










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkEnfermería Global
versión On-line ISSN 1695-6141
Enferm. glob. vol.21 no.65 Murcia ene. 2022 Epub 28-Mar-2022
https://dx.doi.org/10.6018/eglobal.477281
Originals
Indices of social and programmatic vulnerability for older adults living at home
1 Universidad de Brasília - Campus Darcy Ribeiro.Brasília, DF, Brasil. alissonobolina@unb.br
2 Escuela de Enfermería de Ribeirão Preto, Universidad de São Paulo. Ribeirão Preto, SP, Brasil.
3 Universidad Federal do Triângulo Mineiro. Uberaba, MG, Brasil.
Objectives:
Build Social and Programmatic Vulnerability indices for older people living at home and verify the association of vulnerability components (individual, social and programmatic).
Methods:
It is a population based study, household and transversal survey type, conducted with 701 community older adults. Descriptive and bivariate exploratory spatial analysis was conducted (p≤ 0.05) as well as analysis of Main Components.
Results:
By means of the indices, it was observed that peripheral census tracts presented very high social vulnerability levels and that the main variables representative of the programmatic component - access to dentist via SUS, medications, and search of the same care location. It was verified that only 3.9% of the older adults did not present some level of vulnerability (individual, social and programmatic).
Conclusion:
Older adults are exposed to multiple vulnerability conditions, and Social and Programmatic Vulnerability indices are important tools for managers’ decision making.
Keywords: Older adults; Frail older adults; Vulnerable populations; Basic health indicators; Nursing
INTRODUCTION
The word vulnerability is used to denote the older adults’ susceptibilities to health problems and damages, increasing mortality1. However, some experts in the field understand that vulnerability in older adults is “more than the impact of physical, emotional and mental damages, it is the result of the social construction and historical context”2 (our translation).
In order to deal with the vulnerability concept adopted for this study3 , individual vulnerability was considered as bio-physiological risk for the development of aggravations to the health4; social vulnerability as adverse environmental and social conditions that determine situations of risk to health5; and programmatic vulnerability concerns the access and use of health resources by older adults3.
Under such definitions, the ageing process increases biological vulnerability to adverse events4,6. It is also known that unfavorable social conditions and restrict access to health services can worsen this condition7. Despite the multidimensional conception of vulnerability, a growing corpus of geriatric and gerontology studies has focused on associating physical frailty to adverse health conditions8.
The most accepted frailty conception in Brazil and worldwide is commonly related in terms of individual bio-physiological vulnerability, which includes higher individual susceptibility to the development of adverse health outcomes6. However, the experts in the area have increasingly acknowledged the importance of considering the conception from an integrated perspective8.
Though there is inter-relation among the concepts, vulnerability goes beyond biological aspects, because it also includes social and contextual matters to which older adults are exposed over the course of ageing2. Therefore, the underlying idea to vulnerability concept requires not simply to account the individual for his/her health condition, but rather to incorporate collective and social plans3.
Considering that the programmatic assessment is one of the components of the vulnerability concept adopted, it was not found in the scientific literature instrument to assess this component. So, a Programmatic Vulnerability index was developed in the present study associated to older adults access and use of health services. It is worth mentioning that indices are variables that provide a picture of the object of assessment in order to assist in health managers’ decision making9.
With regard to older adults, the national literature brings signs of social inequality and inequality of access to health resources by them10. Since they present more need of health care, due to the ageing process7, dimensioning the programmatic component of vulnerability can provide subsidies for the conception of strategies to improve the assistance directed to older adults, considering the Unified Health System (SUS) guidelines.
For the study of vulnerability, the social assessment is also one of the components in Ayres et al.3 definition; however, in that study municipality data for this analysis and their indicators were not found. According to the literature, Belo Horizonte Municipal Health Department (MG) makes available, under public domain, the Health Vulnerability Index5. This index is considered as a synthetic measure aimed at identifying risk and social vulnerability areas, thus contributing to municipal managers’ decision making.
