










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.19 no.58 Murcia abr. 2020 Epub 18-Mayo-2020
https://dx.doi.org/eglobal.373931
Originals
Clinical judgment in nursing diagnoses of chronic kidney patients on hemodialysis
1Nurse. Doctoral Student of the Graduate Nursing Program (PPGENF) from the Federal University of Ceará. Specialist in Nephrology Nursing. Fortaleza, Ceará, Brazil.
2Nurse. Master Student of the Graduate Nursing Program (PPGENF) from the Federal University of Ceará. Scholarship Student from the Coordination for the Improvement of Higher Education Personnel (Capes). Fortaleza, Ceará, Brazil.
3ENurse. Doctoral Student of the Graduate Nursing Program (PPGENF) from the Federal University of Ceará. Assistant Teacher of the Undergraduate Nursing Course from the Federal University of Amapá. Fortaleza, Ceará, Brazil.
4Nurse. Teacher of the Graduate Health and Nursing Clinical Care Program (PPCCLIS). Tenured Teacher of the Undergraduate Nursing Course from the State University of Ceará. Fortaleza, Ceará, Brazil.
5Nurse. Teacher of the Graduate Nursing Program (PPGENF) and Doctor in Nursing. Tenured Teacher of the Nursing Department from the Federal University of Ceará. Fortaleza, Ceará, Brazil.
Method
quantitative study performed with 25 patients undergoing dialysis therapy in a tertiary hospital through the accomplishment of semi-structured interviews, physical examination and analysis of laboratory test results. In order to analyze the diagnostic inferences, we used the clinical reasoning of Alfaro-LeFevre and then applied the Outcome-Present State Test Model.
Results
We inferred 12 nursing diagnoses found in 70% of the sample, where anxiety was the priority diagnosis. In order to minimize changes in the health of the patient, the interventions chosen were: teaching: procedure/treatment; exercise promotion; progressive muscle relaxation; distraction/inattention; emotional support; nutrition control; and improved socialization.
Conclusion
the clinical reasoning technique used by this model can contribute to the agility and execution of the nursing process.
Keywords: Renal Dialysis; Nursing; Nursing Process; Nursing Diagnosis; Health Priorities
INTRODUCTION
Chronic kidney disease is a disease that goes along silently, slowly and progressively, requiring the accomplishment of a kidney replacement therapy when it reaches the most advanced stage 1. In Brazil, according to the latest census performed by the Brazilian Society of Nephrology, there are an estimated 122,825 patients on dialysis treatment, 92.1% of whom on hemodialysis modality (HD) and 92.3% of these are supported by the Unified Health System 2.
It is known that HD is a highly complex procedure and requires nurses to have skills in the identification of possible complications that may affect the patient, in order to establish plans with specific, safe, effective and quality interventions. In this context, it is essential to use the nursing process (NP), defined as the way of thinking and teaching appropriate to the nursing profession, mainly in the identification of impaired, ineffective and maintaining basic human nursing responses that can be expressed in nursing diagnostic concepts (ND), which, based on their constituent elements (related factors, clinical conditions and risk populations) provide the foundations for the selection of interventions and the achievement of results that promote the welfare of patients 3.
The identification of priority ND enables and contributes to the planning of results and interventions can be more effective and based on solvability. This identification requires clinical reasoning to anchor the understanding of behavior standards and the relationships among the nursing care needs of patients 4.
Accordingly, clinical reasoning is defined as a complex cognitive process that uses formal and informal thinking strategies to collect and analyze patient information, evaluate the meaning of this information, and weigh alternative actions. This process is dynamic, expansive and recursive, as information 3.
Among the strategies for the establishment of clinical reasoning, based on the elucidation of priority ND, it raises the Outcome-Present State Test Model (OPT), designed by Pesut and Herdman5. It addresses the detection of standards and recognition of relationships among a large number of diagnoses and represents a network of clinical reasoning with the design of the lines that favors a reflection on how the diagnoses relate to each other. It is a tool that helps nurses to understand behavioral standards and relationships among all the nursing care needs that one patient may have.
