, videos and multidimensional intervention (involving the whole school) were more often adopted, involving a variety of activities aimed at students, school staff and students' families. The study of Mendes21, developed with a multidimensional approach, presented statistically significant results in reducing the participation of students in situations of bullying. This result is in agreement with other studies that have demonstrated that multidimensional interventions directed to the prevention or coping of bullying are better than others focused exclusively on individual student characteristics (27. One possible explanation is that human behavior is also influenced by social contingencies. Thus, broader aspects of classroom, school, family, and community contexts also need to be taken into account as determinants of social interactions signaled by violence. In this perspective, the involvement and efforts of the whole school community and the families of the students ensure positive changes in the patterns of coexistence in the school, in order to establish a culture of non-violence and transform the school environment into a safe place in the students' perceptions28.
This is the type of approach that also seems to favor the performance of different types of professionals in the interventions. It is important to highlight the role of the nurses in the planning of multidimensional intervention in partnership with other school health team professionals, as well as in the coordination of the execution of the activities by the school. Thus, the intervention of the health area in the school context requires that the functions of its professionals be redesigned and that nursing, as a science and profession, do not be restricted to the dimension of clinical assistance, but also act in different contexts, be it in the planning or in the implementation of intersectoral and integral actions13.
The multidimensional intervention analyzed here presents another relevant characteristic: the planning of a contextualized intervention, based on the diagnosis of the school. This practice is also stimulated in the primary health care. In this respect, we emphasize that the reading of the reality of the territories is fundamental to the planning of actions, aiming at the development of healthy environments. When it comes to bullying, the diagnosis makes it possible to identify the individual and social levels that are relevant to the intervention in order to direct the efforts to the circumstances, characteristics, contexts or actors directly related to its occurrence in the school13. For example, specialized literature points to the participation of families, increased supervision of adults in school settings that may facilitate the occurrence of aggressions, and a longer duration of intervention programs as directly related to success in reducing or preventing bullying26, as occurred in the study analyzed here. In summary, the diagnosis allowed the identification of central aspects for the intervention that allowed the students' social environment to be modified.
Other types of intervention identified in this review were also efficient to deal with bullying, including a specific focus on victims, developed by Kvarme, Aabo and Saeteren20. It is important to emphasize that there is still little knowledge produced about interventions targeting that particular audience. The few interventions undertaken specifically with the victims aimed at promoting more effective strategies to respond to the aggressions suffered, based on the assumption that the victims present difficulties in the administration of interpersonal conflicts3)(29. However, the feasibility of this approach aimed at improving the condition of vulnerability to situations of bullying is questioned by some researchers as they consider this as a group phenomenon, in which witnesses play a fundamental role in encouraging the aggressor or in defense of the offended peer30. This was the focus of the intervention analyzed here, which structured a victim support group made up of colleagues who volunteered to offer help. As social isolation and the lack of conditions for self-defense are two aspects that cause vulnerability to bulllying, the success of the intervention may be related to them, as it promoted the expansion of the peer network and social support to the victims.
In view of the objective of this review, we point out that the results of the studies presented bullying, as a transversal theme for health, can be addressed and prevented in schools under a variety of approaches, with possibilities for success. As the quality of the interactions of children and adolescents in school makes up an important dimension of their lives, nursing can intervene so as to reduce the negative impact that bullying has in terms of learning, training, health and quality of life of students15. It is, therefore, necessary to create coping strategies in social life, and consider the role that individual empowerment strategies can take on reality and on the change of the way relationships are constructed, as occurred in the intervention involving support groups developed by Kvarme, Aabo and Saeteren20. This is an important perspective health promotion and education practices in primary care, since individual empowerment allows the development of community (collective) empowerment. Such empowerment is fundamental in cases of bullying, since it may represent a stimulus to the establishment of a culture of non-violence in school, for example.
The intervention developed by Vessey and O'Neill24 with videos, role-play techniques, word-puzzle game, drawing, among others, was also effective to increase the self-concept, reduce provocation situations and better management of situations of bullying among participants. The success of the program developed with physically or mentally disabled children can also be explained from the perspective of individual empowerment, as well as social support and increased peer networking. In the same perspective follow the two studies carried out with theatrical methodology22)(23, whose results indicated improvements in relation to empathy, pro-social behavior, understanding of diversity and of the consequences of bullying. This is because dramatization encourages participants to reflect on their real conflicts through active participation, improves dialogic and corporal expression, and encourages autonomy.
