










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkMedicina Oral, Patología Oral y Cirugía Bucal (Internet)
versión On-line ISSN 1698-6946
Med. oral patol. oral cir.bucal (Internet) vol.11 no.2 mar./abr. 2006
Neuropatías trigeminales tumorales: presentación de 7 casos
Neoplastic trigeminal neuropathy: presentation of 7 cases
Miguel Peñarrocha Diago 1, Elena Mora Escribano 2, José V. Bagán 3, María Peñarrocha Diago 4
(1) Assistant Professor of Oral Surgery Medical and Dental School. University of Valencia
(2) Dentist (DDS). Master of Oral Surgery and Implantology.
Medical and Dental School. University of Valencia
(3) Chairman of Oral Medicine. Medical and Dental School.
University of Valencia.
Head of the Service of Stomatology, Valencia University
General Hospital
(4) Doctor of Medicine and Surgery. Doctor of Odontology.
Private practice in Valencia
ABSTRACT
Trigeminal neuropathy of neoplastic origin accounts for a small percentage of trigeminal neuropathies, though the prognosis may be very poor. It is important to discard neoplastic processes in patients with numbness of the trigeminal territory. We present 7 cases of trigeminal neuropathy secondary to tumors: in four cases there were antecedents of systemic neoplastic disease, while in the remaining three cases neuropathy was the first manifestation of the tumor. The lesion was located in the mandible in three cases, in the region of the skull base in one patient, and in the brainstem and brain in one case each. In one case the lesion level could not be identified. The course was very poor in 5 cases. Recovery was only recorded in one patient in whom the symptoms were seen to disappear after acoustic nerve neurinoma resection. The lesions underlying neoplastic trigeminal neuropathy can be located at any point along the trajectory of the trigeminal nerve, and their prognosis is very poor.
Key words: Trigeminal neuropathy, neoplasms, malignant trigeminal neuropathy.
RESUMEN
Las neuropatías del trigémino de origen tumoral suponen un bajo porcentaje de las neuropatías trigeminales, pero pueden tener muy mal pronóstico. Es importante descartar una neoplasia en los pacientes con adormecimiento en el territorio del trigémino. Presentamos 7 casos de neuropatías trigeminales secundarias a tumores; en 4 existían antecedentes de neoplasias sistémicas previas y en 3 la neuropatía fue el primer signo de la enfermedad tumoral. En tres ocasiones la lesión se localizó en mandíbula, una en base de cráneo, una en troncoencéfalo, una a nivel cerebral y en una no se encontró el nivel lesional. La evolución fue muy mala en 5 pacientes; sólo se recuperó un caso en el que tras la resección de un neurinoma del acústico desaparecieron los síntomas. Las lesiones que producen neuropatías trigeminales tumorales pueden localizarse a lo largo de todo el trayecto trigeminal y las neoplásicas tienen un pronóstico ominoso.
Palabras clave: Neuropatía trigeminal, neoplasias, neuropatía trigeminal maligna.
Introduction
Trigeminal neuropathies (TNs) manifest as skin and mucosal numbness in the region innervated by the trigeminal nerve (1). Their importance is explained by the fact that TN may represent the first manifestation of tumor disease, or of relapse in patients with prior neoplastic processes. As such, these manifestations are ominous, and patient life expectancy is often short (2). TN frequently reflects metastatic invasion or contiguity spread of the tumor lesion to the cranial nerves (3). TNs have been reported secondary to the following processes: tumors located in the region of the pontocerebellar angle (4), Gassers ganglion, the trigeminal roots (5), or nasopharynx and maxillary sinus (6); and mandibular benign (7) or malignant lesions (8-10).
The degree of involvement and the location of the lesion are highly variable. Despite availability of the most recent early diagnostic techniques, it is difficult to differentiate "benign" TN from "malignant" tumor-associated presentations. Early clinical and radiological evaluation is of crucial importance (11). In the event of sensory defects in the territory of the trigeminal nerve, the presence of a primary tumor or of metastatic relapse of malignant disease at some point along the trigeminal trajectory must be discarded (12).
The present study describes 7 patients with neoplastic trigeminal neuropathies. An evaluation is made of the clinical manifestations, the location and etiological diagnosis of the lesions, and patient evolution.
