










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.17 no.49 Murcia ene. 2018 Epub 14-Dic-2020
https://dx.doi.org/10.6018/eglobal.17.1.271551
Originales
Body Mass Index and associated factors in climacteric women
1Master degree in Primary Healh Care at State University of Montes Claros – UNIMONTES. Professor at Faculdades Integradas do Norte de Minas - FUNORTE, Montes Claros, Minas Gerais, Brazil.
2 Master degree in Health, Society and Environment at Federal University of Vales do Jequitinhonha e Mucuri – UFVJM. Professor at Faculdades Integradas do Norte de Minas – FUNORTE, Montes Claros, Minas Gerais, Brazil.
3 Medical student at Faculdades Integradas Pitágoras - FIPMoc, Montes Claros, Minas Gerais, Brazil.
4 Ph.D. student in Health Sciences at State University of Montes Claros – UNIMONTES. Professor at State University of Montes Claros – UNIMONTES and at Faculdades Integradas do Norte de Minas - FUNORTE, Montes Claros, Minas Gerais, Brazil.
5 Ph.D. student in Odontology at Federal University of Minas Gerais – UFMG. Professor at Post-graduation program in Primary Health Care at State University of Montes Claros – UNIMONTES, at Faculdades Integradas Pitágoras – FIPMoc and at Faculdades Integradas do Norte de Minas – FUNORTE, Montes Claros, Minas Gerais, Brazil.
6 Ph.D. in Halth Sciences at University of Brasília – UnB. Professor at Post-graduation program in Primary Health Care at State University of Montes Claros – UNIMONTES and at Faculdades Integradas Pitágoras – FIPMoc, Montes Claros, Minas Gerais, Brazil.
Goal
To identify the association between body mass index and sociodemographic factors, lifestyle, eating habits, anthropometric measurements and clinical factors of climacteric women assisted in Health Strategies of Montes Claros.
Methods
This is a cross-sectional, analytical epidemiological study with a sample of 874 perimenopausal women selected by simple random sampling. Sociodemographic data, lifestyle, eating habits, and clinical, obstetrical and gynecological factors were collected through standardized questionnaires, in addition to performing anthropometric assessment. The bivariate analysis was performed using the chi-square test.
Results
The results showed high prevalence of obesity (36.0%) and overweight (38.1%), as well as associations between body mass index and the the type of school attended (p = 0.009), smoking (p = 0.023), treatment for weight loss (p = 0.000), anthropometric measurements (p = 0.000) and clinical factors (p = 0.000).
Conclusion
We conclude that educational interventions to correct or improve the anthropometric profile may result in benefits for the health of climacteric women, since the presence of obesity and overweight was high, and lifestyle habits, anthropometric and clinical factors present themselves associated to morbidity.
Keywords Body Mass Index; Climacteric; Family Health Strategy
INTRODUCTION
Climacteric is a biological and non-pathological phase characterized by the establishment of a continuous and progressive physiological process of hypoestrogenism 1. The influence of endogenous and exogenous factors in this period intensifies the alteration of the lipid profile, which generates a predisposition to weight gain, changes in body composition and consequently triggers obesity 2)(3.
Obesity advent brings an increase to a set of risks for other chronic diseases such as diabetes, hypertension, depression and multiple neoplasias 4. Its striking features are the increased adiposity located in the abdominal region or generalized. 5. Studies have been conducted to characterize obesity risk factors in climacteric women; however, the risk impact of each of these factors is not yet clearly defined in the literature6) and causes controversy 6)(7.
Obesity stands out as being both a disease and a risk factor for the onset of other comorbidities8, associated with the scarcity of data about this pathology in climacteric women assisted in primary care 9. Therefore, the study aimed to identify the association of Body Mass Index (BMI) with sociodemographic factors, life habits, eating habits, anthropometric measures and clinical factors of climacteric women assisted in the Montes Claros Health Strategies.
MATERIALS AND METHODS
The present work comprises an analytical cross-sectional epidemiological study. The target population corresponded to the climacteric women of the city of Montes Claros, Minas Gerais, made up of 30,018 climacteric women registered in the 73 Family Health Strategy (FHS) units of Montes Claros, Minas Gerais, in 2014.
Sample selection occurred in two stages. Initially, the strategies were selected by conglomerates, making a total of 20 strategies, which covered the rural and urban areas. After that, a proportional number of women was selected obeying the stratification criteria according to the climacteric period (pre, peri and postmenopausal)10, identified through the records available in the units. After that selection, the family health agents invited these women go to the unit on the date established by the invitation. For each unit, 48 women were selected, making a total of 960 women called, of who 113 climacteric women were lost in the study because they did not complete all the evaluations. The final sample corresponded to 874 climacteric women. To incorporate the structure of the complex sampling plan into the statistical analysis of the data, each interviewee was associated with a weight w, which corresponded to the inverse of their probability of inclusion in the sample (f)11.