In all the interventions, the students participated in different stances in the bullying (victims, offenders and non-involved), although one study focused its attention on victims and another on students with disabilities. Although only a small percentage of students are directly involved in the aggressions, this initiative can be important to encourage the contact of victims and aggressors with other students non-involved in the bullying and that can serve as a model of pro-social conduct to the aggressors and/or offer support to the victims.
Regarding the methodological quality of the reviewed studies, it was observed that all were classified as having a high level of evidence. However, considering that some studies included in data collection or in the development of intervention strategies by professionals inserted in the schools (teachers or nurses), only two studies20)(22 considered the researcher/participants relationship as a limitation. This is a methodological fragility that signals an absence of criticism and acknowledgment of potential biases of this nature that impact on how students may behave during interventions or during the completion of assessment instruments at these moments. None of the reviewed studies described adjustments that were made to control this type of problem or its implications for the data.
Finally, the different forms of involvement of the nurses in the interventions carried out, from their planning to their implementation, stand out. Promoting interventions with differentiated methodologies beyond the possibilities of nursing action requires the establishment of partnerships and articulation with other professionals. To recognize the real possibilities for nurses to act in the school is also relevant to the success of the activities developed. In these cases, in particular, these professionals are required to have planning, articulation and management skills, as occurred in the study developed by Fredland23, whose planning was carried out by nursing professionals in partnership with a theater company that was responsible for the execution of the intervention. These aspects emphasize the importance of training and of changes and increase in the logic of understanding the care process.
According to the Care Line for Integral Attention to the Health of Children, Adolescents and their Families in Situation of Violence12, learning and being able to identify different forms of manifestation of violence affecting children and adolescents is fundamental to offer care, especially in public health services. This Line also includes bullying as one of the daily problems of school-age children and adolescents. The same occurs with the document of the Health in the School Program,14 which presents guidelines for actions in primary care in the country focusing on the inclusion of education and health promotion measures to prevent violence and stimulate the construction of a culture of peace. However, the guidelines of these documents still do not respond to the questions raised in the introduction of the present article (Are nurses trained to act in this direction? Is bullying an object of nursing care? What can nurses do?). Nurses and other health professionals still face many difficulties to carry out actions when faced with limiting situations or violence, and especially when they occur in a context that is hardly seen as their work environment, such as schools.
It was the recognition of these limitations that stimulated the development of the present review. At the same time, the revised results indicate actions that can be developed by nurses, as well as by other health professionals to prevent and cope with bullying. First, primary care nurses can contribute to the diagnosis of the issue in the communities attached to the family health strategy teams. As noted, this is one of the essential steps in the definition of intervention programs. Secondly, spaces and groups with school-age children and adolescents can be created based on the perspective of health education. These moments facilitate the sharing of experiences, the elucidation of doubts and the construction of a network of social support. In addition, methods such as those used by some of the revised studies, as theater and dramatization of problem situations/conflict resolution strategies, can be adopted. In another direction, thirdly, in the Brazilian case, primary care nurses can work with families to build links and enhance human rights, principles of solidarity and tolerance of differences. These professionals can also help those responsible for children and adolescents to identify signs of victimization or even aggressive practices in the school context. These are actions that can be developed in home visits, for example. These are broad demands and perspectives.
In addition, it is important to emphasize that attention to children and adolescents involved in situations of bullying in the school context, whatever the amplitude of this phenomenon, implies a work focused on protection and promotion of quality of life, including the promotion of health in defense of life. This work also includes a dimension that should integrate multiple sectors, both in macro-structural aspects such as public social policies, and in the articulation and integration of different sectors and services in the perspective of intersectoriality and integrality, defining and establishing support and protection networks. The diagnosis, treatment, rehabilitation and maintenance of health involves recognizing that nursing actions in the attention to violence in childhood and adolescence should be guided by the principles of universality, accessibility, coordination, bonding, continuity, completeness, accountability, humanization and equity. Thus, the necessary involvement of nurses in intervention programs linked to health promotion and integral care strategies in the school environment, in the perspective of an emancipatory model, seeking the empowerment and participation of the involved subjects, is reiterated.
