










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkArchivos Españoles de Urología (Ed. impresa)
versión impresa ISSN 0004-0614
Arch. Esp. Urol. vol.62 no.3 abr. 2009
Testicular metastasis as first clinical expression of unknown origin malignant melanoma
Metástasis testicular como primera manifestación clínica de melanoma maligno de origen desconocido
José Antonio Contreras Ibañez, Pedro Muriel Cueto1 and José María Baez Perea1
Medical Oncology Department and Pathologic Antomy Department1. Puerta del Mar Universitary Hospital. Cádiz. Spain.
SUMMARY
Objective: To report a rare process and to stimulate clinicians and pathologists to have this possibility present in their diagnoses.
Methods: We report the case of an adult male with pain and swelling in the left inguinal region and increased volume of the homolateral testicle.
Conclusion: It is appropriate to bear in mind the possibility of testicular metastasis of a primary unknown tumor in adult males since metastatic affectation can constitute the first manifestation of the disease.
Key words: Testicle. Metastases. Malignant melanoma.
RESUMEN
Objetivo: Aportar información sobre un raro proceso y alentar a clínicos y patólogos para que tengan presente en sus diagnósticos esa posibilidad.
Métodos: Presentamos el caso de un varón adulto con dolor y tumefacción en región inguinal izquierda y aumento de volumen del testículo homolateral.
Conclusiones: Es conveniente en varones adultos tener presente la posibilidad de metástasis testicular de un tumor primario oculto ya que la afectación metastásica puede constituir la primera manifestación de la enfermedad.
Palabras clave: Testículo. Metástasis. Melanoma maligno.
Introduction
Testicular metastases of malignant melanoma are relatively common in autopsy series, but are very rarely diagnosed in living patients (1). It is even more rare to find them as the first manifestation of disease and even more so to fail to discover the primary malignant melanoma.
There are cases in which the history of melanoma is remote and unrelated to the current testicular process. Furthermore, if this is added to the varied histological appearance of metastatic melanoma, it is not difficult to understand that the pathological diagnosis is underestimated in the orchiectomy specimen, diagnosing primary testicular tumor. In other cases, testicular metastasis is the first manifestation of the disease, with no further evidence of spread, making diagnosis even more difficult.
The objective of this paper is to encourage clinicians and pathologists to consider this possibility when a testicular mass is found in an older man, even when the presence of a primary tumor is unknown.
Case report
61-year old patient, smoker of 20 cigarettes/day, diagnosed several years earlier with chronic atrial fibrillation, HBP and chronic airway obstruction, with a right knee replacement and receiving treatment with dicumarinic, antihypertensive and bronchodilator agents.
He visited the emergency room of the Centre at the end of November 2006 with pain and swelling in the left inguinal region, 12 days of evolution, together with increased volume of the homolateral testicle. He was assessed by the urologist on duty who, in the physical examination and ultrasound scan (27/11/06), detected alarge solid 60 x 58 mm mass with necrotic areas, located in the left testis; there was another large 71 x 55 mm mass in the left inguinal region, heterogeneous, well delimited and hypoecogenic, compatible with adenopathy. Suspecting a primitive testicular tumor, alphafetoprotein and B-HCG were requested (normal) and an inguinal orchiectomy was scheduled, being performed on 21/12/2006.
Anatomical pathology reported: adenopathy sections and testicle with tumor with abundant ochre pigment and nodule-forming theca-like cells with irregular nuclei, gross nucleolus and increased mitotic index. The tumor respects the periphery of the testis and albuginea and massively infiltrates the adenopathy. The immunohistochemical study is positive for S-100 and HMB-45 and negative for alpha-inhibin (Figure 1)
He was referred to Dermatology to search for the primary melanoma, without success, so he was referred to our department for an evaluation of systemic treatment.
His examination in our department was anodyne.
We requested a TAC scan of the chest and abdomen with oral and intravenous contrast: non-calcified, 6 mm nodule on left segment I and 12 mm nodule on right segment 6 with pleural tail. In the upper lumbar region, a 3.1 cm nodule with soft tissue density was found with peripheral uptake and increased attenuation of local fat. 17 mm left inguinal adenopathy with uptake.