Given the above, this study aimed at building Social and Programmatic Indices for community older adults and verifying the association among the vulnerability components (individual, social and programmatic).
METHOD
Quantitative population-based study, household survey type, transversal and observational, conducted with older adults living at home in the municipality of Uberaba - MG.
This study was submitted and approved by the Ethics Committee of Ribeirão Preto Nursing School, São Paulo University, under nº 1780.154.
For definition of the sample, the multistage cluster sampling technique was used. The sample size was calculated using prevalence of functional impairment in Instrumental Activities of Daily Living of 28.8%, 1.5% precision and 95% confidence interval, for a finite population estimated in 36,703 older adults. Thus, a minimum sample of 673 older adults was obtained. Considering the possibility of 20% loss in the sampling, the maximum number of attempts was 808 older adults. It is worth mentioning that for the selection of participants, 50% of the municipality census tracts were drawn (204), setting, then, four older adults per sector in order to secure sample self-weighting sampling. Therefore, a total sample of 816 older adults was obtained (Figure 1).
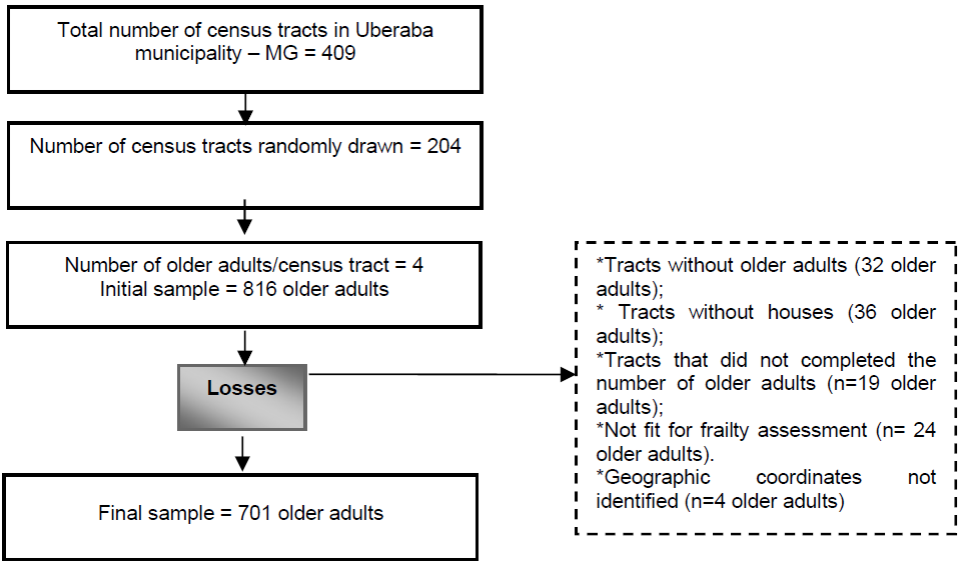
Data collection occurred from January to April 2014 in the older adults’ homes. Inclusion criteria were: be 60 or more than 60 years old, not present cognitive decline and reside in urban area.
The sampling loss resulted from: census tracts without older adults (n=32), without houses (n=36 older adults) and that did not make up the number of older adults (n=19). Older adults that did not make frailty phenotype tests (n=24) and did not identify geographic coordinates (n=4) were excluded (Figure 1).
Before starting interviews, a cognitive assessment of the older adults was made with the Mini-Mental State Examination (MMSE), translated and validated in Brazil11.
The socio-demographic and economic data characterization contemplated the following variables: sex (male and female); age group, age (60|-70, 70|-80 and 80 and above); marital status (with and without partner); schooling, years of study (without schooling, 1├4, 4├9, 9 and above); household patterns (alone and accompanied); and monthly individual income in minimum wages (< 1, 1, 1 ┤3, 4 and above).
