










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Access to primary care and social determinants of health (SDoH) have a large influence on clinical care and patient outcomes.1 According to the United States (US) Department of Health and Human Services data, in 2017 less than half of the nation's primary care needs had been met.2 Despite an increase in the number of programs encouraging physicians to work with medically underserved communities, there remains a shortage of primary care medical providers, particularly in rural communities and communities of racial and ethnic minority groups.3,4 Clinical pharmacists working within medically underserved communities in the US can help fill gaps in care among these vulnerable populations.5
Training, education, and work satisfaction are all key factors to increasing the number of providers in underserved communities.6-8 Almost 50% of medical residents in family medicine will end up practicing within 50 miles of their location of training.6 Likewise, exposure to underserved populations during the experiential portion of a pharmacy school curriculum results in more positive views of underserved populations.7 Furthermore, practitioners in underserved areas have historically reported high satisfaction with their positions. A survey of primary care providers showed that practitioners working in underserved communities were more likely to cite their personal mission and self-identity/background as motivators in their employment decision than practitioners not working in underserved areas.8
Currently, pharmacists and pharmacy advocacy groups are seeking provider status for pharmacists providing services for Medically Underserved Areas (MUA), Medically Underserved Populations (MUP), or Health Professional Shortage Areas (HPSA). In an effort to recruit and retain clinical pharmacists in underserved areas, it is prudent to gather data on the existing pharmacist workforce. This will help identify strategic interventions which may draw in a larger workforce to assist in bridging health disparities and further advance the pursuit of pharmacist provider status. What has yet to be described is the clinical pharmacy workforce among medically underserved areas. This survey aimed to identify characteristics of ambulatory care pharmacists that pursue and maintain employment within underserved areas.
METHODS
An original survey was created using Qualtrics® survey software and distributed in the English language within the United States from April 2019 through June 2019 to members of the following online listservs: American College of Clinical Pharmacy (ACCP) Ambulatory Care Practice and Research Network (PRN), American Society of Health-System Pharmacists (ASHP) Section of Ambulatory Care Practitioners, select members of American Pharmacists Association Academy of Pharmacy Practice and Management (APhA-APPM) Care of Underserved Patients Special Interest Group, and an informal listserv of clinical pharmacists self-identified to be practicing in underserved settings. Clinical pharmacists practicing in ambulatory care settings within medically underserved areas were invited to complete the survey.
A clinical pharmacist was defined as a pharmacist who spends a majority (≥50%) of his or her time in non-dispensing roles and, per the ACCP definition of a clinical pharmacist, provides patient care that optimizes medication therapy, promotes health, and disease prevention.9 Survey respondents meeting the definition of a clinical pharmacist were included in data analyses if they attested to providing care in a United States Health Resources and Services Administration (HRSA) designated MUA, MUP, or HPSA. Respondents were excluded if they had been employed in an underserved area for less than 3 months at the time of survey completion.
Survey respondents were asked questions related to demographic information, education and training, employment history, practice site, funding model of current position, exposure to underserved populations during pharmacy school or post-graduate training, first and primary language, reason for pursuing current job, and job satisfaction. When identifying a reason for pursuing and maintaining their current job, respondents were asked to narrow down and choose only their top motivating factor. Respondent characteristics were analyzed using descriptive statistics. This study was reviewed and approved by the Colorado Multiple Institutional Review Board (IRB).
RESULTS
The exact response rate of our survey is unknown, as there is no credible database that identifies the number of ambulatory care pharmacists working in underserved settings. Currently, HRSA only collects information on primary care, dental, and mental health providers in MUPs, MUAs, and HPSAs. In total, 111 surveys were included in data analysis. A majority of respondents were White, non-Hispanic, female, 30-39 years of age, with English as their only spoken language. Respondents included representation from all regions of the US. Approximately 75% of respondents had completed one or two years of residency training, and over 65% of pharmacists were board certified. A majority (~68%) of pharmacists completed some form of clinical experience or specialized training focused on underserved care prior to their position. More than two-thirds (68%) of respondents had a faculty appointment (adjunct/adjoint or full-time), with about 94% serving as an experiential preceptor for pharmacy or medical trainees. Funding for clinical pharmacist positions was mixed with almost half of pharmacists funded by two or more entities. The top funding sources reported were from a clinical practice site (~64%), a university or school of pharmacy (~46%), a grant (~19%), or an accountable care organization (~15%). See Table 1 for more details.
