










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.18 no.54 Murcia abr. 2019 Epub 14-Oct-2019
https://dx.doi.org/10.6018/eglobal.18.2.322041
Originals
Risk factors for anxiety and depression in the preoperative period of cardiac surgery
1Nurse. Master in Nursing. Nursing Assistant of the Hospital das Clínicas of the Federal University of Pernambuco. Recife, PE, Brazil
2Nurse. Resident in Cardiovascular Nursing of Agamenom Magalhães Hospital. Recife, PE, Brazil.
3Nurse. Resident in Surgical Nursing of Getúlio Vargas Hospital. Recife, PE, Brazil
4Nurse. Post-Doctorate in Fundamental Nursing. Professor of the Associate Program of Nursing Graduate Program at the University of Pernambuco / State University of Paraíba. Recife, PE, Brazil.
Objective
To evaluate the risk factors of anxiety and depression in the preoperative period of cardiac surgery.
Method
This is a sectional study, conducted between January and June 2017, in a university hospital of reference in cardiology in northeastern Brazil. A total of 174 patients were evaluated using their own questionnaire and the Hospital Anxiety and Depression Scale (HADS) and Odds Ratios were calculated to assess the risk.
Results
In the assessment of anxiety, significant risk factors were: female gender, years of study, absence of companion, previous experience of cardiac surgery and cancellation of surgery during hospitalization. As for depression, risk factors were revealed: female sex and hospitalization time greater than 15 days.
Conclusion
The nurse has instruments available to recognize anxiety and depression, including nursing diagnoses and validated scales, as well as having a preponderant role in these cases. It should be an institutional challenge to streamline the service in order to avoid prolongation of hospitalization and cancellations of surgery for structural reasons.
Key words: Anxiety; Depression; Cardiac Surgery; Perioperative period; Nursing
INTRODUCTION
The preoperative period is considered the stage in which the individual becomes more vulnerable for their needs, particularly the psychological needs, becoming more prone to an emotional imbalance, anguish, fear, often translating into anxiety and depression1 2.
The preoperative period represents not only the possibility of cure but also the failure(1)(3). Cardiac surgery has the peculiarity of involving the organ popularly recognized as the noblest and directly related to the maintenance of life3. The unknown along with the possibility of failure aggravate the anguish that patients have to face and, consequently, they have anxiety and depression1 3. Despite the benefits brought to the patient, the surgery also generates pain in many aspects, from the pain and the risks that exposes the patient to his/her daily life, the uncertainties and limitations involved4.
Initially, cardiac surgery for patients may represent a magical intervention to rid them of the risk of heart attack and death, the pain and discomfort that heart disease has forced them to live with5. However, anxiety, depression, stress, fear, and other negative feelings and emotions are found that require the patient to develop coping and adaptation strategies5 6.
Cardiac surgery has been linked to high rates of preoperative anxiety. The hospitalization for cardiological reasons, even non-surgical ones has already great repercussion in the levels of anxiety. In the preoperative period of general surgery, the presence of anxiety and depression measured by the Hospital Anxiety and Depression Scale (HADS) was estimated in 44.3% and 26.6%, respectively7. In the preoperative study of myocardial revascularization surgery, the presence of anxiety and depression investigated with the same scale occurred in 34.4% and 28.1%, respectively, reinforcing the importance of using this scale in the early detection of these symptoms8.
Although there is evidence that cardiac surgery is a major stressor with repercussions on significant levels of preoperative anxiety and depression, it is extremely important to understand the factors worsening or alleviating the condition and the intrinsic or extrinsic resources to patients that nurses can use in their interventions4.
The nurse should develop care that includes the risk factors, but it is necessary to know the intervening factors. Besides the sense of seeking to understand these gaps in the therapeutic relationship between professional and patient, more research should be carried out with the aim of providing evidence for comprehensive care. With the incorporation of new evidences and the result of well-delineated researches, the assistance protocols can be reformulated considering dimensions neglected until then in health care.
This study aimed to evaluate the risk factors of anxiety and depression in the preoperative period of cardiac surgery.
METHOD
This is a cross-sectional, observational study with a quantitative approach performed in the coronary arteries, cardiomyopathies and valvular heart diseases at a university hospital of reference in Northeastern Brazil, between January and April 2017.
A calculation for the delimitation of the sample was performed using the equation to calculate the sample size for means, considering that the variable-outcome is quantitative continuous. For this calculation, an error α of 5% was used, which corresponds to the difference between the value estimated by the research and the true value; and a 95% confidence level was used, which is the probability that the effective sampling error is smaller than the sampling error allowed by the research. The standard deviation adopted with a reference was found in an international study using the same scale with 142 patients evaluating anxiety and depression two days before they underwent cardiac surgery. The value of the standard deviation found in the study was 8.729. The maximum error was 1.5 points in the mean. Considering the finite population of 200 patients submitted to cardiac surgery on average and for a period of five months of collection, the sample was estimated in 130 patients. There was a goal to collect, but 30% more patients were collected (169) considering the possible losses. Thus, in the end, a total of 174 patients were collected.