Accordingly, the clinical reasoning network is a graphical representation that depicts the reflection on relationships, since, while a line is drawn, it explains how and why a diagnosis is connected or influenced by others. It clearly shows that one of the nursing diagnoses acquires greater importance or has greater influence in terms of interaction with other problems. This diagnosis that has the greatest influence becomes the priority and, therefore, deserves more attention 6-7.
It is necessary to highlight that the Brazilian scientific diffusion regarding the OPT Model is still poor. However, we believe in the relevance of this study so that other nurses know this model and use it in their clinical care work process. In this sense, this study aims to analyze the current state outcome in chronic kidney patients on hemodialysis, establishing interventions and results from the Nursing Interventions Classification 8(NIC) and Nursing Outcomes Classification 9(NOC), respectively.
MATERIAL AND METHOD
This is an analytical and quantitative study, developed in a tertiary hospital of Fortaleza - Ceará, which is reference for chronic kidney patients, from December 2015 to January 2016.
In order to develop this research, we included all the chronic kidney patients who underwent HD, totaling 25 patients. Inclusion criteria were: being 18 years old or older and presenting hemodynamic stability to dialysis during the data collection period. Exclusion criteria were: impaired cognitive capacity and impaired auditory and visual acuity, measured by Mini Mental, propaedeutic auditory tests (tuning fork test, Weber and Rinne), Snellen test, respectively.
In order to identify the problems, changes and difficulties that the disease produces in each patient, we used semi-structured interviews designed by the researchers to hold this study, based on a script directed to the physical examination of the patient and to the search for laboratory test results in the medical records.
Data collection took place at different times by two nephrology nurses working longer than five years in replacement therapy services considering the following steps (data collection, data validation, data grouping, standard identification, communication and data registration), as established in the Alfaro-LeFevre 4framework for nursing research. These nurses prepared the diagnostic inferences considering the Outcome-Present State Test Model (OPT) diagnostic reasoning model structured in the following phases: reflection, perception, logical clues, tests, decision-making processes and judgment 3 5.
Subsequently, they formed a consensus group with another nurse with extensive experience in the use of nursing taxonomies in clinical practice, teaching and management with the purpose of solving possible discordant doubts or inferences between the two members. Thus, in order to denominate the groups, we used the ND standardized by the 2018-2020 NANDA-I Taxonomy Inc 3based on the defining characteristics, risk factors and related factors. In order to compose the OPT Model, we extracted the ND present in 70% of the sample.
In the operationalization of this study, the following steps were followed: location of the underlying disease, aggravation or other problem issue; positioning of the disease at the center of the graphic representation; fitting of nursing diagnoses around the disease; reflection and connection from all those involved, explaining why diagnoses are connected and how they influence each other; identification of a priority diagnosis and questioning about the effect, if care is focused on solving the priority diagnosis and what effect it would have on other diagnoses 10. Once the priority diagnosis was framed, nursing interventions and outcomes were determined from the standardized NIC 8and NOC 9taxonomies considering the respective diagnosis.
The development of this study complied with the ethical and legal aspects of Resolution 466/12 of the National Health Council and obtained a favorable opinion by the Ethics and Research Committee of the State University of Ceará with Opinion nº 392.488.
RESULTS
In order to accomplish the OPT Model, we chose the most prevalent ND. From this perspective, 12 ND were chosen from the total (Table 1).