Trained and calibrated professionals performed the data collection. Socio-demographic data, life habits and clinical factors were collected through questionnaires. The presence of diabetes mellitus and systemic arterial hypertension were self-reported by the interviewees. Anthropometric data such as waist circumference, waist-hip ratio and BMI were evaluated. Measurement of stature occurred with the help of the SECA 206 anthropometer on a wall with ninety degrees in relation to the floor and without skirting boards with the woman in proper position to evaluate this data. We used the SECA OMEGA 870 digital scale for measuring weight (kg). BMI was the result of the division of the body weight by the squared height (P / E2). It caused the classification of those surveyed in eutrophic (18.5-24.9), overweight (25.0-29.9) and obesity (30.0- above)12.
Abdominal circumference (AC) and waist -hip ratio (WHR) were evaluated using an inelastic millimeter tape measure in regions and with a standardized technique. Values ≥ 88 cm in AC were classified as altered according to NCEP/ATP-III13 and 0.80 in WHR, according to Molarius et al.,14.
We selected the independent variables considering the following dimensions: sociodemographic data (age, marital status, skin color, education, minimum wage, religion, school attended, paid activity and profession); lifestyle (physical activity, smoking, alcoholism and treatment to lose weight); dietary habits (salt in food, fruit intake per week, weekly soda intake and red meat fat intake); clinical factors (menopause, self-perception of depression, diabetes, and blood pressure); obstetric and gynecological factors (normal births, weight of the first child at birth, woman's hormone, type of menopause).
For statistical analysis, we used the SPSS 20.0 software. Initially, we described the simple frequencies and percentages of the analyzed variables. Bivariate analysis was performed using the chi-square test. In all statistical analyzes, statistical significance was considered p <0.05.
The research project was approved by the Research Ethics Committee of Faculdades Integradas Pitágoras of Montes Claros with opinion n. 817.666 (CAAE 36495714.0.0000.5109). Only the women who signed the Free and Informed Consent Term participated in the study. This study meets the regulatory norms of research involving human beings - Resolution n. 466/12 - of the National Health Council.
RESULTS
We evaluated 874 climacteric women between the ages of 40 and 65. It was observed that the majority of the women were between 52 and 65 years old (45.3%), married (69.8%) and brown skinned (64.8%). As for schooling, the majority had complete primary education (68.2%), received up to a minimum wage (63.8%), were Catholic (66.9%), attended public schools (97.3%), did not work (59.6%). Regarding the profession, the majority of women reported working in domestic services (42.1%) (Table 1).