Based on the weekly surgical schedule released on Fridays by the surgical team, visits to the wards were scheduled from Monday to investigate the patients who were eligible for the survey and who were aware by the surgical indication team. All patients had been informed of the surgical indication and the expected date of the surgery by the team. Patients hospitalized in the preoperative period of cardiac surgery for myocardial revascularization, valve replacement or valvuloplasty with written agreement were included and those with aortic disease or congenital heart disease, lowered level of consciousness, impaired verbal communication or any clinical or psychological condition that interfere with the interview or make them uncomforTable, previous use of anti-depressant, prior medical diagnosis of mood, anxiety, or other psychiatric disorders and refusal at any stage of the interview were excluded of the study
The data were collected by the researchers using a specific instrument containing: a questionnaire created for a socio-demographic survey, such as gender, age, origin, income, education level, type of surgery, hospitalization time, among others and the Hospital Anxiety and Depression Scale.
The Hospital Anxiety and Depression Scale (HADS) is composed of 14 questions, seven of them to evaluate anxiety and seven to evaluate depression, with each item scored on a scale of 0 to 3, with a total of 21 points for each scale. The cutoff point of adopted is without anxiety or depression from 0 to 8, with anxiety or depression >9 on each sub-scale, respectively7,8. This scale has been used for its quick and simple use (in up to ten minutes), since its validity and reliability has been demonstrated in several studies and because it does not contain somatic symptom assessment8).
The primary data were stored using spreadsheets of the Microsoft Excel 2013 software. Data were analyzed using descriptive and inferential statistics using the Statistical Package for the Social Sciences - SPSS 20.0 software. The Kolmogorov-Smirnov Normality test showed that the evaluated outcomes had no normal distribution (<p = 0.05). The Odds Ratio was calculated to assess the risk of anxiety and depression among dichotomized groups by the variables collected, which are presented with the 95% confidence interval and p-value, considering the level of statistical significance of the test for p <0.05. The internal consistency of the scales items was evaluated by Cronbach's alpha. The reliability of the application in the sample was considered high for both the subscale Anxiety (Cronbach's alpha = 0.815) and Depression (Cronbach's alpha = 0.845), indicating its good representation of the desired information.
The patients were evaluated in the afternoon, before the visit time of the relatives, considering that the routine visits of the nursing and medical teams are performed in the morning. Data collection took place in two main phases. In the first stage, the study participants were informed about the procedures and objectives of the research and invited to participate by signing the Informed Consent Form (ICF). In the second stage, the interviews were carried out and the collection instrument was applied.
The interviews were conducted at the bedside, with the consent of the nurse responsible for the sector and the companions who were instructed not to intervene in any answer if they stayed with the patients. Patients were approached and invited to participate in the research, agreeing in writing after they were informed about the objectives, risk, and benefits involved. The research was elaborated according to the precepts of Resolution CNS nº436/12, approved by the Research Ethics Committee of the institution (Opinion nº 1,915,220/CAAE: 30622414.7.0000.5192).
RESULTS
There were 50.6% of men and 49.4% of women. Most patients (54.6%) were married, Catholic (55.2%), and from the interior (49.1%), married or with companion (54.6%). The mean age was 59.16 ± 13.86 years old, and 55.7% were over 60 years old. Most of the sample was reported without work (66.7%), with only one-third of them active in the labor market (33.3%). The average income observed between them was 1.31 ± 0.96 minimum wages in force in the period (R$ 880.0), and 70.7% declared receiving up to 1 minimum wage.
Only a little more than a fifth of the sample (22.5%) has already undergone previous cardiac surgery. In 34.5% of cases, surgery was canceled and the mean number of cancellations observed was 0.57 ± 0.98 (Table 1).
On average, the patients were hospitalized for 22.06 ± 11.08 days, with 70.7% more than 15 days; the mean preoperative period was 20.95 ± 29.78 with 56.9% of the patients within 15 days and 43.1% with a period of more than 15 days, according toTable 2. Most of the patients had a companion (85.6%) and religious visit (65.5%), but a daily visit was not observed so frequently (25.3%). In only 6.9% of cases, there was a request for a religious visit.
Table 1. Preoperative surgery and hospitalization data. Recife, Pernambuco, Brazil, 2017.

*Md±dp: mean±standard deviation
The mean value found for anxiety was 5.68 ± 4.79, lower than the cut-off point (8 points), which classified the patients as anxious, and only 27.6% of the patients fit into this classification. For the subscale depression, the values are even better, with a mean score of 3.99 ± 4.40, with only 17.8% of depressive patients.