Material and method
The study includes the cases of neoplastic trigeminal neuropathies seen in the Dental Clinic of the School of Medicine and Dentistry (Valencia University, Spain) in the period between 1988 and 2002. The relevant patient data and antecedents were recorded. The diagnosis of TN was based on the clinical manifestations. All patients reported orofacial numbness in the territory of one or more branches of the trigeminal nerve, and clinical examination revealed sensory defects of one or more branches of this nerve (12). The presence or absence of pain associated to the sensory defect was documented, along with the type of pain and its response to pharmacological treatment.
Clinical exploration was made of the oral cavity and cranial nerves. An extraoral panoramic X-ray study was made in all cases, together with maxillofacial or brain computed tomography (CT) and/or brain magnetic resonance imaging (MRI). In patients with mandibular lesions, the latter were subjected to biopsy, while patients with central nervous system disorders underwent biopsy or surgery, depending on the process involved. The treatment provided and the course of the disease were documented.
Results
Seven patients were studied. The mean age was 47 years (range 35-72 years). There were four males and three females (Table 1). As to the personal antecedents, two patients had a history of breast tumors (cases 1 and 4), one had prostate cancer (case 3), and one presented lip carcinoma (case 3).
Three patients referred pain of a neurogenic nature (cases 1, 2 and 5), located in the trigeminal territory affected by the neuropathy. Pain intensity was great in all cases, with good initial response to pharmacological treatment in the form of carbamazepine and amitriptyline. In cases 1 and 2 the pain was atypical, continuous and with added crises. As the disease process evolved, the pain worsened, and the medication became less effective. In the patient with acoustic nerve neurinoma the pain exhibited typical features (fulgurating and characterized by crises lasting seconds), and improved with carbamazepine. The pain disappeared after surgical treatment of the tumor.
As to the location of the sensory defect, four patients showed involvement of the territory of the mental nerve, while one patient presented combined involvement of the second and third trigeminal branches. One subject showed involvement of all three branches.In one patient the sensory defect was located on the left side (case 5), while in 6 cases it was confined to the right side of the face.
The intraoral exploration only detected anomalies in case 2, in the form of a mass in the mandibular retromolar trigone. The clinical examination revealed no alterations in trigeminal motor function. As regards the rest of the cranial nerves, case 5 presented left hypoacusia, while the rest of patients showed no alterations.
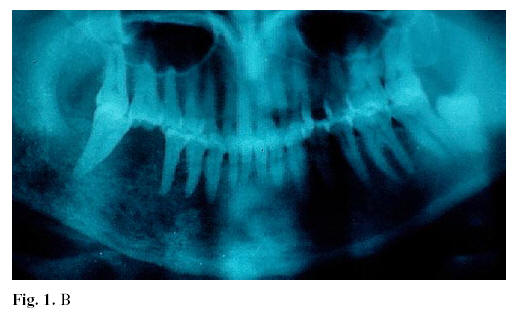
Orthopantomography and maxillofacial CT identified mandibular osteolytic lesions in three patients: squamous cell carcinoma of the mandibular angle was recorded in case 2, corresponding to a patient who had undergone surgery for lower lip squamous cell carcinoma three years before. The remaining three cases corresponded to mandibular metastatic lesions secondary to breast cancer (case 4)(Fig. 1, A, B and C) and lung cancer (case 7).

In three cases brain CT or MRI revealed alterations. In this context, case 5 presented an acoustic nerve neurinoma within the pontocerebellar angle, while case 1 corresponded to a metastatic lesion that destroyed the tip of the petrosal bone in a patient with a history of breast cancer (Fig. 2 A and B). Lastly, case 6 corresponded to a brain tumor initially manifesting as facial numbness the final diagnosis being glioblastoma multiforme (Fig. 3. A and B).
In case 3 we observed no orthopantomographic or brain or maxillary CT alterations. This patient had been diagnosed with prostate cancer.
In cases 1, 4 and 7 (Table 2), TN was caused by distant metastases of systemic cancers. Case 2 corresponded to local spread of a lower lip carcinoma possibly via the perineural route. In all four patients TN was the first sign of relapse of the malignancy. In case 3 neuropathy of the chin region manifested in a patient with a previous prostate neoplasm, though metastasis could not be demonstrated. In cases 5 and 6, facial numbness was the first sign of the disease (corresponding to acoustic nerve neurinoma and glioblastoma multiforme, respectively), while in case 7 TN was the first sign of metastatic spread of an occult tumor subsequently identified as lung adenocarcinoma.