Table 1 Characterization of the sample according to sociodemographic factors of climacteric women, Claros, Minas Gerais Montes, 2014.
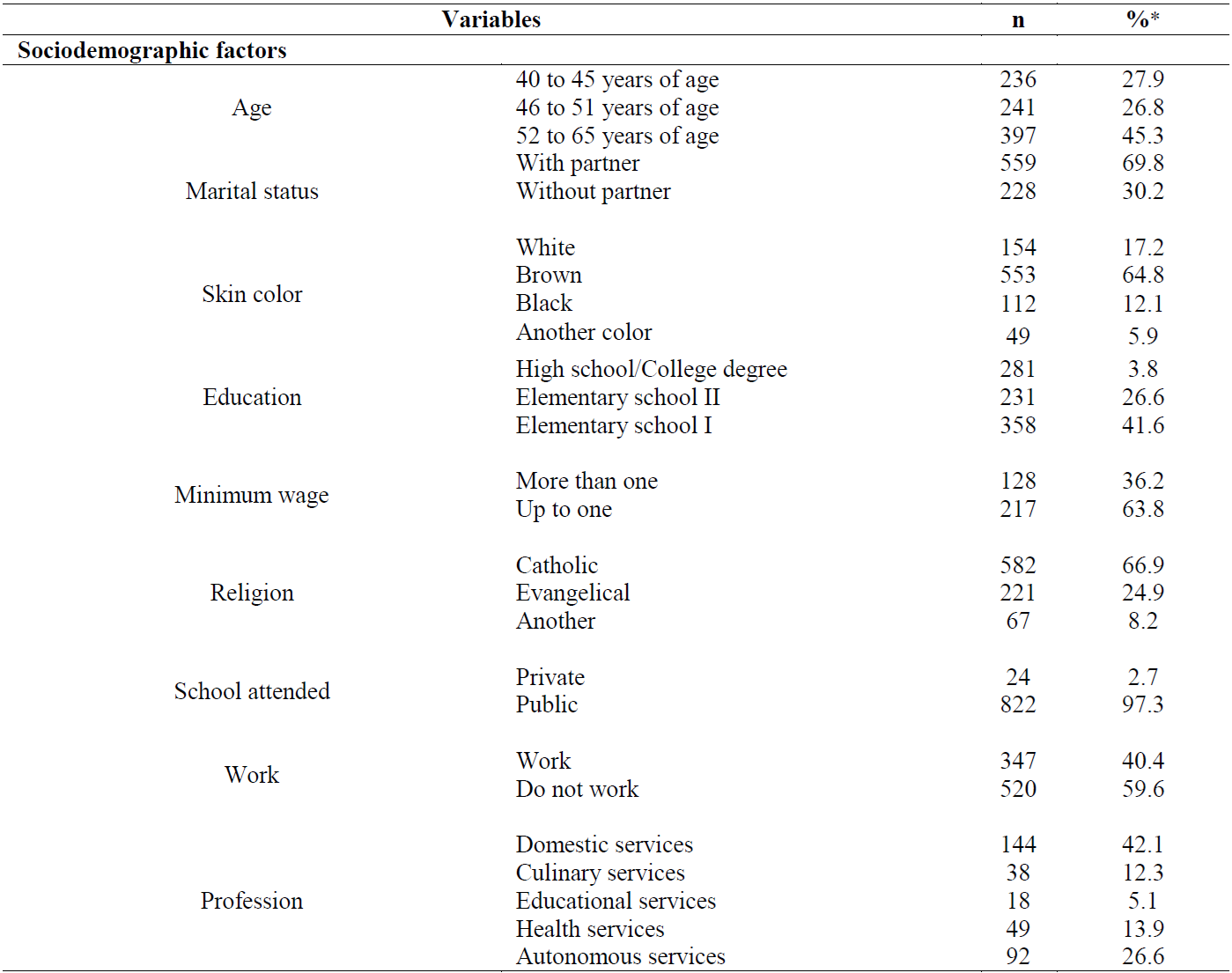
*: Corrected by the drawing effect (deff).
The practice of irregular physical activity was reported by (55.7%). Women reported they were not smokers (89.8%), they did not ingest alcohol (21.2%) and they did not have treatment for the weight loss (78.0%). Regarding eating habits, a large number of women reported to never salt in food (78.8%), to eat fruit 3 to 6 times a week (70.6%), not to drink soft drinks weekly (50.8% %), and the majority affirmed to remove the fat from red meat (80.5%). As for the anthropometric measurements, the AC of the majority of the women had altered (84.7%) and in the BMI, there were prevalence of overweight (38.1%) and obese (36.0%) women (Table 2).
Table 2 Characterization of the sample according to life habits, eating habits and anthropometric measurements in climacteric women, Montes Claros-MG, 2014.
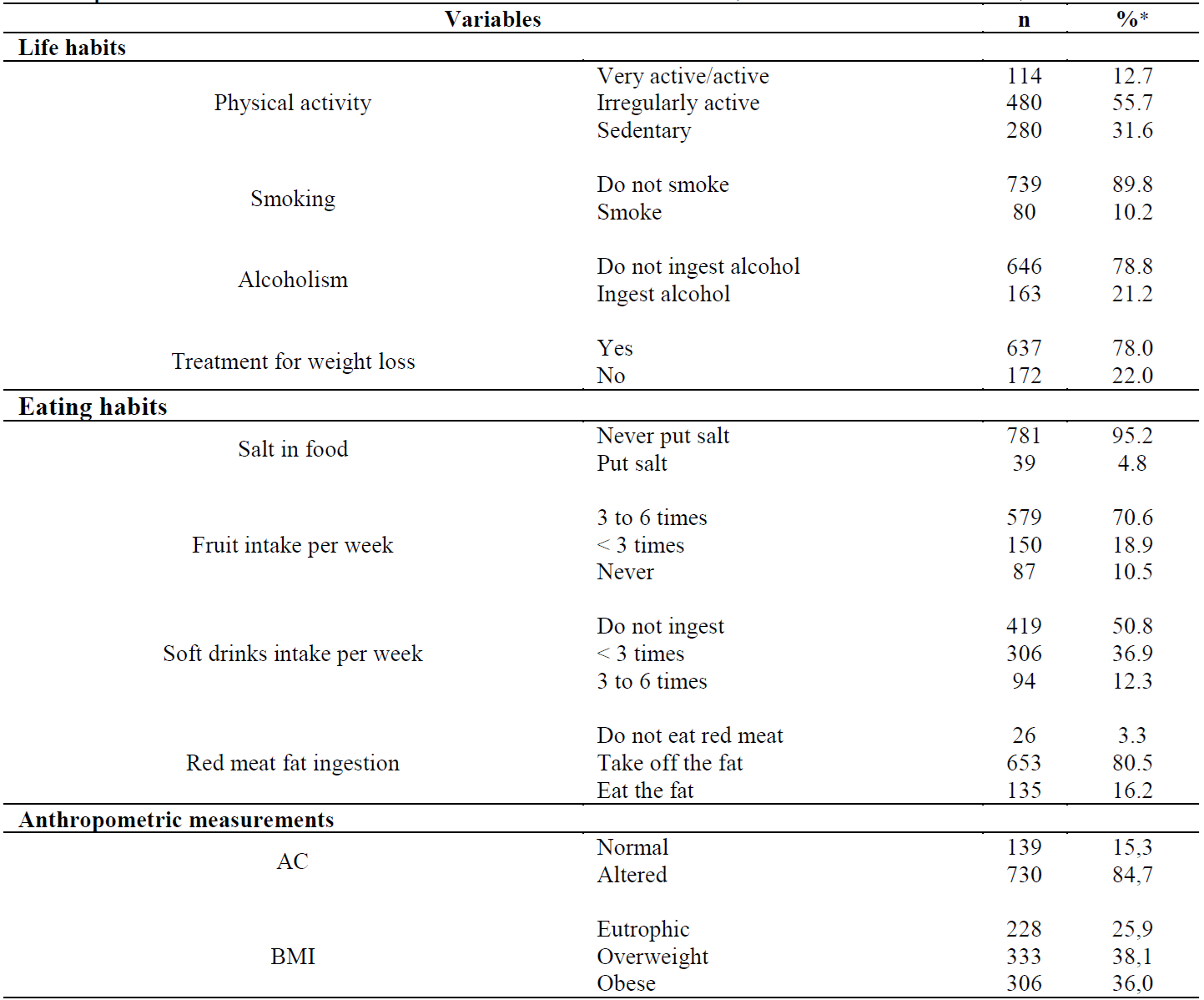
*: Corrected by the drawing effect (deff); AC: Abdominal circumference.
Regarding the menopausal phase, most women were postmenopausal (43.9%), non-diabetic (84.9%), non-hypertensive (51.0%), and had a good health (44.1%) (Table 3).
Table 3 Characterization of the sample according to clinical, obstetric and gynecological factors of climacteric women, Montes Claros-MG, 2014.
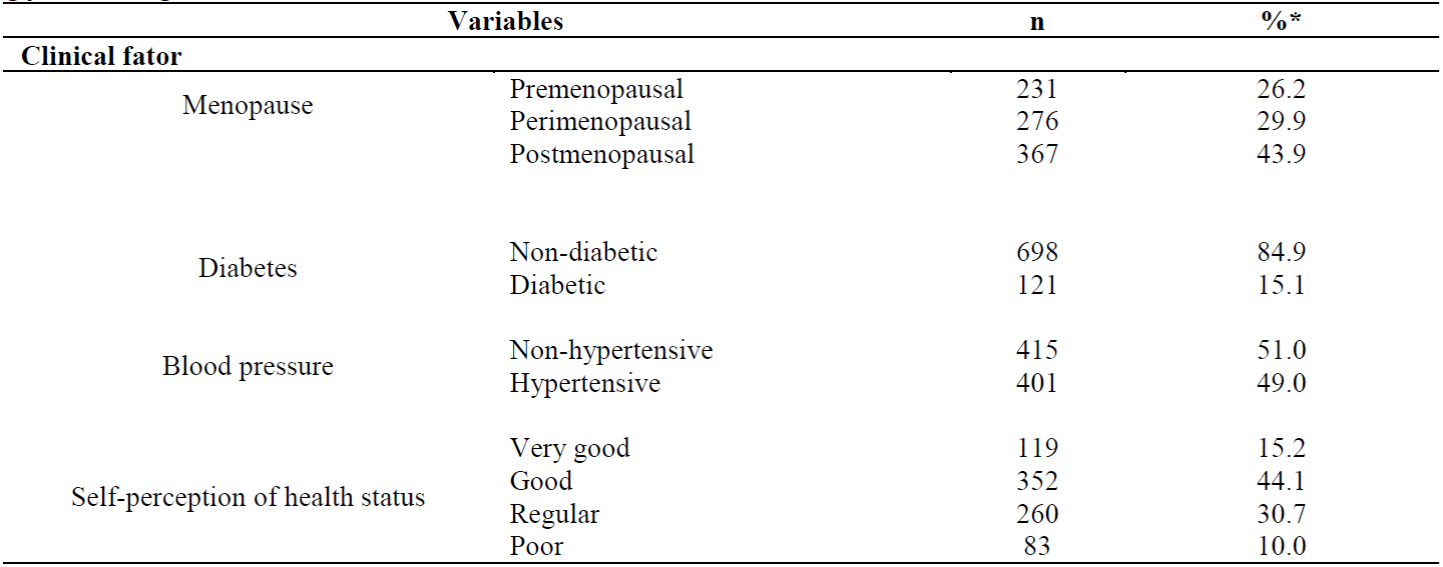
*: Corrected by the drawing effect (deff).