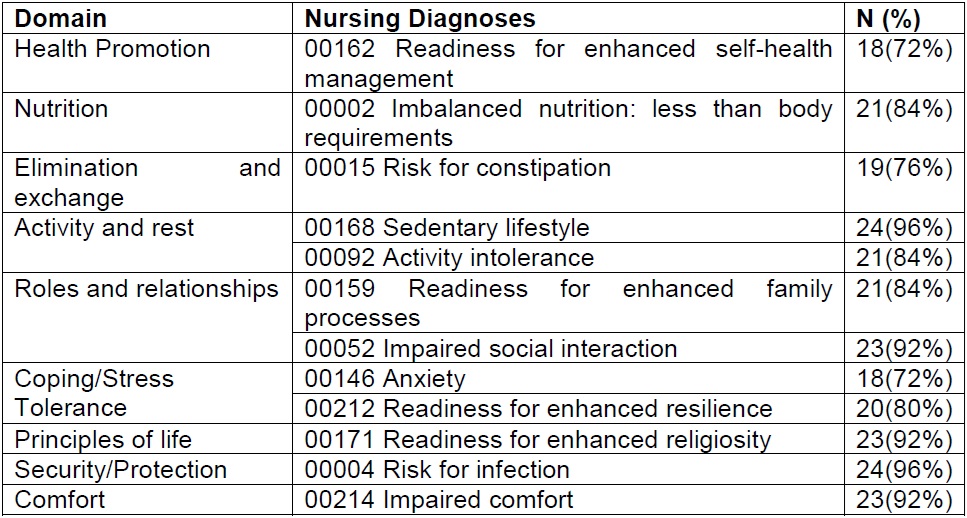
The clinical reasoning used by this analysis model is performed on the basis of problem-solving techniques, where we chose problem-focused diagnoses and risk diagnoses. Thus, only eight ND were included in the study: risk for infection, anxiety, impaired social interaction, activity intolerance, sedentary lifestyle, risk for constipation, imbalanced nutrition and impaired comfort. Figure 1shows this distribution.

establishing the most prevalent ND, we noted their relationship with the comorbidities inherent in the health-disease process. Among them, we should highlight the risk for infection due to the fact that chronic kidney patients are subjected to invasive procedures, such as the passage of a double lumen catheter and the puncture of a fistula or due to uremia that causes the impaired immune system to respond later than the system of a person considered healthy. This diagnosis has a cause relationship with impaired comfort and sedentary lifestyle, besides an effect relationship with imbalanced nutrition lower than body requirements.
The ND on anxiety was shown due to the changes that the aggressive treatment and the pathology bring to the life of the patient. It has a cause and effect relationship with the ND on risk for constipation, impaired comfort, imbalanced nutrition lower than body requirements, sedentary lifestyle and activity intolerance. These relationships were identified in patients from concerns due to changes in life events, decreased productivity, increased tension, anguish, disquiet and fatigue.
Another ND is the impaired social interaction, which emerges as a secondary problem due to physical limitations and treatment routine, which sometimes prevents the development of outside activities. This ND has a cause and effect relationship with anxiety and sedentary lifestyle, and only an effect relationship with activity intolerance and impaired comfort.
As for activity intolerance, it corresponds to uremia and excessive fluid accumulation, which causes dyspnea. This ND has a cause relationship with sedentary lifestyle, risk for constipation and impaired social interaction, and a cause and effect relationship with impaired comfort.
Sedentary lifestyle was another ND identified in the study, justified by the exhaustive routine of HD sessions, in addition to insufficient interest and motivation for physical activities. This ND has a cause association with risk for constipation, a cause and effect relationship with impaired social interaction and anxiety, besides an effect relationship with physical activity intolerance, risk for infection and impaired comfort.
The ND on risk for constipation due to water restriction was identified to avoid excessive weight gain, change in dietary habits, daily physical activity less than recommended, among other factors. There are cause relationships with impaired comfort, a cause and effect relationship with anxiety, besides an effect relationship with imbalanced nutrition, sedentary lifestyle and activity intolerance.
Another ND investigated was imbalanced nutrition lower than body requirements. There is an association with the clinical condition of the patient, which sometimes entails loss of appetite, and with the diet restriction offered before and after hemodialysis treatment. Therefore, it has a cause relationship with the ND on risk for constipation and risk for infection, besides a cause and effect relationship with anxiety.