For assessment of social vulnerability, the SVI (social vulnerability index) was developed for the present study municipality, resorting to the Health Vulnerability Index.5 The SVI construction in the present study was based on data from the last Demographic Census, considering as analysis unit the census tracts. In Uberaba, it was observed that there were 435 census tracts classified as urban. From this total, 392 tracts were included for calculation of the SVI, due to the exclusion of 17 for presenting confidential data or built with exclusively collective residences, and 26 for being out of the urban area limits, though having been classified as such.
The SVI was prepared based on the analysis of eight indicators in two dimensions (sanitation and socio-demographic)5. For calculation of each indicator, first, the variables of interest were selected in the list of public domain data available on IBGE website. Then, an electronic spreadsheet was prepared in Excel® with the variables of interest for calculation of SVI.
After the calculation of the eight indicators, scale standardization was conducted to enable their comparison and aggregation, since each indicator represented one measure of scale. For such, the following formula was used:

Later, weights were assigned to each indicator and their dimensions 5. Based on the final SVI calculation, the census tracts were categorized according to the following cutoff points as proposed by the Health Vulnerability Index 5. Then, the older adults were assessed considering the vulnerability level of the vector in which they fit, and the variable was re-categorized as low, medium and high/very high social vulnerability.
Individual vulnerability was assessed by means of five components of the frailty phenotype 4, as described in previous study 12. Older adults with three or more of these items were classified as frail, while those with one or two items were classified as pre-frail. Older adults with all tests negative for frailty syndrome were considered non frail4; and so, they were considered non vulnerable in this dimension.
The programmatic component was analyzed with an index of access and use of health services, called Programmatic Vulnerability Index. The assessment of access and use of health services utilized 32 items of two sections of the questionnaire National Household Sample Survey13.
For calculation of the index, to each category previously encoded answers of the instrument were assigned, individual weights (from 0 to 1), and the highest value represented better access/use for the item. To meet this criterion, five variables were excluded from the instrument for being qualitative. Later, the individual weights were added to form the score generated, which underwent the adherence test to normal distribution, and, even while using transformations, such as the logarithmic, adherence was not observed.
Therefore, the Principal Component Analysis technique14 was used to summarize the information contained in the variables to a small number of components that explains the higher variance of data from linear combinations among them.
Based on that, the first principal components that retained, approximately, 78% of variance (eigenvalue > 1.0) were selected. For each component, the variables with higher factor loading were selected and they were included in the calculation of the programmatic vulnerability score. Hence, the representative programmatic vulnerability index (vulprog) resulted in the multiplication of factor loadings by the value of variables selected, as demonstrated by the following equation.

It is worth mentioning that lower scores represent higher vulnerability in this component. The score was later classified in three categories using the cutoff points corresponding to the three distributions (low, medium and high) of vulnerability in this component.
For data processing electronic spreadsheets were built in Excel®. After consistency verification, the data bank was exported to the Statistical Package for the Social Sciences - SPSS 22.0 for purpose of data analysis. The construction of thematic maps and the exploratory descriptive spatial analysis used QGIS program, version 2.12.
Category variables were analyzed with absolute and percentage frequencies and for numeric categories mean and standard deviation were used. To represent the tracts distribution according to SVI, spatially, exploratory descriptive spatial analysis was performed, while for verification of the association among the vulnerability components association measurements in contingency Tables were used (chi-square test). The tests were considered significant where p<0.05.
RESULTS
In the sample studied, most of the older adults were female (n=468; 66.8%), under 60├ 70 years age group (n=302; 43.1%), without partners (n=406; 57.9%), lived with a companion (n=552; 78,7%), with 4 ├ 9 years of education (n=303; 43.2%) and with 1 minimum wage of income (n=317; 45.2%).
In the analysis of the municipality SVI, it was observed that most census tracts presented medium risk of social vulnerability (n=194; 49.49%), followed by low risk (n=116; 29.59%). It was also observed that these tracts spatial distribution did not occur homogeneously and randomly, as demonstrated in Figure 2. The tracts located in the municipality outskirts presented very high social vulnerability, while those from central areas were classified, most of them, as low and medium levels (Figure 2).
