










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkMedicina Oral, Patología Oral y Cirugía Bucal (Internet)
versión On-line ISSN 1698-6946
Med. oral patol. oral cir.bucal (Internet) vol.11 no.2 mar./abr. 2006
Transmigration of impacted lower canine. Case report and review of literature
Transmigración del canino inferior
incluido. Presentación de un caso y
revisión de la literatura
Daniel Torres Lagares1, Rafael Flores Ruiz2,
Pedro Infante Cossío3,
Manuel García Calderón3, José
Luis Gutiérrez Pérez4
(1) Assistant Professor of Oral Surgery. Professor of Master
of Oral Surgery
(2) Student. Master of Oral Surgery
(3) Associated Professor of Oral Surgery. Professor of Master
of Oral Surgery
(4) Titular Professor of Oral Surgery. Director of master of
Oral Surgery. Faculty of Odontology. University of Seville
ABSTRACT
Retention, that is, a permanent tooth which is unerupted more
than a year after the normal age of eruption, is a relatively rare event, except
in the case of the third molars and the upper canines. Transmigration is defined
as the phenomenon of more than half an unerupted impacted tooth crossing the
midline.
We report the clinical case of a twenty-year-old patient
presenting transmigration of the lower left canine, with a type 4 transmigration
pattern (Mupparapu). Likewise, we carried out a review of the literature of the
cases that have been published on transmigration, updating the main aspects of
this pathology.
Key words: Lower canine impaction, dental migration, transmigration of lower canine.
RESUMEN
La retención, es decir, la no erupción de un
diente permanente más allá de un año después de la edad normal de erupción,
es relativamente poco frecuente si exceptuamos el caso de los terceros molares y
los caninos superiores. La transmigración se define como el fenómeno en el
cual un diente incluido no erupcionado traspasa en más de la mitad de su
longitud la línea media.
Exponemos el caso clínico de una paciente de 20 años de edad, que presentaba
la transmigración del canino inferior izquierdo, con un patrón de migración
tipo 4 de Mupparapu. De igual forma, realizamos una revisión bibliográfica de
los casos publicados de transmigración, actualizando los principales aspectos
de esta patología.
Palabras clave: Impactación de canino inferior; migración dentaria, transmigración de canino inferior.
Introduction
Retention is defined as a tooth which is unerupted more than a year after the normal age of eruption, and is a relatively rare event, except in the case of the third molars and the upper canines. When the tooth crosses the midline, this is known as dental transmigration. (1).
Although there have been references to this type of impaction since the second half of the last century, (2) the definition of this relatively rare anomaly in dental eruption was not standardised until some time after the first cases were reported. Several terms have been used, such as anomalous (3), malpositioned (4) or displaced (5) tooth., although the first to use the more widely accepted term, transmigration (and thus, transmigrated tooth) was Ando et al in 1964 (6). Tarsitano defined it as the phenomenon of an unerupted mandibular canine crossing the midline (7) and Javid (1) later stated that the midline had to be crossed by half of the tooth.
The purpose of this article is to report a clinical case of transmigration and to perform a literature review of those cases that have been reported, in order to present, in as true a light as possible, the epidemiological characteristics of this anomaly.
Clinical Case
We present the case of a twenty-year-old patient, referred by his orthodontist to the Faculty of Dentistry, Seville. Given the incorrect position of the lower left canine (impacted horizontally), the diciduous canine was used as a permanent tooth by the orthodontist during treatment, since he considered the rescue of the tooth to be inappropriate. He informed the patient of the existence of the dental impaction and the need for its extraction, or at least, observation.
Upon radiological examination (orthopantomograph), we observed the lower left canine to be in a position of horizontal impaction below the apices of the lower contralateral premolars and canines (type 4 of Mupparapu pattern of transmigration (8)) (Figure 1). Given the evidence for the transmigration of the canine, we established that the tooth should be extracted. If we were to continue monitoring the case, in the event of the impacted tooth nearing the mental foramen, the risks of intervention would be unnecessarily increased. Furthermore, with complete clinical certainty, irritation would be caused by the impacted tooth to the lower dental nerve (9,10).
The tooth was extracted by means of a partial Neumann incision, with removal at the left lateral incisor level. The tooth was not removed in the fourth quadrant due to the proximity of the mental foramen, with the right mental nerve being identified and protected during the intervention. The tooth was extracted by coronal osteotomy and two dental sections, and the pericoronal sack was also eliminated (Figure 2).