The ND on impaired comfort was also identified due to the duration of each hemodialysis session. In order to better conduct the treatment, the patient is practically motionless so that its blood flow is sufficient and constant. This ND also relates to the use of uncomforTable armchairs and to the sensation of chilliness. Thus, this diagnosis entails a cause relationship with sedentary lifestyle and impaired social interaction, a cause and effect relationship with anxiety and activity intolerance, besides an effect relationship with risk for infection and risk for constipation. Figure 2shows the relationships established among ND.

When establishing the links among the diagnoses, we found that anxiety had more influence on other problems; therefore, it is classified as a priority ND.
From this perspective, we defined the expected result and the interventions/ activities for the ND on anxiety, which were relevant to the chronic kidney patient on HD (Table 2).
Table 2. Results10and interventions9for the ND on anxiety present in chronic kidney patients on hemodialysis. Fortaleza, CE, Brazil, 2016
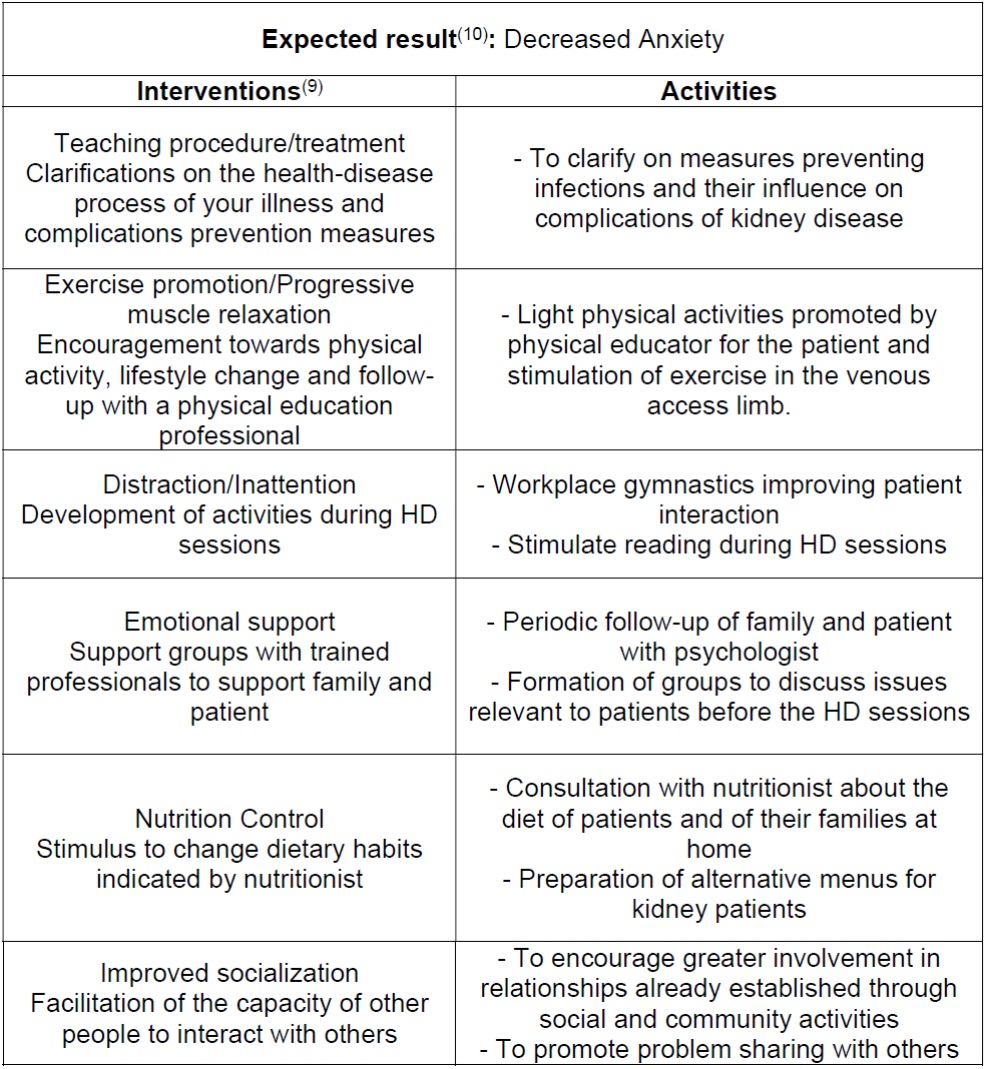
In order to properly perform NP, the nursing staff should implement interventions and activities with the support of a multidisciplinary team in a collaborative and interdependent way, in order to develop health education actions, such as support groups and activities during nursing sessions of HD.