FINAL REMARKS
The inclusion of nursing professionals in schools in countries with different socioeconomic realities for development of educational health interventions in partnership with the school community has generated positive effects to bullying prevention and coping. In this sense, this review provided evidence of a diversity of antibullying methodologies and strategies used by nurses. In short, the apprehension of different educational approaches has demonstrated the need for educational planning that considers the specificities, interests and expectations of each group; ensures the availability of audio visual resources and educational technologies; and also is based on the interaction of these resources with the target public of the actions.
The reviewed studies allowed us to perceive that the role of Nursing in the fight against bullying should be configured as educational intervention based on the use of active methodologies and having as central axis the broad participation and stimulus to the protagonism of the school-age childred or adolescents in the production of critical and reflexive knowledge about the phenomenon and its consequences. In practical terms, professionals in this area should not only deal with the treatment of health problems and the quality of life of students, but propose training actions for the school community to recognize the problem and how to combat it, prepare informative material (booklets, posters and folders) to be distributed to students, parents and guardians, and assist parents and guardians to identify the involvement of children in bullying situations, whether as a victims or aggressors.
The small size of the samples from the reviewed studies makes it impossible to generalize the results, since none was developed with a representative sample and others were pilot studies. Investigations with larger samples are necessary and could be developed in Brazil, since no research in the national territory was found in the databases consulted. Another limitation identified was the lack of evaluation of the impact of the distributed materials on parents, teachers and school employees on the reduction ofbullying. Future research may develop strategies for evaluating the different components that make up the interventions, in order to better specify the contribution offered by each one in particular. It is also important to highlight the absence of control groups to compare with the students participating in the interventions.
Finally, the oustanding points of this study and its contribution to Nursing and knowledge about bullying are listed as follows: 1. Strategies of nursing performance in face of a recognized public health problem are presented, although they are little explored or disseminated in the scientific literature; 2. International experiences were synthesized, with indicators of success in the interventions, which may guide the construction of intervention models in Brazil, with the nurses as protagonists; and 3. The study contributes to the dissemination of scientific production on an object of care of the interest of Nursing, but still little researched by this area in Brazil. Faced with this scenario, research on bullying in the area of health and nursing is stimulated in addition to the dissemination of results of interventions developed by professionals in these areas.
REFERENCIAS
1. Olweus D. School bullying: Development and some important challenges. Annu Rev Clin Psychol. 2013;9:751-80. [ Links ]
2. Malta DC, Porto DL, Crespo CD, Silva MMA, Andrade SSC, Mello FCM, et al. Bullying in Brazilian schoolchildren: Analysis of the National Adolescent School-based Health Survey (PeNSE 2012). Rev Bras Epidemiol. 2014;17:92-105. [ Links ]
3. Stan C, Beldean IG. The development of social and emotional skills of students - ways to reduce the frequency of bullying-type events. Experimental results. Procedia Soc Behav Sci. 2014;114:735-43. [ Links ]
4. Williford A, Boulton AJ, Jenson JM. Transitions between subclasses of bullying and victimization when entering middle school. Aggress Behav. 2014;40(1):24-41. [ Links ]
5. Bejerot S, Edgar J, Humble MB. Poor performance in physical education - a risk factor for bully victimization. A case-control study. Acta Paediatr. 2011;100(3):413-9. [ Links ]
6. Oliveira WA, Silva MA, Mello FC, Porto DL, Yoshinaga AC, Malta DC. The causes of bullying: results from the National Survey of School Health (PeNSE). Rev Latino-Am Enfermagem. 2015;23(2):275-82. [ Links ]
