










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkMedicina Oral, Patología Oral y Cirugía Bucal (Internet)
versión On-line ISSN 1698-6946
Med. oral patol. oral cir.bucal (Internet) vol.11 no.2 mar./abr. 2006
Oral myiasis: A case report
Evandro Neves Abdo 1, Ausgusto César Sette-Dias 2, Cláudio Rômulo Comunian 1,
Carlos Eduardo Assis Dutra 1, Evandro Guimarães de Aguiar 3
(1) DDS, MSD
(2) DDS
(3) DDS, PHD. School of Dentistry of Federal Univesity from Minas Gerais- Brazil
ABSTRACT
Oral Myiasis is a rare pathology in humans and is associated with poor oral hygiene, alcoholism, senility, supuranting lesions, severe halitosis and others conditions. The treatment is a mechanical removal of the maggots one by one but a systemic treatment with Ivermectin, a semi-synthetic macrolide antibiotic, have been used for treatment for oral myiasis. We present a case report of a 32-year-old man indigent, alcohol-dependent with an extensive necrotic area and acute swelling in upper lip and fetid odor. The patients manegement included topic use of gencian violet, oral therapy with ivermectin (6 mg orally), surgical exploration to remove the larvae and necrotic tissue. After the complete larvae removal the swelling and the wounds were healing normally, the patients was referred to plastic surgery to repair tissue damage. The prevention of human myiasis is by education, but unfortunately in the developing countries some people live in low social condition, predisposing the occurrence of the infestation.
Key words: Myiasis, oral infestation, invermectin.
Introduction
The term myiasis (Greek: myi= fly) is used for refer the infestation of living tissues of humans and animals, by diptereous eggs or larvae (1).
The oral cavity is rarely affecting by this infestation (2) and the oral myiasis has been associated with poor oral hygiene, alcoholism, senility, supuranting lesions, severe halitosis and others conditions (1-5).
The myiasis can be classified as obligatory, when larvae develop in living tissue, or facultative, when maggots feed on necrotic tissue. The obligatory myiasis is more harmful for the humans. The most common anatomic sites for myiais are the nose, eye, lung, ear, anus, vagina and more rarely, the mouth (3).
The aim of this papers is to report an extensive case of myiasis in upper lip.
Report of Case
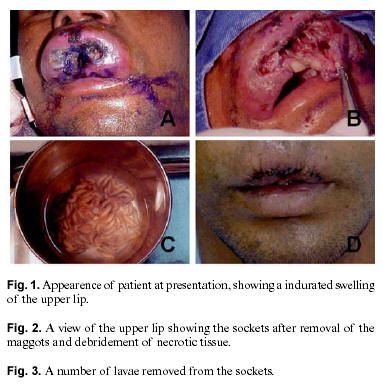
A 32-year-old man indigent, alcohol-dependent, living on streets, was brought to Odilon Behrens Hospital (OBH), in Belo Horizonte – Brazil, and presented with acute upper lip swelling with an extensive necrotic area and fetid odor. The oral examination revealed a diffused indurated swelling nonfluctuant on palpation (Fig. 1). In addition, general symptons including pain, fever and malaise were present. The patient was drunk, presenting a poor oral and general hygiene and was confused about the evolution time. The surface of the swelling revealed several orificies which lived a number of maggots, involving intra-orally mucolabial fold (Fig. 2). The management was performed by Oral and Maxillofacial Surgeons from Surgery and Pathology Department of de School Dentistry of the Federal University from Minas Gerais-Brazil. Complementary treatment to the general symptons was carried out in the clinic internal medicine of the OBH.
The patients manegement included topic use of gencian violet, oral therapy with ivermectin (6 mg orally), surgical exploration to remove the larvae (Fig. 3) and necrotic tissue. This procedure was carried out three times for remove the remaining maggots and was observed, in the last procedure after 5 days of hospitalization, which the larvae were mobile. After the complete larvae removal the swelling and the wounds were healing normally, the patients was referred to plastic surgery to repair tissue damage.
Discussion
Myiasis occurs by dipterous larvae developing in decaying tissues and the developmental transition via the larval stage requires an intermidiate host and the number of developing larvae depends on the number of viable eggs deposited (4). The late diagnostic and the number of maggots in this report, determined an extense tissue damage, have been necessary a esthetic surgery.
The myiasis is diagnosed clinically based on presence of the maggots (5-7) but the classification of the larvae rarely has been made. In the present case was no possible to identify the larvae.
The risk factors for oral myiasis include suppurative lesions, trauma in the face, mouth-breathers, extraction wonds and others conditions (6-9). In this report it was not possible to identify a local condition in the upper lip, however is possible suppose that trauma was the most probable local condition in the development of myiasis in an alcoholics and abandoned person.
The traditional management for myiasis is the mechanical removal of the maggots (6,7). When there are multiple larvae and in advanced stages of maggots development and tissue destruction, local application of several substances have been used to ensure complete removal of all larvae (2-5,7). Recently a systemic treatment with Ivermectin, a semi-synthetic macrolide antibiotic, have been used for treatment for oral myiasis (10).
In the present case after 5 days, the maggots were mobile despite the ivermectin therapy. The careful surgical removal of the larvae and the adequate debridement of necrotic tissue were the efficient treatment.
The prevention of human myiasis is by education, but unfortunately in the developing countries some people live in low condition, predisposing the occurrence of the infestation.
References
1. Millikan LE. Myiasis. Clin Dermatol 1999;17:191-5. [ Links ]
2. Pindborg JJ. Atlas of Diseases of the Oral Mucosa. Philadelphia: PA, Sauders; 1992. p. 84-5. [ Links ]
3. Hall MJR, Wall R. Myiasis of Humans and Domestic Animals. Adv Parasitol 1995;35:257-334. [ Links ]
4. Felices RR, Ogbureke KUE. Oral Myiasis: Report of Case and Review of Management. J Oral Maxilofac Surg 1996;54:219-20. [ Links ]
5. Gomez RS, Perdigão PF, Pimenta FJ, Rios Leite AC, Tanos de Lacerda JC, Custódio Neto AL. Oral Myiasis by Screwworm Cochliomy Hominivorax. Br J Oral Maxillofac Surg 2003;41:115-6. [ Links ]
6. Bhatt AP, Jayakrishnan A. Oral Myiasis: a case report. Int J Paediatr Dent 2000;10:67-70. [ Links ]
7. Al- Ismaily M, Scully C. Oral myiais: report of two cases. Int J Paediatr Dent 1995;5:177-9. [ Links ]
8. Hakimi R, Yazdi I. Oral Mucosa Myiasis Caused by Oestrus Ovis. Arch Iranian Med 2002;5:194-6. [ Links ]
9. Aguiar AMM, Enwonwu CO, Pires FR. Noma (cancrum oris) Associated with Oral Myiasis in an Adult. Oral Dis 2003;9:158-9 [ Links ]
10. Shinohara EH, Martini MZ, Oliveira Neto HG, Takahashi A. Oral Myiasis Treated with Ivermectin: Case Report. Braz Dent J 2004;15:79-81. [ Links ]
![]() Correspondence
Correspondence
Prof. Evandro Neves Abdo
Universidade Federal de Minas Gerais
Faculdade de Odontologia
Av: Antônio Carlos, 6627 sala 3204
Belo Horizonte, MG, Brasil.
CEP 31270901
E-mail: enabdo@uai.com.br
Received: 10-07-2005
Accepted: 30-10-2005