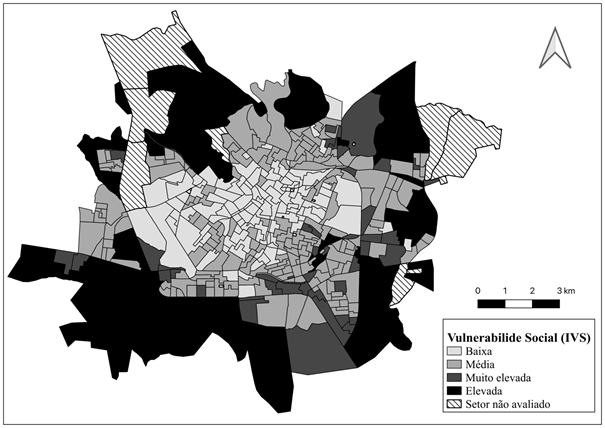
Figure 2: Spatial distribution of census tracts in Uberaba - MG, according to SVI, Uberaba, MG, Brazil, 2014.
Based on the census tract of participants’ residence, it was verified that 53.8% (n=377) of the older adults lived in areas with low social vulnerability; 30.5% (n=214) low; and 15.7% (n=110) high/very high.
With regard to Programmatic Vulnerability Index, the variables representative of each component, in descending order of the factor loading and importance, were: 1) access to dentist via SUS (0.8219); 2) main reason for not having bought medications (0.7916); 3) search for the same location of services (0.7779); 4) received continuous use medications for free (0.6356); 5) search for health care for the same reason in the last two weeks (0.5558); 6) were prescribed medications in the last service (0.5402); 7) consultation to dentist (0.5175); 8) purchase of medications not received for free (0.4944); 9) use of continuous use medications (0.3613) and 10) search for service related to their own health in the last two weeks (0.3583). It should be emphasized that the first and second components corresponded, respectively, to 27.15% and 10.52% of the explained variance. The others presented similar variances, between 7.58 and 3.71.
Based on this analysis, it was verified that the programmatic vulnerability score of the older adults ranged from 0.129 to 4.93, with mean 1.90 and standard deviation 0.61. Based on the distribution thirds, the older adults were classified as low (score > 2.09), medium (score between 1.76 and 2.09) and high (score < 1.76) programmatic vulnerability.
With regard to the individual component, it was identified that 16% (n=112) of the older adults were frail; 52.2% pre-frail (n=366) and 31.8% non frail.
While analyzing the relation among vulnerability components it was observed that most of them (n=224; 32%) concomitantly presented the three conditions for social, individual and programmatic vulnerability. It was also verified low percentage of older adults presenting only one of the vulnerabilities, 7.1% (n=50) high/very high social vulnerability; 5.8% (n=41) pre-frailty/frailty and 6.8% (n=48) medium/high programmatic vulnerability. Only 3.9% (n=27) did not present any of these conditions (Figure 3).
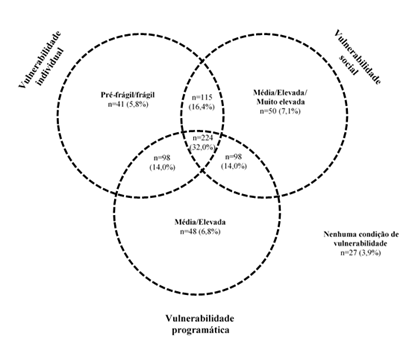
Figure 3: Older adults’ distribution according to individual, social and programmatic vulnerability condition, Uberaba, MG, Brazil, 2014.