Table 4 shows the association of BMI levels among sociodemographic factors. There was a significant association between BMI changes and the school-attended variable (p = 0.009). Among women attending private schools, they had higher rates of overweight and obesity.
Table 4 Association of BMI levels among sociodemographic factors.
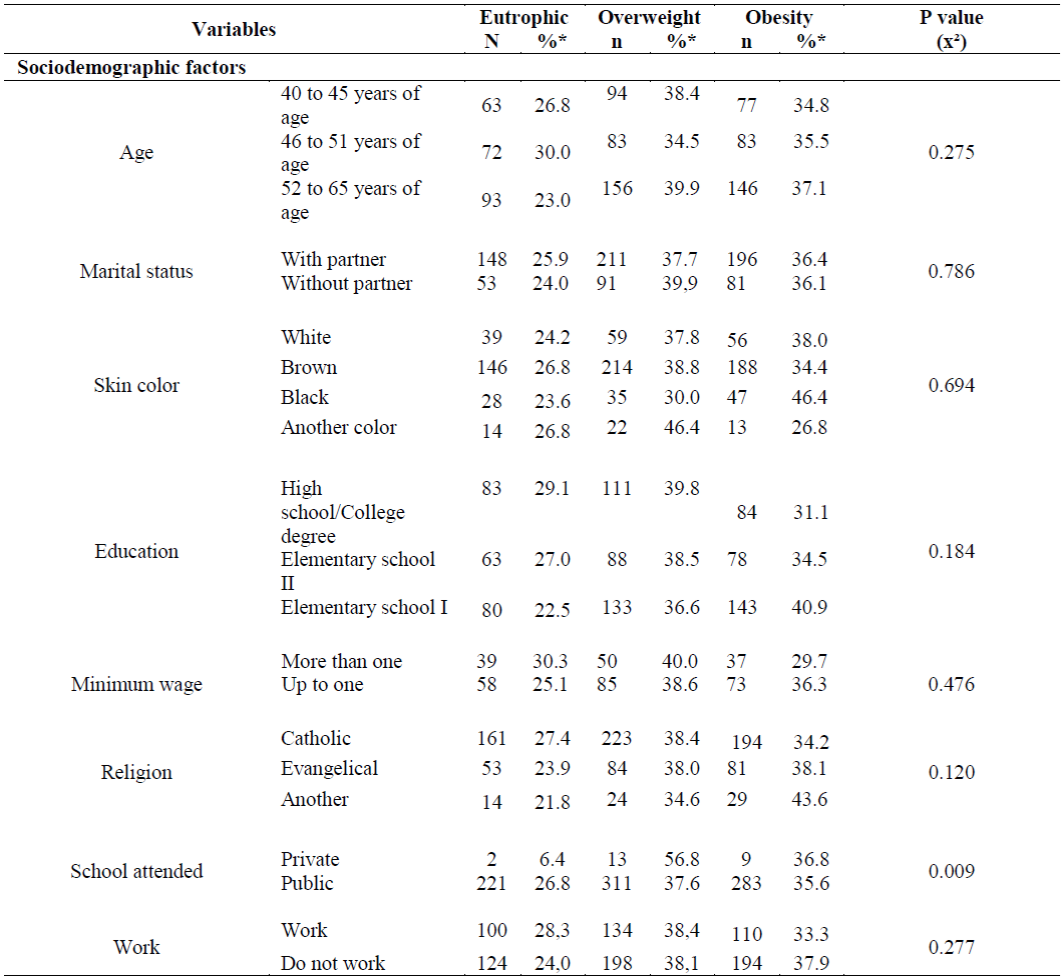
*: Corrected by the drawing effect (deff); (x²): Qui-Square test; p value: Significance level p <0.05.
Table 5 shows the significant association between the BMI change variables such as smoking (p = 0.023) and treatment for weight loss (p = 0.000). Among the non-smokers (74.7%) and those who received treatment for weight loss, (86.5%) had higher rates of overweight and obesity.
As for anthropometric factors, there were significant associations (p = 0.000), with BMI change. Women who presented altered AC (83.0%) and WHR (80.5%) had higher rates of overweight and obesity (Table 5).
Table 5 Association of BMI levels among lifestyle, eating habits and anthropometric measures.