DISCUSSION
Hemodialysis treatment causes changes in the life of the chronic kidney patient that undermines, besides the physical aspect, the psychological one, with personal, family and social impacts. For this reason, it requires intensive and immediate nursing interventions to deal with the limitations caused by the disease, in order to ensure a better quality of life.
In this study, anxiety stands out as a priority ND that has the greatest influence on other diagnoses. This result corroborates another study that associates anxiety with the onset of almost all pathologies. In the case of kidney disease, anxiety emerges from two strong factors: the chronicity of the disease and the arduous treatment of HD. Anxiety emerges from both the effective loss and from the possibilities of loss 11.
It is important to highlight the physical and mental adaptation to treatment, such as prescriptions, restrictions and diets, which make the patient alert and tense, thereby triggering anxiety reactions due to constant exposure to stressful situations, such as dialysis and frequent permanence in a hospital environment 11.
Although anxiety is prevalent in chronic kidney patients, as it is perceived as life threatening because it impairs the identity of the patient, its authority, and brings uncertainty about the future. In this sense, a clinical trial with musical intervention was effective in relation to anxiety and vital parameters of chronic kidney patients and proved to be a therapeutic resource that could be used in nursing care 12.
Another study determines that the relationship between prevalence of anxiety and quality of life is inversely proportional. This condition may represent an increased mortality and morbidity in hemodialysis patients, as well as undermining treatment adherence and modulating their immune and nutritional status, both due to anxiety and associated symptoms, such as loss of concentration, loss of motivation, sleep disorders, fatigue, depressed mood and difficulty in understanding information 13.
It is a task of the nursing staff to provide, during hemodialysis sections, a quiet, comforTable and pleasant environment so that the patient can feel welcomed and safe during the HD sessions 14, as these patients often remain motionless, since blood flow needs to be sufficient and constant.
In light of the foregoing, we should emphasize the need for a periodic evaluation of anxiety-causing agents and their effects on the health and quality of life of patients, in order to qualify the care for which nurses are responsible 15. Moreover, with the support of a multidisciplinary team, we can enable the development of strategies that offer interventions aimed at improving the welfare of patients 11.
During this study, we perceived that anxiety is poorly investigated in patients with chronic kidney disease, with a larger number of studies focusing on depressive episodes. Thus, few studies on the prevalence of anxiety disorders in hemodialysis patients are available 16.
Accordingly, it is crucial to recognize that the use of this clinical and educational tool for professional learners promotes the visibility of nursing as a social and humanistic discipline impregnated by health care practice. It is notorious that the model employed is a device that can elucidate or generate innumerable mid-range theories and practical theories by producing specific knowledge involving teaching and research, underpinning the best practice choices so that they are sensitive to the uniqueness of each individual and to the context of life and general welfare of this person, thereby orienting in the choice of clinical priorities 17.
Given the results now found, we found that, during the process of articulating human responses in chronic kidney patients, it is possible to transfer knowledge to professional practice, since it favors the development of strong intellectual skills, as well as technical-scientific, ethical, esthetic and humanistic skills 18.