There was no significant association between socio-demographic characteristics and anxiety in the preoperative period. Only in the gender issue, women were 3.46 times more anxious than men (p <0.01), and higher education (OR: 0.477, CI 0.247-0.962, p = 0.037) (Table 2).
Table 2. Risk factors for anxiety related to socio-demographic characteristics in the preoperative period of cardiac surgery. Recife, Pernambuco, Brazil, 2017.
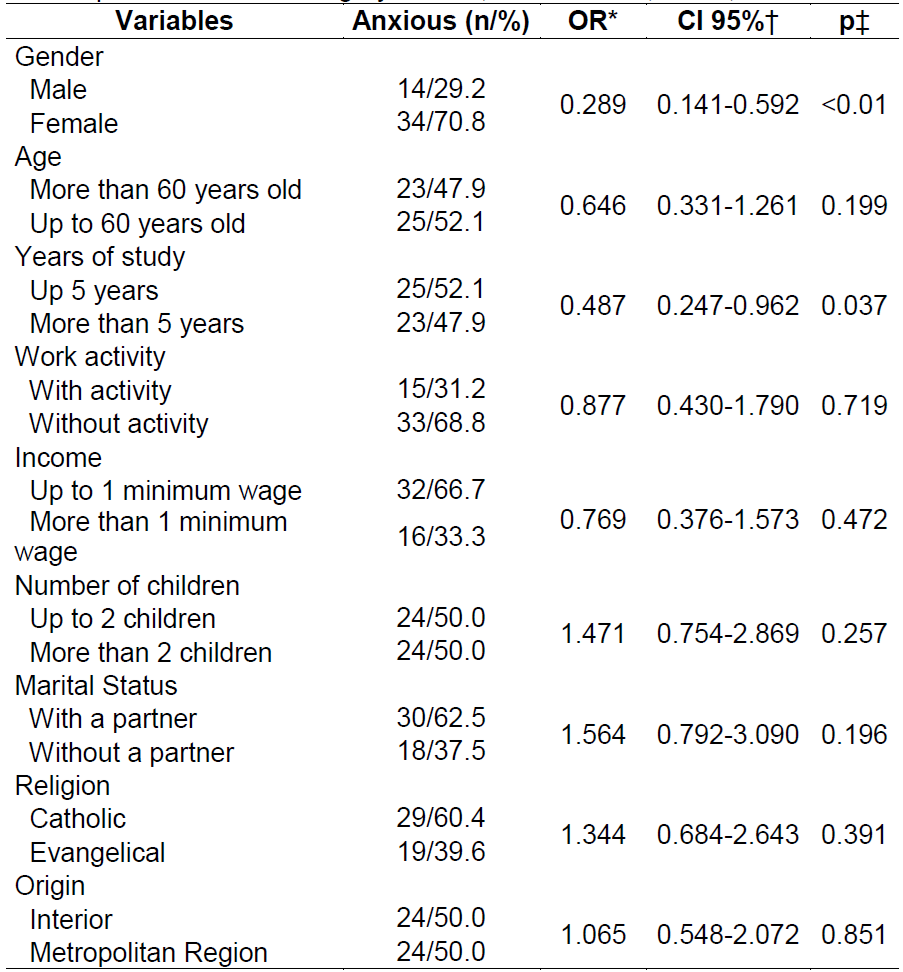
*odds ratio† confidence interval (95%) ‡ Chi-square test
Analyzing the data related to surgery and hospitalization as risk factors for anxiety, in a statistically significant way, the cancellation of surgery increases by 1.96 times the risk of anxiety and the absence of companions increased in 2.37 times (Table 3).
Table 3. Risk factors for anxiety related to surgery and hospitalization in the preoperative period of cardiac surgery. Recife, Pernambuco, Brazil, 2017.

*odds ratio† confidence interval (95%) ‡ Chi-square test
Table 4shows that, regarding the depression, the risk was approximately three times higher in women (p = 0.008). The other socio-demographic aspects were not statistically significant as risk factors or protection for the presence of depression (Table 4).
Table 4. Risk factors for depression related to socio-demographic characteristics in the preoperative period of cardiac surgery. Recife, Pernambuco, Brazil, 2017.