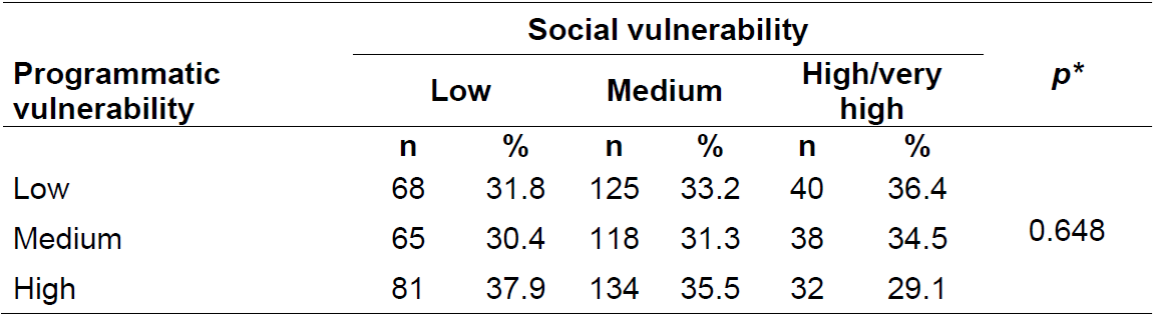
While comparing older adults distribution according to individual, social and programmatic vulnerability (Tables 1 and 2), it was verified lower proportion of frail older adults (n=30; 26.8%) with high programmatic vulnerability against those that are pre-frail (n=125; 34.2%) and not frail (n=92; 41.3%) (p=0.011). Significant difference was not found when comparing individual vulnerability and the social component (p>0.05), or when comparing social and programmatic vulnerabilities (p>0.05).
Table 1: Association of social and individual vulnerability components of older adults, Uberaba, MG, Brazil, 2014.
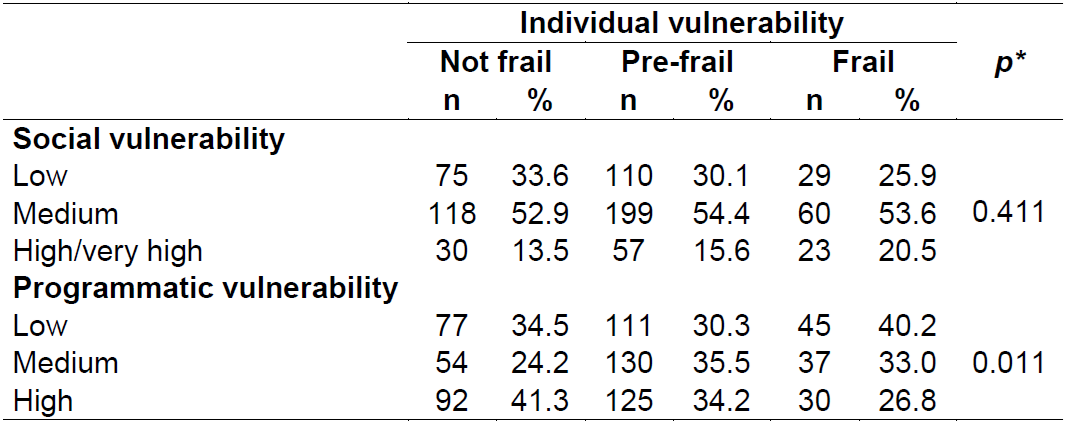
*p<0.05.
DISCUSSION
The social vulnerability impact on older adults’ health has been limited to socio-economic characteristics. Since all social circumstances are complex, experts in the field have considered the social vulnerability concept from a holistic point of view, quantifying it with indicators. The study demonstrated the wide potential for their application to determine risk of adverse outcomes in older adults health condition15.
While considering SVI spatial distribution, it was verified that those older adults who lived in the outskirts of the city presented higher levels of social vulnerability, which corroborates another study conducted in Brazil16. Considering the principles of the Unified Health System (SUS), reduction in social inequality should contemplate guarantee of access to health services and social protection resources to more vulnerable populations. Therefore, the population in this study was also assessed according to the programmatic vulnerability index, which can contribute to indirectly assess the Health System equality9.