Regarding treatment, in the cases of pain the patients received carbamazepine and/or amitriptyline, together with specific management for the associated neoplastic process. The patients with antecedents of systemic malignancy were subjected to chemotherapy, both in the case of radiological manifestations of metastatic lesions (in the base of the skull (case 1) or mandible (cases 4 and 7), and in those patients without evidence of metastasis (case 3). One patient (case 6) with cerebral glioblastoma multiforme received chemotherapy, in the same way as another patient (case 2) with perineural metastatic spread of lip cancer affecting the lower jaw. Case 5 (acoustic nerve neurinoma) underwent surgery.
Regarding the course of the disease, the patients showed slow progression from the onset of symptoms to the diagnosis of TN: from 6 months in case 1, to three years in case 3. In the latter patient TN coincided with the diagnosis of systemic tumor spread. In case 6 the clinical manifestations corresponded to TN of the second and third branch and remained stationary during 6 months. There was no associated pain or involvement of other cranial nerves suggesting the existence of a lesion in the sensory roots of the nerve, in Gassers ganglion, or in the corresponding branches. However, brain MRI demonstrated the presence of a space-occupying cortical lesion. Posteriorly, the patient developed sensory alterations of the contralateral upper limb and other clinical manifestations.
Regarding the duration of follow-up, four patients died within the first year (cases 2, 4, 6 and 7), while case 3 died after 13 months. Case 1 failed to improve of the neuropathy during the 8-month follow-up period (this patient was subsequently lost to follow-up), and only case 5 showed clinical recovery (acoustic nerve neurinoma).
Discussion
The importance of the diagnosis of neoplastic trigeminal neuropathy is that the disorder may manifest in the context of a systemic neoplastic process, and in some cases can precede the diagnosis of the malignancy (9,13). In this context, in the review by Massey et al. (14), 47% of the patients reported dysesthesias prior to diagnosis of the cancer. This fact makes it necessary to explore the presence of a possible occult neoplasm in non-oncological patients diagnosed with mental nerve neuropathy focusing special attention on bronchopulmonary and breast malignancies and lymphoproliferative processes, which represent the most common underlying etiologies. Vadell et al. (12) presented 5 patients in the context of progressing disease. TN manifested in two of our patients with antecedents of breast adenocarcinoma, in one patient with prostate cancer, and in another individual with lip carcinoma. In all of these cases numbness of the trigeminal territory was the first sign of neoplastic relapse. In the remaining three cases, TN was the first manifestation of the disease: two primary tumors (one benign and the other malignant), and a case of tumor metastasis.
Clinically, neoplastic trigeminal neuropathies can manifest as numbness or numbness with pain, in an association of deficiency and irritative symptoms (15,16). Malignant mental neuropathy is characterized by spontaneous, non-traumatic anesthesia of the region innervated by the mental nerve. The sensory defect includes the skin and mucosa of the lower lip (14). All of our patients showed involvement of the mental nerve, either alone or in combination with one or both of the remaining trigeminal nerve branches. Tumors affecting the trigeminal nerve may cause atypical neuralgia with sensory loss the associated pain being intense, with progressive neurological impairment (17). In our series there was associated neurogenic pain in three cases. The pain was described as fulgurating and lasted seconds in one patient, while in the rest the pain exhibited atypical characteristics. Calvin et al. (18) suggested that such pain may be caused by tumor compression of the sensory roots of the trigeminal nerve, resulting in areas of demyelization.
Different authors have stressed the importance of performing a complete radiological study of patients with trigeminal neuropathy, in order to discard the possible existence of a lesion in the brain, brainstem, preganglionic region, in Gassers ganglion or in the cavernous sinus, or in the extracranial zone of the three trigeminal branches with exploration of the entire trajectory of the fifth cranial nerve (12,19-22). In TN it is necessary in all cases to discard a possible tumor lesion - benign (7,8) or malignant (12) at any point along the trajectory of the trigeminal nerve, and the lesion cannot be located based on the clinical signs and symptoms alone. Three of our patients presented mandibular carcinomas. In the patient with prostate cancer we detected no radiographic lesions; this case may have corresponded to a paraneoplastic lesion, as has been suggested by some investigators (14). The patient with a neurinoma in the pontocerebellar angle presented atypical neurogenic pain together with TN and hypoacusia. Another patient had a brain lesion initially manifesting as contralateral facial numbness.
Regarding treatment, and once the background disease causing the neuropathy had been diagnosed, our patients were referred to the required specialists for systemic therapy. In the case of operable malignant or benign tumors, surgery is indicated as in our patient with an acoustic nerve neurinoma. Carbamazepine and amitriptyline were prescribed in the cases presenting neurogenic pain, with initial partial symptoms improvement.