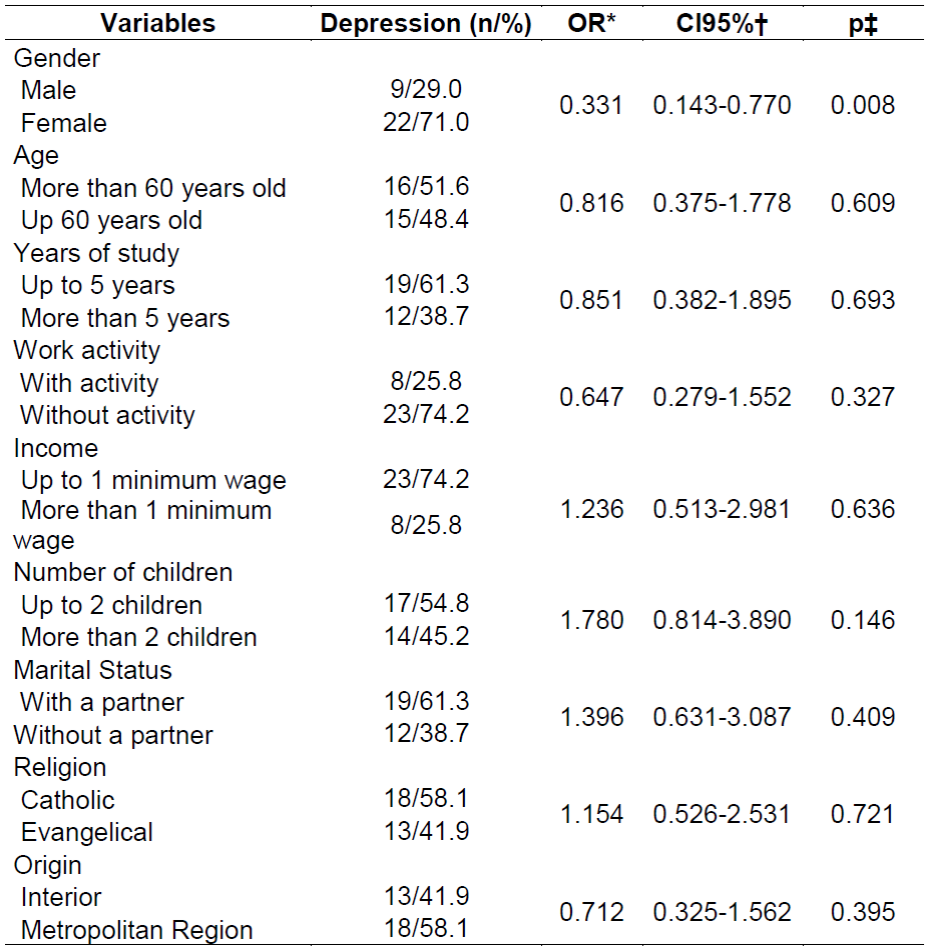
*odds ratio† confidence interval (95%) ‡ Chi-square test
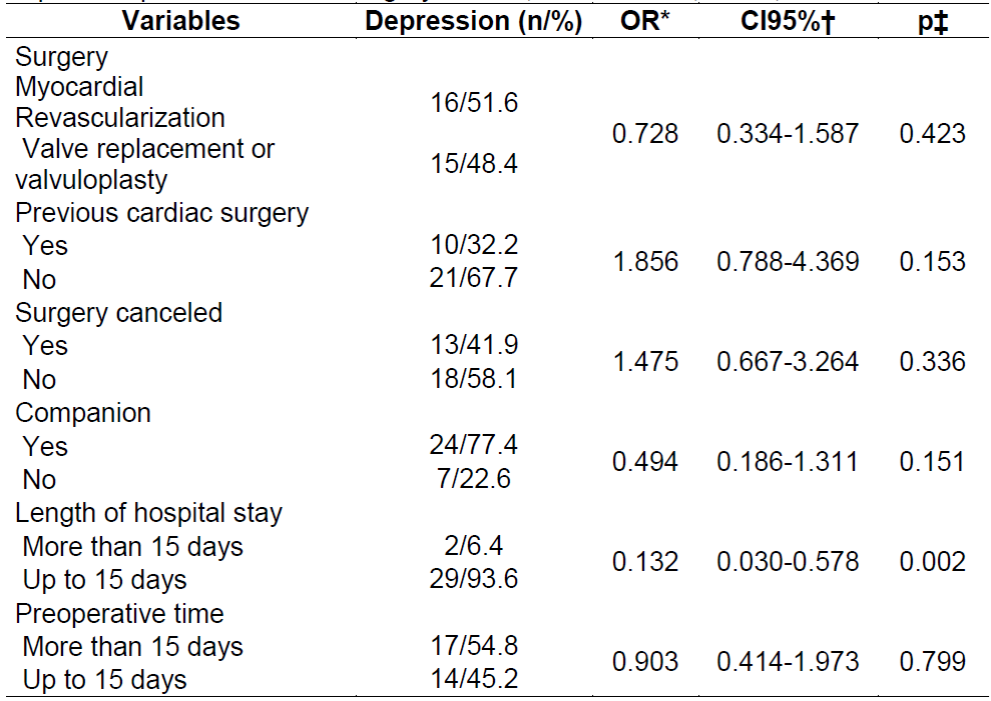
There was no difference between the surgery and the hospitalization data to influence the risk of depression among those patients evaluated. The hospitalization time greater than 15 days increased by 7.6 times the risk of depression (p = 0.002) (Table 5).