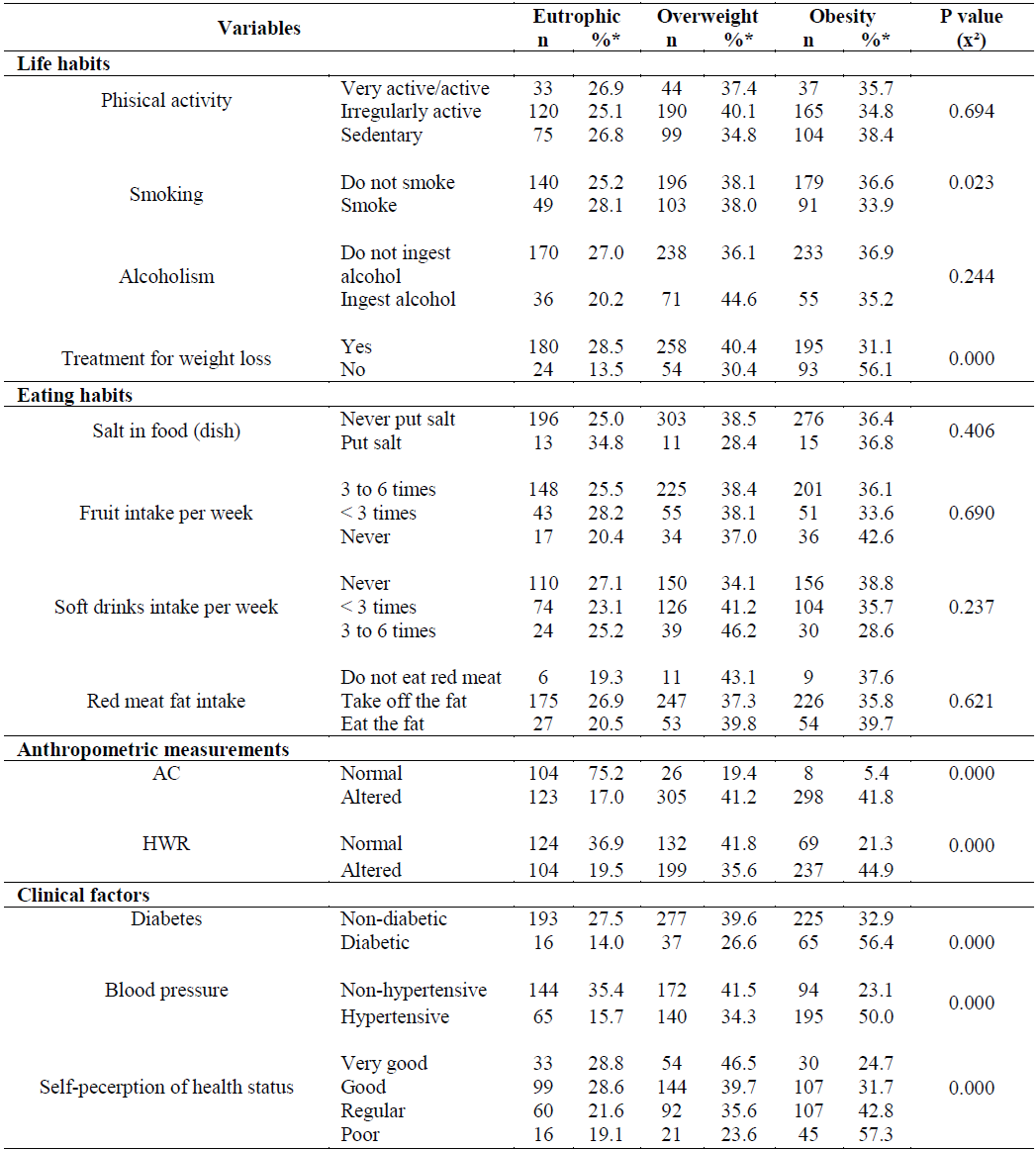
*: Corrected by the drawing effect (deff); AC: Abdominal circumference; HWR: Hip-waist ratio; (x²): Qui-Square test; p value: Significance level p <0.05.
Significant associations were also observed with the presence of diabetes (p = 0.000), high blood pressure (p = 0.000), self-perception of poor health status (p = 0.000), and prevalence of overweight and obesity (Table 5).
DISCUSSION
Due to the alterations that the female organism undergoes during this period, the association between obesity and climacteric has been object of study of several authors15),(16. Being overweight is a serious health problem, since it represents an important risk factor for the development of cardiovascular diseases, systemic arterial hypertension, respiratory problems, diabetes mellitus, dyslipidemias and neoplasias, with a significant impact on the mortality of affected individuals17),(18. It also increases significantly in women after they reach 40 years of age. It has reached 65% of them between 40 and 59 years of age and 73.8% in women over 60 years of age 54.
When associated sociodemographic factors with BMI, considering the type of school attended by the women, those attending private schools were more predisposed to the development of overweight and obesity. A study carried out by Rosaneli et al19) stated that school is a suitable place for healthy activities, including adequate food and educational and physical activities. These are decisive factors to prevent the occurrence of diseases. However, considering the rise of chronic diseases such as obesity in students of private schools, more studies focused on socioeconomic variables should be performed to clarify this association.19.
Regarding cigarette smoking, those surveyed women with overweight and obesity were not smokers, information that is in agreement with the study by Soares and Barreto20. They highlighted smoking as a protective action for overweight and abdominal obesity, as tobacco competes with brain reward sites for food, leading to reduced appetite. In addition, nicotine raises lipid oxidation levels, contributing to a more significant catalytic state and lower weight gain.