In a systematic review protocol, the authors concluded that dental services presented higher social inequality in terms of accessibility, thus corroborating the present study for demonstrating that access to dentist was the most representative variable of the Programmatic Vulnerability Indicator17. In countries with universal health system, like Brazil, the increase in offer of dental public services may contribute to the accessibility of older adults, and, therefore, has an effect in this population dental health. Moreover, it is relevant to raise older adults’ knowledge about oral diseases and early treatment, in order to prevent dental losses18)(19)(20.
With regard to access to medications, it is known that the cost of medications was the main problem in health services reported by older adults, and is considered one of the main forms of showing social inequality21. These data denote signs of insufficient access to medications by older adults in SUS. Still, the expansion of Family Health Strategy (ESF) has contributed to improve access to these resources22.
It should be emphasized that ESF is considered priority proposal to improve the health system in the consolidation of SUS principles. However, ESF quality is directly associated to the capacity of effectuating the attribute of the first contact of the population, that is, it becomes priority service to the population whenever there is a new problem/episode that needs attention to health23. Though the present study did not assess the specific place of service, this information indirectly corroborates the data, since regularity in the search of services location was considered one of the variables indicating programmatic vulnerability.
In the present study, it was also observed that most of the older adults presented the three vulnerability conditions concomitantly. It is known that in the ageing process there may arise biological vulnerability, which, while interacting with the socio-cultural process, the cumulative effects of deficient conditions of education, income and health as old age comes, and the habits of our modern life7, can expose older adults to multiple vulnerability conditions.
It is consensual that vulnerability components are correlated and also influence the health conditions of older adults17. There was particularly lower proportion of frail older adults with high programmatic vulnerability against pre-frail and non frail older adults. Despite that, it was observed that 5.8% and 7.1% of the older adults presented only physical frailty and high/very high social vulnerability, respectively. It can be inferred that not all vulnerable populations present frailty condition, that is, social vulnerability and frailty can be associated and also overlapped; however, these are distinct constructions that affect the older adults; which was also suggested by other researchers17. These findings support contributions developed by Ayres et al.3 where individual, social and programmatic components are interdependent.
The present investigation presented potential limitations: a) transversal design that makes unfeasible causal relation of the events studied; b) use of a synthetic indicator of social vulnerability, with which this aspect can’t be identified at individual level, for considering homogeneity in the census tract. Studies with multicentre cohort should be conducted, considering individual social vulnerability measures, to contribute to the planning of policies for attention to this population, particularly those more vulnerable.
Despite the limitations in this study, the findings demonstrate the importance of a wide understanding of older adults’ vulnerability, having as guiding axis the individual, social and programmatic aspects. These contributions may represent a possibility of change of paradigm that will better subsidize nursing interventions in the healthcare provided to older adults.
However, the applicability of the vulnerability concept in practice is still a challenge, since the health system is fragmented and disarticulated, focused on the biomedical model and, therefore, incapable of offering integral and continuous care23 to the older population. The older population, in face of this situation, becomes one of the most compromised due to its higher susceptibility and, consequently, higher need to use health resources, which means investment in innovative practices that will transcend the biological aspects’ limitations.
The SVI and the Programmatic Vulnerability Index construction in this study can contribute to make available technology with easy access and quick, both for assessment of the population by means of surveys and managers in decision making of public policies, considering the need to ensure social justice.
CONCLUSION
Data in this study suggest that Social and Programmatic Vulnerability Indices represent important assessment tools for municipal health managers, particularly considering the multiple conditions of vulnerability to which older adults can be exposed (individual, social and programmatic) during the ageing process. Such data reveal the need to consider a multidimensional approach to vulnerability to plan several health care services for this population.