DISCUSSION
Other studies with similar samples found approximate frequencies of anxiety and depression(8)(9)(10)(11)(12)(13)(14). A review on the topic showed that the prevalence for anxiety and depression reach 41.5% and 28.3%, respectively4.
Other references revealed that these symptoms are relevant in the preoperative period and may last a week after surgery, and may interfere in the recovery and adaptation of patients to the new reality11 14 15. The association of anxiety with postoperative mortality was have increased the risk in up to five times12. There are references that these preoperative mood disorders reflect in a higher incidence of postoperative anxiety and depression, and resulting in greater long-term mortality11 15 16. Also in the postoperative repercussion, another follow-up with 1071 patients showed that preoperative anxiety, which lasts after surgery, is a predictor of postoperative chest pain for two years(17).
A recent Spanish study obtained averages of anxiety and depression very close to those found with a sample of preoperative cardiac surgery patients of the same size (n = 100), measured on the same scale13. The research showed that the age under 65 years old would be a risk factor for preoperative anxiety. However, in the sample presented here, there was no significant difference according to their age13. This publication did not find differences between genders, whereas our findings revealed female gender as a risk factor for anxiety and depression13, while in our sample women were 3.46 times more anxious than men, and according toTables 2andTable 4their risk of women was approximately three times more than men (p <0.01, p = 0.008). Consistent with the results presented, this study pointed out that the increase in hospital stay is associated with higher depression scores and preoperative anxiety is related to increased postoperative pain, although it does not show relationships with other outcomes such as mechanical ventilation, intensive care unit stay, and death13.
Another study showed a weak association between preoperative state anxiety in cardiac surgery and age (r = 0.226, p <0.001), higher values in women, negative correlation with education level (p <0.001), and higher scores in patients with companions than without companion (single, widowed and divorced)(18). The female gender was statistically significantly associated with higher scores of depression in a study of patients with heart disease after percutaneous intervention19.
Table 3shows that education level over 5 years was a protective factor (OR: 0.487, CI: 0.247-0.962; p = 0.037) for anxiety. An international cohort study showed that patients with preoperative anxiety traits and lower levels of formal education had higher long-term mortality, followed by 10 years, as EUROSCORE, which assesses the risk of cardiac surgery through clinical variables20.
The presence of a companion was shown as a protective factor for both anxiety and depression, and the absence of companions increased the risk of anxiety by 2.37 times, according toTable 3. A national study compared the variation of anxiety in a control group in the preoperative period, a group with a trained nurse and a group that received visits from relatives and found that the presence of family members in the period was responsible for the greater reduction of the scores21.
On average, the patients were hospitalized for 22.06 ± 11.08 days, with 70.7% more than 15 days; the mean preoperative period was 20.95 ± 29.78 with 56.9% of the patients within 15 days and 43.1% with a period of more than 15 days.
The hospitalization time greater than 15 days increased by 7.6 times the risk of depression (p = 0.002), according toTable 5. The increase in depressive symptoms has also been evidenced in other studies12 20 22. Despite evaluating a small sample and not considering depression, one study showed that the short waiting time for surgery (approximately 6 days) may also be related to fear and anxiety23).
Although there was no other reference in the cardiac surgery that confronted the results of the present study, the relevance of a situation that occurs commonly in the public health system should be highlighted: the cancellation of the surgery. Patients who had this experience had almost double the risk (OR = 1.96, p <0.05). Surgeries can be canceled due to clinical situations such as unwanted infections to be treated previously or structural reasons, including lack of blood reserve, specific material or not for surgery.
Studies of a qualitative approach reveal that for patients, the ideation of the disease is associated with a limiting situation and that delay in performing surgery may result in greater complications or even death3 22. Feelings related to the preoperative period of cardiac surgery involve waiting anxiety, fear of surgery and future expectation after surgery, religiosity, and introspection22. Surgery can also be understood in its empowering aspects of individuals reorganizing their lives and their relationships22.
Also in the qualitative approach, a research investigating the strategies that patients use to deal not only with anxiety and depression before a cardiac surgery but with all the psycho-emotional repercussions of the event for the individual, acknowledged that this confrontation is based in the presence and support of the family, in the quality of interfamily relationships, in the use of spiritual resources and in the participation of a rehabilitation program that, in addition to physical conditioning, it enables social interaction24. Other references found that spirituality was the main support for facing heart surgery and the presence of belief in God is considered as an important factor for this confrontation3 25. Preoperative anxiety in another sample had a significant and negative association with hope and a positive response to avoidance and anger behavior and negative religious coping26.
Finally, a national study concluded that despite being considered a major stressor and having a great impact on the patients' lives, cardiac surgery had a fundamental role in improving quality of life, depression, and anxiety in all evaluated aspects, corroborating with the positive value of the surgery besides the clinical aspect27.