Table 1. Demographics of survey respondents
| Characteristic | Number (%) |
|---|---|
| Age Group (n=106) | |
| 20-29 years | 26 (24.5) |
| 30-39 years | 55 (51.9) |
| 40-49 years | 18 (17) |
| 50+ years | 7 (6.6) |
| Race: White/Caucasian (n=111) | 93 (83.8) |
| Ethnicity: Hispanic/Latino (n=106) | 8 (7.5) |
| Gender: Female (n=107) | 82 (76.6) |
| Language: Bilingual (n=110) | 35 (31.8) |
| 2nd language Spanish (n=35) | 21 (60) |
| Region of US (n=111) | |
| Midwest | 31 (27.9) |
| Northeast | 6 (5.4) |
| South | 32 (28.8) |
| West | 42 (37.8) |
| PGY1 Training: Yes (n=111) | 83 (74.8) |
| Community (n=83) | 23 (27.7) |
| Pharmacy practice (n=83) | 60 (72.3) |
| PGY2 Training: Yes (n=111) | 55 (49.5) |
| In ambulatory care (n=55) | 46 (83.6) |
| Fellowship Training: Yes (n=111) | 4 (3.6) |
| Board Certification: Yes (n=111) | 76 (68.5) |
| BCPS (n=76) | 24 (31.6) |
| BCACP (n=76) | 60 (78.9) |
| Exposure to Underserved Setting (n=111) | |
| During pharmacy school | 51 (45.9) |
| During PGY1 training | 48 (43.2) |
| During PGY2 training | 26 (23.4) |
| During fellowship | 2 (1.8) |
| Informal training | 11 (9.9) |
| Volunteer work | 25 (22.5) |
| Type of Underserved Setting (n=111) | |
| FQHC/Community health center | 63 (56.8) |
| Ambulatory clinic affiliated with safety-net hospital | 23 (20.7) |
| Private practice clinic in an underserved area | 7 (6.3) |
| Faith-based low-income clinic | 5 (4.5) |
| Other | 13 (11.7) |
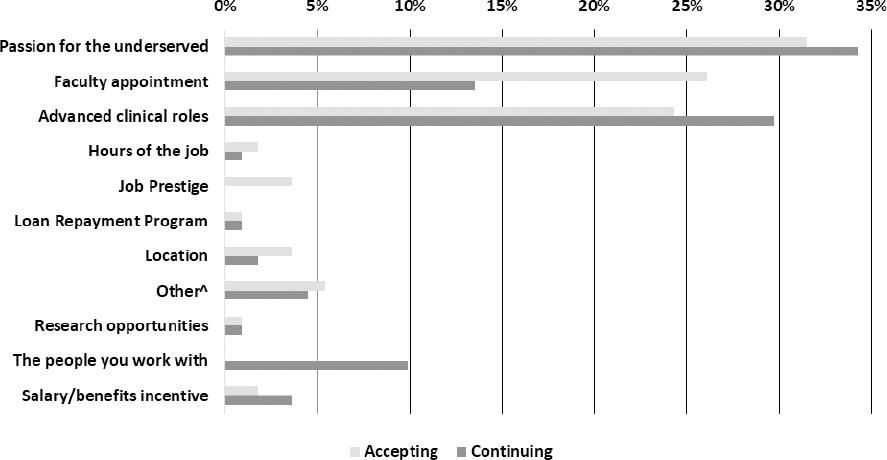
Most pharmacists (~81%) reported practicing under collaborative practice agreements, protocols, or prescriptive authority to manage chronic disease states at their sites. The top three motivators for pharmacists accepting their clinical position in order of frequency were passion for caring for underserved populations, the presence of a faculty appointment, or the freedom and flexibility of advanced clinical roles. When looking at motivators for staying at their current position, passion for underserved settings remained at the top of the list. However, presence of a faculty appointment became less important, whereas advanced clinical roles became more important. Presence of a loan repayment incentive and research opportunities did not appear to be important in a pharmacist's decision making to initially accept their job nor to maintain their employment in underserved care (Figure 1).