Considering the clinical reasoning network of nursing diagnoses with the establishment of the main diagnosis, we observed that, besides investigating, diagnosing, setting goals and intervening based on evidence, the holistic perspective is somewhat evident when listing nursing diagnoses from different domains of the Taxonomy NANDA-I Inc., traversing physiological responses and achieving responses that are characterized as behavioral and social, thereby producing tangible results that are able to improve the coping response to stress inferred in the study on Anxiety, as well as the interventions.
Accordingly, developing critical thinking and holistic clinical reasoning is to apply strong critical thinking, based on a set of consistent and accurate clinical data underpinned by solid knowledge capable of elucidating these data 19. Moreover, in order produce an accurate diagnosis, it is essential to consider the relevant factors for decision-making processes and problem-solving techniques when establishing nursing interventions 19.
Thus, when establishing the OPT Model, nephrology nurses and nursing students make a reflective judgment on what to believe or what to do in the context analyzed; as well as to develop clinical decision trees that foster the rupture of diagnostic chains, thereby increasing the knowledge of the causality of the elements of professional practice.
CONCLUSION
The experience with the clinical reasoning of the OPT Model provided an expanded view of the relationships among nursing diagnoses, enabling the identification of a priority diagnosis. Accordingly, we can observe the importance that this model represents by allowing a holistic and efficient approach, thereby contributing to the development of the nursing process and to the quality of the care actions provided.
We can verify that studies of this type are crucial to stimulate the teaching of critical thinking, clinical reasoning, diagnostic and therapeutic decision-making processes, allowing nursing students to start thinking as nurses, based on the identification of the basic human responses hindering the health care-disease process.
With regard to clinical practice, we can envisage that this study may help nephrologists or health care nurses to ground their critical and clinical gaze on the identification and articulation of related factors that are linked to the priority nursing diagnoses found in chronic kidney patients on hemodialysis or other contexts of care, ensuring the elaboration and discernment among the results to be expected and the interventions prescribed to be implemented.
Regarding the contribution to nursing science, this study has shown strong signals and evidence for causal theories, whether biological, psychological or social, in individuals who experience chronic kidney disease and undergo dialysis therapy, thereby consolidating innumerable theoretical models or nursing theories.
This study had as its limitations the sample size, which is not allowed to generalize the data obtained, since there were no random samples. In addition, we can mention restraining factors like type of sampling, selection of a single hemodialysis service, as well as the absence of comparative studies using the OPT model in chronic kidney patients on hemodialysis.
REFERENCIAS
1. Dhima X, Jaku G, Zefaj D, Ioannis K, Chrysoula V, Margitsa S, et al. Needs of hemodialysis patients and factors affecting them. Glob J Health Sci. 2016;8(6):109-20. doi: http://dx.doi.org/10.5539/gjhs.v8n6p109 [ Links ]
2. Sociedade Brasileira de Nefrologia. Relatório Censo 2018. 2018. Disponível em: https://sbn.org.br/categoria/censo-2018/ [ Links ]
3. Herdman TH, Kamitsuru S. Diagnósticos de enfermagem da NANDA: definições e classificação 2018-2020. Porto Alegre: Artmed; 2018. [ Links ]