In this study, the results showed significant associations between BMI changes and treatment for weight loss. That confirms the findngs of Leão et al21. They highlighted in their work the fact that most individuals seeking treatment for weight loss do not do so with the necessary motivation. In addition to this, there is evidence that weight loss depends on the change of the permanent lifestyle, requiring a multiprofessional and continuous approach in order to be successful.22.
The changes in waist circumference and waist-hip ratio were more evident in climacteric women who presented high BMI. This suggests that central obesity may be due to climacteric hormonal variations, leading to android obesity, accumulation of fat in the abdomen, and decreased fat in the hips and thighs (gynoid fat)2.
Diabetes mellitus and systemic arterial hypertension were associated with high BMI indexes in the studied women. This fact meets Al-Safi and Polotsky23. They point out that over the last decades the prevalence of obesity has increased in epidemic proportions, along with several comorbidities such as hypertension and diabetes mellitus type two, due to the increase in life expectancy, changes in lifestyle and eating habits20.
It is also emphasized that BMI was associated with self-perception of health, evidencing that overweight and obese women presented poor perception of their health status. This fact was already demonstrated in a previous study conducted with Brazilian women over 50 years of age24. These findings also compare with data obtained by Lui Filho et al25 in their study about climacteric, which observed that the climacteric symptoms, associated with obesity, bring negative repercussions to mood and negative self-perception of individual health.
Duarte et al26 emphasize the importance of a more frequent monitoring of the health area of climacteric women, seeking to estimate the presence of obesity and associated factors. Such information contributes to the planning of health actions, programs and policies aimed at the promotion, prevention and diagnosis of these diseases, impacting on the reduction of the mortality of this population group.
The present study points out, by means of a probabilistic, stratified and representative sample of the climacteric population assisted in primary care, factors associated with overweight. However, it presents as main limitation the study design, of the transversal type, measuring the outcome and the exposure simultaneously and not proving temporality.
CONCLUSION
The present study identified a high prevalence of overweight and obesity among the climacteric women assisted by primary care, as well as associations between the Body Mass Index and the type of school attended, smoking, treatment for weight loss, anthropometric measures, and factors, such as diabetes, blood pressure and self-perception of health status. These findings point to the need for strategies for obesity control to be planned and implemented, especially among climacteric women.
The Family Health Strategy should be more incisive in the search for prevention and reduction in the number of obesity cases among climacteric women, since this action will have a positive impact on changes in the morbidity and mortality profile of this population group.
REFERENCIAS
1. Ventura DA, Fonseca VM, Ramos EG, Marinheiro LP, Souza RA, Chaves CR, et al. Association between quality of the diet and cardiometabolic risk factors in postmenopausal women. Nutrition Journal. 2014; 13(1): 121. [ Links ]
2. Fortes CK, Berlezi EM, Winkelmann ER, Franz LBB. Estudo populacional de identificação de fenótipo de risco cardiovascular em mulheres no período do climatério. In: Anais do XXII Seminário de Iniciação Científica, 2014, Ijuí, RS. Editora: Universidade Regional do Noroeste do Estado do Rio Grande do Sul. 2014. p. 1-7. [ Links ]
3. Blümel JE et al. Obesidade e sua relação com sintomas depressivos e sedentarismo em mulheres de meia-idade. Maturitas. 2015; (80)1: 100-105. [ Links ]
4. Moore LL, Bradlee ML, Singer MR, Splansky GL, Proctor MH, Ellison RC et al. BMI and waist circumference as predictors of lifetime colon cancer risk in Framingham Study adults. International Journal of Obesity and Related Metabolic Disorders. 2004; 28(4): 559-567. [ Links ]
5. Andrade FT, Martins MCC, Santos MAP, Torres-Leal FL, Ferreira AHC. Estimativa do percentual de gordura utilizando o IMC. Revista Brasileira de Obesidade, Nutrição e Emagrecimento. 2014; 8(47): 142-147. [ Links ]