Nurses should be aware of anxiety and depression in the preoperative period, including nursing diagnoses and interventions in the systematization of the care provided, and should also consider the possible relation with the knowledge deficit of the disease or the procedure1 3.
A recent systematic review showed that preoperative education offered or coordinated by nurses has an effect on preoperative anxiety and on improving physical or psychological recovery, and the relationship with pain reduction and hospital stay should be further explored since the analysis of the studies was not conclusive in these aspects28.
The failure to establish therapeutic relationships with the professionals leads to a lack of guidance regarding the surgery and lack of support by the health team, causing the patients to stay in an anxious and depressed state throughout the hospitalization. However, the presence of information on surgery contributes to the reduction of anxiety levels29.
The present study was limited because although the findings were confronted with the literature and they were found in other studies, they reflect the reality of only one service. In other hospital environments and other interdisciplinary preoperative care routines, the results may be different. Also, the relationships with quality of life with personality trait anxiety and with previous cardiovascular symptoms were not considered, since the literature has shown that such factors have a major influence on anxiety before the cardiac surgery, nor were predictive risk for surgery, such as EuroSCORE.
FINAL CONSIDERATIONS
The main risk factors for anxiety and depression found should be given special attention to women, unaccompanied patients, those who have undergone previous surgeries, those who spend more time in hospital and with their surgery schedule canceled.
Two factors that can be considered modifiable are highlighted: length of hospital stay and cancellation of surgery. It is a challenge to improve the service to avoid long hospitalization and cancellations of surgery for structural reasons. Identifying the cause of cancellations for these patients and the reason for the delay in performing the surgery should be the theme of further research and health professionals and managers should prevent such events.
The institutions that attend the patient in the perioperative period of cardiac surgery should favor and encourage strategies of preventive action of the mood disorders, in particular in the moments that precede the surgery.
The nurse has instruments available to recognize anxiety and depression, including nursing diagnoses and validated scales, as well as having a preponderant role in acting in these cases. The nurse should be articulated with the multi-professional team to elaborate the best approach for the patient.
REFERENCIAS
1. Gomes ET, Melo RLAS, Vasconcelos EMR, Alencar EM. Use of nursing diagnoses anxiety and fear in the medical and surgical clinics of a university hospital. R pesq cuid fundam online [Internet]. 2012 [Acesso 10 dezembro 2017]; 4(2):2419-26. Disponível em: http://www.seer.unirio.br/index.php/cuidadofundamental/article/view/1779 doi: 10.9789/2175-5361.2012.v4i2.2419-2426 [ Links ]
2. Costa VASF, Silva SCR, Lima VCP. The pre-surgery anxiety of the patient: the alliance between the nurse and psychologist. Rev SBPH [Internet]. 2010 [Acesso 10 dezembro 2017]; 13(2): 282-98. Disponível em: http://pepsic.bvsalud.org/pdf/rsbph/v13n2/v13n2a10.pdf [ Links ]
3. Camponogara S, Soares SGA, Silveira M, Viero CM, Barros CS, Cielo C. Percepção de pacientes sobre o período pré-operatório de cirurgia cardíaca. Rev Min Enferm [Internet]. 2012 [Acesso 10 dezembro 2017]; 16(3):382-390. Disponível em: http://www.reme.org.br/artigo/detalhes/541 doi: S1415-27622012000300010 [ Links ]
4. Gomes ET, Bezerra SMMS. Ansiedade e depressão no período pré-operatório de cirurgia cardíaca. Rev RENE [Internet]. 2017 [Acesso 10 dezembro 2017]; 18:420-427. Disponível em: http://www.periodicos.ufc.br/rene/article/viewFile/20078/30728 doi: 10.15253/2175-6783.2017000300019 [ Links ]