The appearance of TN of malignant origin is classically associated with a poor prognosis involving a short patient life expectancy, and is regarded as an ominous sign of the disease (23). Laurencet et al. (2) reported a mean survival after the diagnosis of malignant TN of less than one year. In our series, 5 patients had a very poor prognosis, with short survival: most died within one year of follow-up. Of note is the fact that a considerable period of time elapsed from the onset of facial numbness to the diagnosis of TN. This may have been because the patients did not consider the symptoms to be particularly important, and did not seek medical help. Only one of our patients showed complete recovery. This case corresponded to a neurinoma of the acoustic nerve, and all the clinical manifestations disappeared after surgical removal of the tumor.
If a patient with a tumor develops trigeminal facial numbness, the condition should be regarded as evidence of tumor relapse with a very poor associated prognosis. In the event of facial numbness manifesting in a patient without disease antecedents of interest, the location of the lesion should be established, with diagnosis of the disorder, and considering that the condition may effectively correspond to the first manifestation of a neoplastic process.
![]() Correspondence
Correspondence
Dr. Miguel Peñarrocha Diago
Clínica Odontológica
Gascó Oliag, 1
46021- Valencia
E-mail: miguel_Peñarrocha@uv.es
References
1. Calverley JR, Mohnac AM. Syndrome of the numb chin. Arch Intern Med 1963; 112:819-21. [ Links ]
2. Laurencet FM, Anchisi S, Tullen E, Dietrich PY. Mental neuropathy: report of five cases and review of the literature. Crit Rev Oncol Hematol 2000;34:71-9. [ Links ]
3. Dalmau J, Grauss F. Neuropatía mentoniana. Neurología 1986;1:203-11. [ Links ]
4. Bodner L, Oberman M, Shteyer A. Mental nerve neuropathy associated with compound odontoma. Oral Surg Oral Med Oral Pathol 1987; 63:658-60. [ Links ]
5. Heng CK, Heng J. Implications of malignant lymphoma on a periapical mandibular lesion. Gen Dent 1995;43:454-8. [ Links ]
6. Halachmi S, Maded R, Madjar S, Wald M, River Y, Nativ O. Numb chin síndrome as the presenting symptom of metastat carcinoma. Urology 2000;55:286-9. [ Links ]
7. Martí JF. Neuropatía craneal en el enfermo con cáncer sistémico. Neurología 1986;1:183-4. [ Links ]
8. Massey EW, Moore J, Schold S. Mental neuropathy from systemic canceer. Neurology 1981; 31:1277-81. [ Links ]
9. Vadell C, Tusquets I, Roquer J, Corominas JM, Nogue M, Gil M, et al. Neuropatía mentoniana asociada a neoplasis. Presentación de cinco casos y revisión de la literatura. Arch de neurobiol 1989;52,1:17-22. [ Links ]
10. Bullit E, Tew JM, Boyd J. Intracraneal tumors in patients with facial pain. J Neurosurg 1986;64:865-71. [ Links ]
11. Schnetler J. Intracraneal tumours presenting with facial pain. Br Dent J 1989;166:80-4. [ Links ]
12. Peñarrocha M, Peñarrocha MA, Soler F. Neuralgia trigeminal típica secundaria a tumores del ángulo pontocerebeloso. A propósito de dos casos. Medicina Oral 1997; 2:109-12. [ Links ]
13. Calvin WH, Laeser JD, Howe JP. A neurophysiological theory for the mechanism of the tic douloreus. Pain 1977; 3:147-54. [ Links ]
14. Peñarrocha M, Bagán JV, Alfaro A, Escrig V. Mental nerve neuropathy. Report of three cases. Oral Surg Oral Med Oral Pathol 1990;69:48-51. [ Links ]
15. Reyes N, Terron C, Martinez E, Zabala JA, Larrondo J. Progressive cranial neuropathy due to perineural spread of an squamous cell carcinoma. Neurologia 2003;18:112-5. [ Links ]
16. Manon-Espaillat R, Lanska DJ, Ruff RL, Masaryk T. Visualization of isolated trigeminal nerve invasion by limphoma using Gadolinium-enhanced magnetic resonance imaging. Neuroradiology 1990;32:531-2. [ Links ]
17. Cousin GC, Ilankovan V. Mental nerve anaesthesia as a result of mandibular metastases prostatic adenocarcinoma. Br Dent J 1994;177:382-4. [ Links ]
18. Peñarrocha M, Bagán JV, Alfaro A, Martinez V, Montalar J. Malignant mental nerve neuropathy. Case report and meta-analysis. Rev Neurol 1992;101:31-5. [ Links ]