6. Steiner ML, Azevedo LH, Bonacordi CL, Barros AZ, Strufaldi R, Fernandes CE. Avaliação de consumo alimentar, medidas antropométricas e tempo de menopausa de mulheres na pós-menopausa. Rev Bras Ginecol Obstet. 2015; 37(1):16-23. [ Links ]
7. Assunção WAC, Prado WL, Oliveira LMFT, Falcão APST, Costa MC, Guimarães FJSP. Comportamento da gordura abdominal em mulheres com avanço da idade. Rev. Educ. Fis. UEM. 2013; 24(2): 287-294. [ Links ]
8. Bak-Sosnowska M, Skrzypulec-Plinta V. Przyczyny nadmiernej masy ciala u kobiet w okresie menopauzalnym. Prz Menopauzalny. 2012; 11: 31-35. [ Links ]
9. Pasquala KK, Carvalhaes MABL, Paradac CMGL. Atenção à saúde da mulher após os 50 anos: vulnerabilidade programática na Estratégia Saúde da Família. Revista Gaúcha de Enfermagem. 2015; 36(2): 21-27. [ Links ]
10. Organizácion Mundial De La Salud. Investigaciones sobre la menopausia em los años noventa. Genebra: Organizácion Mundial de La Salud; 1996. (Serie de Informes Técnicos 866). [ Links ]
11. Szwarcwald CL, Damacena GN. Amostras complexas em inquéritos populacionais: planejamento e implicações na análise estatística dos dados. Revista Brasileira de Epidemiologia. 2008; 11(1): 38-45. [ Links ]
12. World Health Organization (WHO). Obesity: preventing and managing the global epidemic (report of a WHO consultation on obesity). Genebra: World Health Organization; 1998. [ Links ]
13. The Third Report of the National Cholesterol Education Program (NCEP). Expert Panel on Detection. Evaluation, and treatment of high blood cholesterol in adults (Adult Treatment Panel III). JAMA. 2001;16;285(19):2486-97. [ Links ]
14. Molarius A, Seidell JC, Sans S, Tuomilehto J, Kuulasmaa K. Waist and hip circumferences, and waist-hip ratio in 19 populations of the WHO MONICA project. International Journal of Obesity. 1999; 23(2): 116-125. [ Links ]
15. Lizcano F, Guzmán G. Estrogen deficiency and the origin of obesity during menopause. Bio Med Res Int. 2014; 2014:757461. [ Links ]
16. Gravena AA, Brischiliari SC, Lopes TC, Agnolo CM, Carvalho MD, Pelloso SM. Excess weight and abdominal obesity in postmenopausal Brazilian women: a population-based study. BMC Womens Health. 2013;13:46. [ Links ]
17. Reis CEG, Vasconselos IAL, Oliveira OMV. Panorama do estado antropométrico dos escolares brasileiros. Revista Paulista de Pediatria. 2011; 29(1): 108-16. [ Links ]
18. Instituto Brasileiro de Geografia e Estatística (BR), Pesquisa de Orçamentos Familiares: antropometria e estado nutricional de crianças, adolescentes e adultos do Brasil. Brasília (DF); 2010. [ Links ]
19. Rosaneli CF, Baena CP, Auler F, Nakashima ATA, Netto-Oliveira ER, Oliveira AB, Guarita-Souza LC, Olandoski M, Faria-Neto JR. Aumento da Pressão Arterial e Obesidade na Infância: Uma Avaliação Transversal de 4.609 Escolares. Arq Bras Cardiol. 2014; [online].ahead print, PP.0-0. [ Links ]
20. Soares DA, Barreto SM. Sobrepeso e obesidade abdominal em adultos quilombolas, Bahia, Brasil. Caderno de Saúde Pública. 2014; 30(2): 341-354. [ Links ]
21. Leão JM, Lisboa LCV, Pereira MAP, Lima LF, Lacerda KC, Elias MAR, et al. Estágios motivacionais para mudança de comportamento em indivíduos que iniciam tratamento para perda de peso. Jornal Brasileiro de Psiquiatria. 2015; 64(2): 107-14. [ Links ]
22. Viana LV, Paula TP, Leitão CB, Azevedo MJ. Fatores determinantes de perda de peso em adultos submetidos a intervenções dietoterápicas. Arq Bras Endocrinol Metab. 2013; 57(9): 717-21. [ Links ]
23. Al-Safi ZA, Polotsky AJ. Obesity and menopause. Best Pract Res Clin Obstet Gynaecol. 2014; 29(4): 548-53. [ Links ]
24. Machado VSS, Valadares ALR, Costa-Paiva LH, Osis MJ, Sousa MH, Pinto-Neto AM. Factors associated with the self-perception of health among Brazilian women 50 years or older; a population-based study. Menopause. 2013; 20(10):1055-1060. [ Links ]
25. Lui Filho JF, Baccaro LFC, Fernandes T, Conde DL, Costa-Paiva L, Pinto Neto AM. Epidemiologia da menopausa e dos sintomas climatéricos em mulheres de uma região metropolitana no sudeste do Brasil: inquérito populacional domiciliar. Revista Brasileira de Ginecologia e Obstetrícia. 2015; 37(4): 152-8. [ Links ]
26. Duarte MR, Reis VMCP, Rocha JSB, Passos BMA. Anthropometric Parameters, Blood Pressure and Climacteric Phases of Diabetic and Non-Diabetic Women in the City of Montes Claros- Minas Gerais, Brazil. International Journal of Humanities Social Sciences and Education (IJHSSE). 2015; 2(8): 57-63. [ Links ]
Received: October 14, 2016; Accepted: January 22, 2017
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