5. Quintana JF, Kalil RAK. Cirurgia cardíaca: manifestações psicológicas do paciente no pré e pós-operatório. Psicol hosp [Internet]. 2012 [Acesso 10 dezembro 2017]; 10(2):17-32. Disponível em: http://pepsic.bvsalud.org/pdf/ph/v10n2/v10n2a03.pdf [ Links ]
6. Ai AL, Wink P, Shearer M. Fatigue of survivors following cardiac surgery: positive influences of preoperative prayer coping. Br j health psychol [Internet]. 2012 [Acesso 10 dezembro 2017]; 17(4):724-42. Disponível em: https://www.ncbi.nlm.nih.gov/pubmed/22524258 doi: 10.1111/j.2044-8287.2012.02068.x. [ Links ]
7. Marcolino JAM, Mathias LAST, Piccinini Filho L, Guaratini AA, Suzuki FM, Alli LAC. Hospital Anxiety and Depression Scale: a study on the validation of the criteria and reability on preoperative patients. Rev bras anestesiol [Internet]. 2007 [Acesso 10 dezembro 2017]; 57(1): 52-62. Disponível em: https://www.ncbi.nlm.nih.gov/pubmed/19468618 doi: 10.1590/S0034-70942007000100006 [ Links ]
8. Carneiro AF, Mathias LAST, Rassi Júnior A, Morais NS, Gozzani JL, Miranda AP. Evaluation of preoperative anxiety and depression in patients undergoing invasive cardiac procedures. Rev bras anestiol [Internet]. 2009 [Acesso 10 dezembro 2017]; 59(4):431-8. Disponível em: http://www.scielo.br/pdf/rba/v59n4/05.pdf doi: 10.1590/S0034-70942009000400005 [ Links ]
9. Krannich JHA, Weyers P, Lueger S, Herzog M, Bohrer T, Elert O. Presence of depression and anxiety before and after coronary artery bypass graft surgery and their relationship to age. BMC Psychiatry [Internet]. 2007 [Acesso 10 dezembro 2017]; 7:47. Disponível em: https://www.ncbi.nlm.nih.gov/pubmed/17850655 doi: 10.1186/1471-244X-7-47 [ Links ]
10. Ramesh C, Nayak BS, Pai VB, George A, George LS, Devi ES. Pre-operative anxiety in patients undergoing coronary artery bypass graft surgery - a cross-sectional study. Intern J afri nurs sci [Internet]. 2017 [Acesso 10 dezembro 2017]; 7:31-36. Disponível em: https://www.sciencedirect.com/science/article/pii/S2214139116300476 doi: 10.1016/j.ijans.2017.06.003 [ Links ]
11. Patron E, Messerotti BS, Palomba D. Preoperative and perioperative predictors of reactive and persistent depression after cardiac surgery: a three-month follow-up study. Psychosomatics [Internet]. 2014 [Acesso 10 dezembro 2017]; 55(3):261-71. Disponível em: https://www.ncbi.nlm.nih.gov/pubmed/24673940 doi: 10.1016/j.psym.2013.12.011. [ Links ]
12. Williams JB, Alexander KP, Morin JF, Langlois Y, Noiseux N, Perrault LP, et al. Preoperative anxiety as a predictor of mortality and major morbidity in patients aged >70 years undergoing cardiac surgery. Am j cardiol [Internet]. 2013 [Acesso 10 dezembro 2017];111(1):137-42. Disponível em: https://www.ncbi.nlm.nih.gov/pubmed/23245838 doi: 10.1016/j.amjcard.2012.08.060 [ Links ]
13. Navarro-García MA, Marín-Fernández B, Carlos-Alegre V, Martínez-Oroz A, Martorell-Gurucharri A, Ordoñez-Ortigosa E et al. Preoperative mood disorders in patients undergoing cardiac surgery: risk factors and postoperative morbidity in the intensive care unit. Rev esp cardiol [Internet]. 2011 [Acesso 10 dezembro 2017]; 64(11):1005-10. Disponível em: https://www.ncbi.nlm.nih.gov/pubmed/21924811 doi: 10.1016/j.recesp.2011.06.009 [ Links ]
14. Gallagher R, McKinley S. Anxiety, depression and perceived control in patients having coronary artery bypass grafts. J adv nurs [Internet]. 2009 [Acesso 10 dezembro 2017]; 65: 2386-2396. Disponível em: https://www.ncbi.nlm.nih.gov/pubmed/19747294 doi: 10.1111/j.1365-2648.2009.05101 [ Links ]
15. Tully PJ, Pedersen SS, Winefield HR, Baker RA, Turnbull DA, Denollet J. Cardiac morbidity risk and depression and anxiety: a disorder, symptom and trait analysis among cardiac surgery patients. Psychol health med [Internet]. 2011 [Acesso 10 dezembro 2017]; 16(3):333-45. Disponível em: https://www.ncbi.nlm.nih.gov/pubmed/21491341 doi: 10.1080/13548506.2011.553960 [ Links ]
16. Pourafkari N, Pourafkari L, Nader D. Depression following coronary artery bypass grafting surgery revisited. Turk kardiyol dern ars [Internet]. 2016 [Acesso 10 dezembro 2017];4(6):524-29. Disponível em: https://www.ncbi.nlm.nih.gov/pubmed/27665338 doi: 10.5543/tkda.2016.49697 [ Links ]