REFERENCIAS
1. Wang J, Lin W, Chang LH. The linear relationship between the Vulnerable Elders Survey-13 score and mortality in an Asian population of community-dwelling older persons. Arch Gerontol Geriatr [Internet]. 2018 [cited 2021 Fev 8]; 74:32-38. Available from: doi: 10.1016/j.archger.2017.09.005. [ Links ]
2. Brocklehurst H, Laurenson M. A concept analysis examining the vulnerability of older people. Br. J. Nurs [Internet]. 2008 [cited 2021 Fev 8]; 17(21):1354-1357. Available from: doi: 10.12968/bjon.2008.17.21.31738. [ Links ]
3. Ayres JRC, Paiva V, França Junior I. From natural history of disease to vulnerability: changing concepts and practices in contemporary public health. In: Parker R, Sommer M, organizators. Routledge handbook in global public health. New York: Taylor & Francis; 2011, p. 98-107. [ Links ]
4. Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci [Internet]. 2001 [cited 2021 Fev 8]; 56(3):146-56. Available from: https://doi.org/10.1093/gerona/56.3.M146 [ Links ]
5. Belo Horizonte. Secretaria Municipal de Saúde. Índice de vulnerabilidade da saúde 2012 [Internet]. 2013 [cited 2021 Fev 8]. Available from: https://prefeitura.pbh.gov.br/sites/default/files/estrutura-de-governo/saude/2018/publicacaoes-da-vigilancia-em-saude/indice_vulnerabilidade2012.pdf [ Links ]
6. Lourenço RA, Moreira VG, Mello RGB, Santos IS, Lina SM, Pinto ALF, et al. Consenso brasileiro de fragilidade em idosos: conceitos, epidemiologia e instrumentos de avaliação. Geriatr Gerontol Aging. [Internet]. 2018 [cited 2021 Fev 8]; 12(2):121-35. Available from: doi: 10.5327/Z2447-211520181800023. [ Links ]
7. Rodrigues NO, Neri AL. Vulnerabilidade social, individual e programática em idosos da comunidade: dados do estudo FIBRA, Campinas, SP, Brasil. Ciência & Saúde Coletiva [Internet]. 2012 [cited 2021 Fev 8]; 17(8): 2129-39. Available from: https://doi.org/10.1590/S1413-81232012000800023 [ Links ]
8. Santiago LM, Gobbens RJJ, VanAssen MALM, Carmo CN, Ferreira DB, Mattos IE. Predictive validity of the Brazilian version of the Tilburg Frailty Indicator for adverse health outcomes in older adults. Archives of Gerontolgy and Geriatrics [Internet]. 2018 [cited 2021 Fev 8];76:114-119. Available from: doi: 10.1016/j.archger.2018.02.013. [ Links ]
9. Pereira BS, Tomasi E. Instrumento de apoio à gestão regional de saúde para monitoramento de indicadores de saúde. Epidemiol. Serv. Saúde [Internet]. 2016 [cited 2021 Fev 8];25(2):411-418. Available from: https://doi.org/10.5123/s1679-49742016000200019 [ Links ]
10. Lima-Costa MF, Facchini LA, Matos DL, Macinko J. Mudanças em dez anos das desigualdades sociais em saúde dos idosos brasileiros (1998-2008). Rev Saúde Públ [Internet]. 2012 [cited 2021 Fev 8];46:100-7. Available from: https://doi.org/10.1590/S0034-89102012005000059 [ Links ]
11. Bertolucci PHF, Brucki SMD, Campacci SR, Juliano Y.O mini-exame do estado mental em uma população geral. Impacto da escolaridade. Arq neuropsiquiatr [Internet]. 1994 [cited 2021 Fev 8];52(1):1-7. Available from: https://doi.org/10.1590/S0004-282X1994000100001 [ Links ]
12. Alves MKL, Oliveira NGN, Pegorari MS, Tavares DMS, Rodrigues MCS, Bolina AF. Evidence of association between the use of drugs and community-dwelling older people frailty: a cross-sectional study. Sao Paulo Med. J [Internet]. 2020 [cited 2021 Apr 09];138(6):465-474. Available from: https://doi.org/10.1590/1516-3180.2020.0205.r1.06082020 [ Links ]