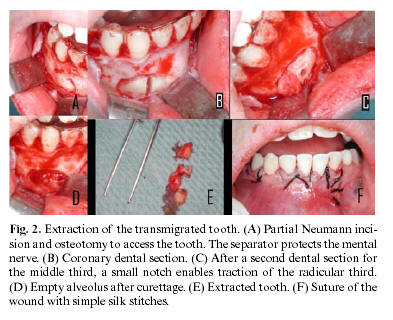
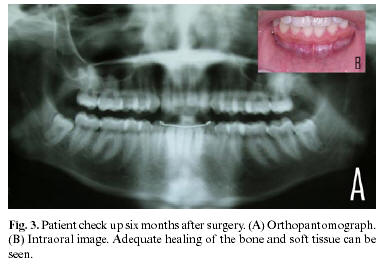
Finally, the wound was sutured and analgesic, anti-inflammatory (Ibuprofen 600 mg, 1 tablet / 8 hours for one week) and antibiotic (Amoxicillin 875 mg / Clavulanic acid 125 mg, 1 tablet / 8 hours for a week) medication was prescribed during the postoperative period, which was without incident. The stitches were removed after ten days. Progress was favourable and no complications were detected (Figure 3).
Discussion
Transmigration is an extremely rare anomaly. If we consider that the impaction of the lower canine occurs 20 times less than the upper canine and assuming that Javids reports, in which a survey of 1,000 students revealed only one transmigration, are correct, (1), we get some idea of how rare this condition is.
The presence of transmigration must be suspected, if the lower canine is absent from the arch, if the canine has not erupted more than a year after the normal age of eruption and if there is deviation from the midline. In some cases, agenesis of the lateral incisors and lower premolars has been detected (6).
The cause of such rare behaviour is not yet known and there are many hypotheses surrounding it. Bruzst believes that the canine germ is situated in front of the lower incisors and that facial growth pushes it towards the contralateral side (10), while other authors believe that an abnormally strong eruption force or a change which affects the crypt of the tooth germ might lead to erroneous eruption (11). Other factors favouring the appearance of this anomaly are: premature loss of deciduous teeth, osteodental discrepancy, agenesis of the lower lateral incisors, endocrinopathy and hereditary factors, traumas and odontomas (6).
Although the impacted transmigrated canine does not normally erupt, in some bibliographical reviews, it has been pointed out that in approximately 5% of cases, this does occur. Likewise, bilateral transmigration occurs in approximately 12% of cases (12).
Although the number of transmigrated canines is normally higher in women than in men, with a ratio of 2:1, according to other, broader reviews, this difference is not so great (12). Patients presenting transmigration range between the ages of 8 to 62 years old. This is in agreement with other authors opinions, who state that migration begins at an early age, between 6 and 8 years old, before root formation is complete (12).
Clinically, transmigration can be, and usually is symptomless. Although the first published cases were detected as a result of neurological changes caused by the compression of the lower dental nerve by the impacted tooth (10), radiology has made it possible to detect other similar, but symptomless, cases, allowing an adequate assessment of the percentage of cases which are presented clinically.
The presence of pathological conditions with transmigration must also be mentioned. The most frequent of these conditions are the presence of dentigerous cysts, odontomas and the appearance of other impactions (12).
Transmigration, that is, the migration of impacted teeth which cross the midline, has classically affected mandibular canines. As a result, it has been speculated and almost taken as fact, that it does not affect any other dental group (8). However, cases of transmigration in maxillary canines have been detected (11,13).
From the data published, it is possible to define various behavioural patterns of the transmigrated mandibular canines. In particular, Mupparapu described five patterns (8). Pattern 4 corresponds to our case (canine impacted horizontally below the apices of the contralateral canine and premolars). Type 1 is a canine which is in a mesioangular position below the front teeth with its corona crossing the midline. Type 2 is similar to type 4 except that the canine is located below the apices of the lower incisors. Type 3 is an erupted canine caused by the contralateral canine moving mesially or distally. Finally, type 5 is a canine in a vertical position coinciding with the midline (8).
Mupparapus type 1, followed by type 2, is the most frequently occurring pattern. Type 4 and 3 occur less frequently, while type 5 is the least frequent (8).