7. Caravita SS, Sijtsema J, Rambaran JA, Gini G. Peer influences on moral disengagement in late childhood and early adolescence. J Youth Adolesc. 2014;43(2):193-207. [ Links ]
8. Russell ST, Sinclair KO, Poteat VP, Koenig BW. Adolescent health and harassment based on discriminatory bias. Am J Public Health. 2012;102(3):493-95. [ Links ]
9. Cook CR, Williams KR, Guerra NG, Kim TE. Variability in the prevalence of bullying and victimization: A cross-national and methodological analysis. In: Jimerson SR, Swearer S, Espelage DL. Handbook of bullying in schools: An international perspective. New York: Routledge/Taylor & Francis Group; 2010. [ Links ]
10. Westphal MF. Promoção da saúde e prevenção de doenças. In: Campos GWS, Minayo MCS, Akerman M, Drumond Júnior M, Carvalho YM. Tratado de Saúde Coletiva. 2. ed. São Paulo (SP): Hucitec; Rio de Janeiro (RJ): Fiocruz; 2012. [ Links ]
11. Minayo MCS. O desafio do conhecimento: pesquisa qualitativa em saúde. 11. ed. São Paulo: Hucitec, 2012. [ Links ]
12. Ministério da Saúde. Metodologias para o cuidado de crianças, adolescentes e famílias em situação de violências. Brasília: Ministério da Saúde, 2014. [ Links ]
13. Silva MAI, Silva JL, Pereira BO, Oliveira WA, Medeiros M. The view of teachers on bullying and implications for nursing. Rev Esc Enferm USP. 2014;48(4):723-30. [ Links ]
14. Ministério da Saúde. Saúde na escola (Cadernos de Atenção Básica n. 24). Brasília: Ministério da Saúde, 2009. [ Links ]
15. Silva MAI. Bullying entre pares na escola: desafio aos enfermeiros que atuam na atenção básica à saúde. Rev Eletrônica Enferm. 2013;15(3):603-04. [ Links ]
16. Galvão CM, Mendes KDS, Silveira RCCP. Revisão integrativa: método de revisão para sintetizar as evidências disponíveis na literatura. In: Brevidelli, MM, Sertório SCM. Trabalho de conclusão de curso: guia prático para docentes e alunos da área da saúde. São Paulo (SP): Iátria; 2010. [ Links ]
17. Souza MT, Silva MD, Carvalho R. Revisão integrativa: o que é e como fazer. Einstein. 2010;8(1):102-06. [ Links ]
18. Carvalho, K.E.G. Cuidado de enfermagem ao adolescente: proposta de educação em saúde sobre o preservativo masculino. [Dissertação]. 114f. Universidade Federal de Pernambuco. Programa de Pós-Graduação em Enfermagem. Universidade Federal de Pernambuco: Centro de Ciências da Saúde, 2012. [ Links ]
19. Fundação de Amparo à Pesquisa do Estado de São Paulo. Código de Boas Práticas Científicas. São Paulo: FAPESP, 2014. [ Links ]
20. Kvarme LG, Aabo LS, Saeteren B. From victim to taking control: Support group for bullied schoolchildren. J Sch Nurs. 2015;1-8. [ Links ]
21. Mendes CS. Preventing school violence: an evaluation of an intervention program. Rev Esc Enferm USP. 2011;45(3):581-8. [ Links ]
22. Joronen K, Häkämies A, Astedt-Kurki P. Children's experiences of a drama programme in social and emotional learning. Scand J Caring Sci. 2011;25(4):671-88. [ Links ]
23. Fredland NM. Nurturing healthy relationships through a Community-based Interactive Theater Program. J Community Health Nurs. 2010;27(2):107-18. [ Links ]
24. Vessey JA, O'Neill KM. Helping students with disabilities better address teasing and bullying situations: A MASNRN study. J Sch Nurs. 2010;27(2):139-48. [ Links ]
25. Brito AKA, Silva FIC, França NM. Programas de intervenção nas escolas brasileiras: uma contribuição da escola para a educação em saúde. Saúde debate. 2012;36(95):624-32. [ Links ]
26. Kub J, Feldman MA. Bullying prevention: A call for collaborative efforts between school nurses and school psychologists. Psychol Schools. 2015;52(7):658-71. [ Links ]
27. Ttofi MM, Farrington DP. Effectiveness of school-based programs to reduce bullying: A systematic and meta-analytic review. J Exp Criminol. 2011;7(1):27-56. [ Links ]
28. Skrzypiec G, Slee P, Murray-Harvey R, Pereira B. School bullying by one or more ways: Does it matter and how do students cope? Sch Psychol Int. 2011;32(3):288-311. [ Links ]
29. Faria CS, Martins CBG. Violencia escolar entre adolescentes: condiciones de vulnerabilidad. Enferm. glob. Abr. 2016; 15(42):157-170. [ Links ]
30. Berry K, Hunt CJ. Evaluation of an intervention program for anxious adolescent boys who are bullied at school. J Adolesc Health. 2009;45(4):376-82. [ Links ]
31. Kärna A, Voeten M, Little TD, Poskiparta E, Kaljonen A, Salmivalli C. A large-scale evaluation of the KiVa anti-bullying program: Grades 4-6. Child Dev. 2011;82(3):311-30. [ Links ]
Received: September 18, 2016; Accepted: November 06, 2016
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