17. Pagé MG, Watt-Watson J, Chomiere M. Do depression and anxiety profiles over time predict persistent post-surgical pain? A study in cardiac surgery patients. Eur j pain [Internet]. 2017 [Acesso 10 dezembro 2017]; 21(6):965-76. Disponível em: https://www.ncbi.nlm.nih.gov/pubmed/28185371 doi: 10.1002/ejp.998. [ Links ]
18. Fathi M, Alavi SM, Joudi M, Joudi M, Mahdikhani H, Ferasatkish R et al. Preoperative anxiety in candidates for heart surgery. Iran J Psychiatry behav sci [Internet]. 2014 [Acesso 10 dezembro 2017]; 8(2):90-6. Disponível em: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4105610/ [ Links ]
19. Furuya RK, Costa ECA, Coelho M, Richter VC, Dessotte CAM, Schmidt A et al. Anxiety and depression among men and women who underwent percutaneous coronary intervention. Rev esc enferm USP [Internet]. 2013 [Acesso 10 dezembro 2017]; 47(6):1333-7. Disponível em: https://www.ncbi.nlm.nih.gov/pubmed/24626358 doi: 10.1590/S0080-623420130000600012. [ Links ]
20. Cserép Z, Losoncz E, Balog P, Szili-Török T, Husz A, Juhász B et al. The impact of preoperative anxiety and education level on long-term mortality after cardiac surgery. J cardiothorac surg [Internet]. 2012 v;(14):7:86. Disponível em: https://www.ncbi.nlm.nih.gov/pubmed/22973828 doi: 10.1186/1749-8090-7-86. [ Links ]
21. Assis CC, Lopes JL, Nogueira-Martins LA, Barros ALBL. Embracement and anxiety symptoms in patients before cardiac surgery. Rev bras enferm [Internet]. 2014 [Acesso 10 dezembro 2017];67(3): 401-407. Disponível em: http://www.scielo.br/pdf/reben/v67n3/0034-7167-reben-67-03-0401.pdf. doi: 10.5935/0034-7167.20140053 [ Links ]
22. Wottrich SH, Quintana AM, Camargo VP, Quadros COP, Naujorks AA. Significados e vivências mediante a indicação cirúrgica para pacientes cardíacos. Psicol estud [Internet]. 2013 [Acesso 10 dezembro 2017];18(4), 609-619. Disponível em: http://www.scielo.br/pdf/pe/v18n4/04.pdf doi: 10.1590/S1413-73722013000400004 [ Links ]
23. Feuchtinger J, Burbaum C, Heilmann C, Imbery C, Siepe M, Stotz U et al. Anxiety and fear in patients with short waiting times before coronary artery bypass surgery - a qualitative study. J clin nurs [Internet]. 2014 [Acesso 10 dezembro 2017]; 23(13-14):1900-7. Disponível em: https://www.ncbi.nlm.nih.gov/pubmed/24372741 doi: 10.1111/jocn.12467. [ Links ]
24. Koerich C, Baggio MA, Erdmann AL, Lanzoni GMM, Higashi GDC. Myocardial revascularization: strategies for coping with the disease and the surgical process. Acta paul enferm [Internet]. 2013 [Acesso 10 dezembro 2017]; 26(1):8-13. Disponível em: http://www.scielo.br/pdf/ape/v26n1/03.pdf. doi: 10.1590/S0103-21002013000100003 [ Links ]
25. Gomes ET, Espinha DCM, Bezerra SMMS. Religiosidade e crença em Deus no pré-operatório de cirurgia cardíaca. Online braz j nur [Internet]. 2015 [Acesso 10 dezembro 2017]; 14(3): 273-83. Disponível em: http://www.objnursing.uff.br/index.php/nursing/article/view/5138. doi: 10.17665/1676-4285.20155138 [ Links ]
26. Ai AL, Noel T. Postoperative Biomarkers and Psychiatric Symptoms one-month following open-heart surgery. Biolog psychiatry psychopharm [Internet]. 2013;15(1). [ Links ]
27. Dal Boni AL, Martinez JE, Saccomann IC. Quality of Life of patients undergoing coronary artery bypass grafting. Acta paul enferm [Internet]. 2013 [Acesso 10 dezembro 2017]; 26(6):575-80. Disponível em: http://www.scielo.br/pdf/ape/v26n6/11.pdf doi: 10.1590/S0103-21002013000600011 [ Links ]
28. Guo P. Preoperative education interventions to reduce anxiety and improve recovery among cardiac surgery patients: a review of randomised controlled trials. J clin nurs [Internet]. 2015 [Acesso 10 dezembro 2017]; 24(1-2):34-46. Disponível em: https://www.ncbi.nlm.nih.gov/pubmed/24894181 doi: 10.1111/jocn.12618. [ Links ]
29. Silva MEM, Zakir NS. Instructional control and relaxation procedure as psychological preparation for pre-surgery patients with heart disease. Estud psicol [Internet]. 2015 [Acesso 10 dezembro 2017]; 28(3):371-379. Disponível em: http://www.scielo.br/pdf/estpsi/v28n3/a09v28n3.pdf doi: 10.1590/S0103-166X2011000300009 [ Links ]
Received: February 18, 2018; Accepted: June 02, 2018
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