With respect to the treatment of these canines, ideally, interceptive treatment should be carried out, although it is extremely difficult, if not impossible, to predict the appearance of this anomaly. There is often a difference of a couple of years between a normal orthopantomograph and another in which transmigration of the canine is established. For Joshi, predicting the appearance of the profile depends on the inclination that the canine tooth germ presents. If the angle formed by the mid-sagittal plane and the dental axis exceeds 50º, transmigration is predictable; if an angle between 30º-50º is formed, it is possible that transmigration will develop, and transmigration is unlikely if it does not exceed 30º (14).
For interception, it is best to detect patients presenting characteristics which are most related to transmigration when they are between 8 and 9 years old, and these patients should undergo a clinical radiology examination so that action can be taken quickly. (14). This ensures a significantly greater number of treatment options, the most suitable being rescue surgery by way of surgical repositioning, autotransplantation or surgical/orthodontic treatment, assessing the individual characteristics of the patient, location and inclination of the tooth (3).
Once transmigration is established, it is difficult to carry out rescue surgery or orthodontic repositioning (if the tooth has erupted) although this possibility should not be ruled out. However, in such situations, extracting the impacted tooth is the most favoured treatment. Although the tooth is extracted on the contralateral side to the transmigrated canine, the tooth maintains its nervous innervation on the side that the germ is formed. This must be taken into account if the tooth is extracted under local anaesthesia (9).
One last treatment option in these patients is observation and clinical check ups, with radiographs taken periodically. In patients under 14 years old, before extracting the tooth, other options should be considered and the case should be carefully assessed. In patients over 14 years old, significant changes are not expected and extraction should only be considered if the patient rejects surgical treatment (6).
In the case in question, given the location of the canine, the orthodontist felt it to be more prudent to complete orthodontic treatment using a deciduous canine as a permanent tooth, and given that the canine apices were closed, to advise against transplantation and suggest extraction. The patient was informed of all the aspects of his treatment, and of the possibility of premature loss of the deciduous canine, which would have to be covered with an osseointegrated implant in the said position.
![]() Correspondence
Correspondence
Dr. Daniel Torres Lagares
C/ Sta Mª Valverde 2 3ºC;
41008 Sevilla
E-mail: danieltl@us.es
Received: 1-05-2005
Accepted: 16-11-2005
References
1. Javid B. Transmigration of impacted mandibular cuspids. Int J Oral Surg 1985;14:547-9. [ Links ]
2. Bluestone LI. The impacted mandibular bicuspid and canine: indications for removal and surgical considerations. Dent Items Interest 1951;73:341-55. [ Links ]
3. Howard RD. The anomalous mandibular canine. Br J Orthod 1976;3:117-21. [ Links ]
4. Broadway RT. A misplaced mandibular permanent canine. Br Dent J 1987;163:357-8. [ Links ]
5. Mitchell L. Displacement of a mandibular canine following fracture of the mandible. Br Dent J 1993;174:417-8. [ Links ]
6. Ando S, Aizaea K, Nakashima T, Sanka Y, Shimbo K, Kiyokawa K. Transmigration process of impacted mandibular cuspid. J Nihon Univ Sch Dent 1964;6:66-71. [ Links ]
7. Tarsitano JJ, Wooten JW, Burditt JT. Transmigration of nonerupted mandibular canines: report of cases. J Am Dent Assoc 1971;82:1395-7. [ Links ]
8. Mupparapu M. Patterns of intra-osseous transmigration and ectopic eruption of mandibular canines: review of literature and report of nine additional cases. Dentomaxillofac Radiol 2002;31:355-60. [ Links ]
9. Caldwell JB. Neurological anomaly associated with extreme malposition of a mandibular canine. J Oral Surg (Chic) 1955;8:484-7. [ Links ]
10. Bruszt P. Neurological anomaly associated with extreme malposition of a mandibular canine. J Oral Surg (Chic) 1958;11:89-90. [ Links ]
11. Shapira Y, Kuftinec MM. Unusual intraosseous transmigration of a palatally impacted canine. Am J Orthod Denofacial Orthop 2005; 127:360-3. [ Links ]
12. Camilleri S, Scerri E. Transmigration of mandibular canines - a review of the literature and a report of five cases. Angle Orthod 2003;73:753-62. [ Links ]
13. Aydin U, Yilmaz HH. Transmigration of impacted canines. Dentomaxillofac Radiol 2003;32:198-200. [ Links ]
14. Joshi MR. Transmigrant mandibular canines: a record of 28 cases and a retrospective review of the literature. Angle Orthod 2001;71:12-22. [ Links ]