4. Alfaro-LeFevre R. Critical thinking, clinical reasoning, and clinical judgment: a practical approach. 6ª ed. Elsevier; 2017. [ Links ]
5. Pesut DJ, Herman J. Clinical Reasoning: The art e science of critical & creative thinking. Columbia: Delmar Publishers; 1999. [ Links ]
6. Sevilla JCR. Papel de enfermería en el juicio clínico: la valoración y el diagnóstico. Enferm Cardiol. 2014;(61):25-31. Disponível em: https://www.enfermeriaencardiologia.com/wp-content/uploads/62_02.pdf [ Links ]
7. Gonzáles-Castillo MG, Monroy-Rojas A. Proceso enfermero de tercera generación. Enfermería Universitaria. 2016;13(2):124-129. doi:http://dx.doi.org/10.1016/j.reu.2016.03.003 [ Links ]
8. Bulechek GM, Butcher HK, Dochterman JM. Classificação das intervenções de enfermagem - NIC. 6ª ed. Rio de Janeiro: Elsevier; 2016. [ Links ]
9. Moorhead S, Johnson M, Maas ML, Swanson E. Classificação dos Resultados de Enfermagem (NOC). 5ª ed. Elsevier; 2016. [ Links ]
10. Espinosa C. El modelo AREA es la evolución del PAE que se centra en los resultados. Asociación Española de Nomenclatura, Taxonomía y Diagnósticos de Enfermería. 2011;1-9. [ Links ]
11. Rajan EJE, Subramanian S. The effect of depression and anxiety on the performance status of end-stage renal disease patients undergoing hemodialysis. Saudi J Kidney Dis Transpl. 2016;27(2):331-34. Available from: http://www.sjkdt.org/text.asp?2016/27/2/331/178555 [ Links ]
12. Melo, GAA, Rodrigues, AB, Firmeza, MA, Grangeiro, AS, Oliveira, PP, Caetano, JA. Musical intervention on anxiety and vital parameters of chronic renal patients: a randomized clinical trial. Rev Latino-Am Enfermagem. 2018;26:e2978. doi: http://dx.doi.org/10.1590/1518-8345.2123.2978 [ Links ]
13. Vasilopoulou C, Bourtsi E, Giaple S, Koutelekos I, Theofilou P, Polikandrioti M. The impact of anxiety and depression on the quality of life of hemodialysis patients. Glob J Health Sci. 2016;8(1):45-55. doi: http://dx.doi.org/10.5539/gjhs.v8n1p45 [ Links ]
14. Frazão CMFQ, Delgado MF, Araújo MGA, Silva FBBL, Sá JD, Lira ALBC. Cuidados de enfermagem ao paciente renal crônico em hemodiálise. Rev Rene. 2014;15(4):701-9. Available from: http://www.repositorio.ufc.br/bitstream/riufc/10441/1/2014_art_albclira.pdf [ Links ]
15. Ottaviani AC, Betoni LC, Paravini SCI, Say KG, Zazzetta MS, Orlandi FS. Association between anxiety and depression and quality of life of chronic renal patients on hemodialysis. Texto Contexto Enferm. 2016; 25(3):e00650015. doi: http://dx.doi.org/10.1590/0104-07072016000650015 [ Links ]
16. Dias DR, Shiozawa P, Miorin LA, Cordeiro Q. Prevalência de sintomas depressivos e ansiosos em pacientes com doença renal crônica em programa de hemodiálise: um estudo transversal. Arq Med Hosp Fac Cienc Med Santa Casa. 2015; 60:65-71. Available from: http://www.fcmscsp.edu.br/images/Arquivos_medicos/2015/04-AO83.pdf [ Links ]
17. Facione PA, Crossetti MGO, Riegel F. Pensamento Crítico Holístico no Processo Diagnóstico de Enfermagem. Rev Gaúcha Enferm. 2017;38(3):e75576. doi: http://dx.doi.org/10.1590/1983-1447.2017.03.75576 [ Links ]
18. Riegel F, Crossetti MGO. Theoretical frameworks and instruments for evaluation of critical thinking in nursing and education. Rev Gaúcha Enferm. 2018;39:e2017-0097. doi: https://doi.org/10.1590/1983-1447.2018.2017-0097 [ Links ]
19. Ceolin S, González JS, Ruiz MCS, Heck RM. Theoretical bases of critical thinking in ibero-american nursing: integrative literature review. Texto Contexto Enferm. 2017;26(4):e3830016. doi: http://dx.doi.org/10.1590/0104-07072017003830016 [ Links ]
Received: April 30, 2019; Accepted: August 09, 2019
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