13. Instituto Brasileiro de Geografia e Estatística. Pesquisa Nacional por Amostra de Domicílios [Internet]. Rio de Janeiro: IBGE; 2008 [cited 2021 Fev 8]. 129p. Available from: https://biblioteca.ibge.gov.br/visualizacao/periodicos/59/pnad_2008_v29_br.pdf [ Links ]
14. Jolliffe IT. Principal Component Analysis. 2. ed. New York: Springer; 2002. 487p. [ Links ]
15. Andrew MK, Keefe JM. Social vulnerability from a social ecology perspective: a cohort study of older adults from the National Population Health Survey of Canada. BMC Geriatrics [Internet]. 2014 [cited 2021 Fev 8];14(90). Available from: https://doi.org/10.1186/1471-2318-14-90 [ Links ]
16. Barbosa IR, Gonçalves RCB, Santana RL. Mapa da vulnerabilidade social do município de Natal- RN em nível de setor censitário. J. Hum. Growth Dev [Internet]. 2019 [cited 2021 Apr 9]; 29(1):48-56. Available from: https://doi.org/10.7322/jhgd.157749 [ Links ]
17. Almeida APSC, Nunes BP, Duro SMS, Facchini LA. Determinantes socioeconômicos do acesso a serviços de saúde em idosos: revisão sistemática. Rev. Saúde Públ [Internet]. 2017 [cited 2021 Fev 8]; 51:50. Available from: http://dx.doi.org/10.1590/s1518-8787.2017051006661 [ Links ]
18. Machado LP, Camargo MBJ, Jeronymo JCM, Bastos GAN. Uso regular de serviços odontológicos entre adultos e idosos em região vulnerável no sul do Brasil. Rev. Saúde Públ. [Internet]. 2012 [cited 2021 Fev 8];46(3):526-33. Available from: http://dx.doi.org/10.1590/S0034-89102012000300015 [ Links ]
19. Fonseca EP, Fonseca SGO, Meneghim MC. Fatores associados ao uso dos serviços odontológicos por idosos residentes no estado de São Paulo, Brasil. Rev. bras. geriatr. gerontol. [Internet]. 2017 [cited 2021 Apr 12]; 20(6):785-796. Available from: https://doi.org/10.1590/1981-22562017020.170095 [ Links ]
20. Oliveira RFR, Souza JGS, Haikal DSA, Ferreira EF, Martins AMEBL. Equidade no uso de serviços odontológicos provenientes do SUS entre idosos: estudo de base populacional. Ciênc. saúde coletiva [Internet]. 2016 [cited 2021 Apr 12]; 21(11):3509-3523. Available from: https://doi.org/10.1590/1413-812320152111.22532015 [ Links ]
21. Restrepo SF, Vieira MRS, Barros CRS, Bousquat A. Gasto privado com medicamentos entre idosos e o comprometimento da renda familiar em município de médio porte no estado de São Paulo. Rev. bras. epidemiol. [Internet]. 2020 [cited 2021 Apr 12];23:e200042. Available from: https://doi.org/10.1590/1980-549720200042 [ Links ]
22. Costa KS, Francisco PMSB, Barros MBA. Utilização e fontes de obtenção de medicamentos: um estudo de base populacional no Município de Campinas, São Paulo, Brasil. Cad. Saúde Pública [Internet]. 2016 [cited 2020 Mar 09];32(1):e00067814. Available from: https://doi.org/10.1590/0102-311X00067814 [ Links ]
23. Souza LEPF, Paim JS, Teixeira CF, Bahia L, Guimarães R, Almeida-Filho N, et al . Os desafios atuais da luta pelo direito universal à saúde no Brasil. Ciênc. saúde coletiva [Internet]. 2019 [cited 2021 Apr 09];24(8):2783-2792. Available from: http://dx.doi.org/10.1590/1413-81232018248.34462018 [ Links ]
Received: April 19, 2021; Accepted: September 14, 2021
 Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
Este es un artículo publicado en acceso abierto bajo una licencia Creative Commons