DISCUSSION
A 2019 National Pharmacist Workforce Study showed a promising trend in racial diversity among the pharmacy profession, with increases in both Asian and Black pharmacists in the last ten years.10 Workforce diversity is important for a number of reasons. It has been consistently documented that White patients receive better quality of care and have higher access to care than minority patients.4 In addition, patients who are in minority racial and ethnic groups have disproportionately higher rates of chronic diseases, including but not limited to heart disease and diabetes, compared to White patients.11 Furthermore, previous studies have shown that patients are more likely to seek care, have improved medication adherence, and have higher satisfaction with their care when there is patient-provider race, ethnicity, or language-concordance.12-14 The respondents in this study were 83.8% White, a percentage that is slightly higher than the national 78.2% statistic.11 Thus, there remains a large opportunity to increase diversity in the clinical pharmacy ambulatory care workforce caring for underserved populations. Clinical pharmacists in underserved settings have an opportunity to strengthen the quality of their impact by pursuing skill sets that enhance their cultural competency and sensitivity. Clinical practice sites can further improve this impact by recruiting and maintaining a diverse workforce of pharmacists to meet the needs of diverse patient populations. Another interesting finding in this study was that the majority of survey respondents (76.6%) identified as female, which is slightly higher than the national percentage of women pharmacists at 61.8%.11 Therefore, our data might indicate that female pharmacists are more likely to pursue jobs with underserved populations than male pharmacists.
Within underserved settings, clinical pharmacists have historically reported practicing at the top of their license in an attempt to bridge health disparities where there is a shortage of medical providers.15 A large majority of respondents in this study reported utilizing collaborative practice agreements, protocols, or prescriptive authority to provide patient care, which allows for a higher level of clinical pharmacist independence. Unsurprisingly, our findings indicate that these advanced clinical roles are one of the top motivators for pursuing and maintaining positions in underserved settings. This aspect of the pharmacist's role could be popular due to the national increase in residency training and desire for pharmacists to use their additional clinical skill sets on a daily basis. Respondents also noted their personal passion for underserved care as the top motivator for pursuing and maintaining employment. This passion could have been developed during early exposure to underserved settings, as our results showed a correlation between early experiential or specialized training in underserved care and pharmacists pursuing employment in these areas. Furthermore, teaching opportunities appear to be an appealing aspect for pharmacists in accepting and maintaining positions in underserved settings. This may shed light on a potential avenue for underserved practice sites to create long-standing partnerships with colleges of pharmacy to recruit and maintain quality candidates who could serve as preceptors for trainees. These types of partnerships have a two-fold potential as they could also serve as the catalyst for increasing learner exposure to underserved settings.
This is the first manuscript to date that has reported characteristics for ambulatory care clinical pharmacists in underserved settings. In addition, our data includes representation from all geographic regions of the United States, albeit a smaller proportion from the Northeast region. This finding is consistent with the fact that Northeast states have been shown to have the highest physician surplus, which may indicate a lower demand and employment of clinical pharmacists in this region.16 There were a few limitations to this research study. This survey asked pharmacists to think back and attempt to remember their rationale for accepting their current position. Since this survey included individuals who had been in practice anywhere from 3 months to 53 years, the amount of time elapsed between Day 1 of job and current time is different for all subjects. Thus, there is a potential for recall bias that could have skewed results. In addition, the inability to calculate a response rate limits the ability to ensure reported results are truly reflective of all ambulatory care clinical pharmacists in underserved settings.
CONCLUSIONS
With a large majority of our respondents identifying as White and unilingual, there remains a large opportunity to increase diversity in the clinical pharmacy ambulatory care workforce caring for underserved populations. There is an observed correlation between early experiential or specialized training in underserved care and pharmacists pursuing employment in these areas. Thus, one potential long-term strategy to diversify and grow the ambulatory care clinical pharmacist workforce in underserved settings is for clinical practice sites to partner with colleges of pharmacy to recruit and maintain quality individuals who can meet the needs of diverse patient populations as well as expand student and resident training opportunities in underserved settings.