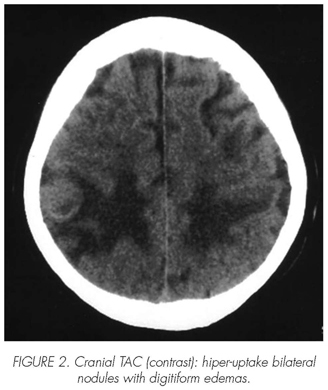
After obtaining his informed consent, we were about to apply the first cycle of systemic treatment with Dacarbazine (DTIC), but a few days before the scheduled date, he was admitted with convulsions, with the cranial TAC scan (Figure 2) revealing multiple parenchymatous, hyper-uptake bilateral nodules, with digitiform edemas, predominantly located in the frontoparietal and right parietal regions, the largest measuring 2 cm.
He received three sessions of palliative holocranial irradiation, with the symptoms improving.
We have started palliative monochemotherapy with DTIC, having administered two cycles to date, which he has tolerated without remarkable incidents. He is also receiving corticoid therapy and anticonvulsant treatment.
Discussion
- Testicular metastases are uncommon and around 15% of all cases derive from a malignant melanoma (MM). Around 30 cases had been described by 2006, most of them as post mortem findings. Only in four cases did testicular metastasis represent the first manifestation of the disease (2).
- Testicular metastases of any histological type without prior diagnosis of the primary tumor are rare and have been reported as isolated cases (3-7). Only exceptionally is the primary tumor a melanoma (8).
- In our case, the diagnosis was made while the patient was alive. It was the first clinical manifestation of the disease and the most remarkable point is that the location of the primary melanoma was unknown.
- Where most testicular metastases have been found in autopsy series have been at the Memorial Hospital and M. D. Anderson. The former identified 8 cases in 100 autopsies performed on patients with metastatic melanoma, and they all formed part of a widespread disease (9). The latter found only 2 cases in 72 autopsies performed on patients with metastatic melanoma at genitourinary locations, and none of them had been clinically recognised (10).
- Metastatic spread to the testicle can occur through several routes: retrograde venous extension, retrograde lymphatic extension and arterial embolism. On the other hand, on some occasions the primary tumor has regressed and is only manifest in the metastasis, as in the case presented here.
- The primary locations most commonly giving rise to testicular metastases are carcinoma of the prostate, lung, kidney, colon and stomach.
- The important practical aspect under discussion is the differential diagnosis with primitive and metastatic tumors of the testicle and even benign processes (hydrocele, varicocele), in order to establish a correct approach and therapeutic plan. Obviously, a microscopic evaluation is essential for establishing a diagnosis of testicular metastasis of melanoma, especially considering that the clinical history of disease is often lacking and the primary melanoma could have regressed, which could have occurred in this case.
- In our case, the anatomopathological characteristics were typical and there were no doubts over the diagnosis.
- In general lines, the specific prognosis of testicular metastases is unclear. In our case, it was the first manifestation of the disease, although it was soon followed by other visceral metastasis sites. We therefore believe that the testicular metastasis in this case does not represent a worse prognosis.
- The treatment of the testicular metastasis will largely depend on the patient's life expectancy. In this case, as the primary tumor was unknown, the surgeon decided on an inguinal orchiectomy. This procedure could also be applied in cases when the primary location is known, in order to eliminate potential local-regional complications derived from the neoplastic testicular involvement. The patient was also treated with holocranial irradiation and monochemotherapy with DTIC, in view of possibly compromised cerebral and systemic sites. Polychemotherapy does not improve survival relative to DTIC alone.
Conclusion
Testicular metastases are rare and largely discovered incidentally in autopsies or therapeutic orchiectomies. They are derived from primary carcinomata of the prostate, lung, gastrointestinal tract, kidney or melanomas. Only exceptionally do they represent the first manifestation of the disease and their specific prognosis is unknown. Histologically, they present distinctive characteristics and should be considered in the differential diagnosis of testicular masses, especially in older men.
 Correspondence:
Correspondence:
José Antonio Contreras Ibañez
Hospital Universitario Puerta del Mar
Servicio Oncologia Médica (9a planta)
Avda. Ana de Viya 21.
11009 Cádiz. (Spain).
joseantonio.contrerasibaez@gmail.com
Accepted for publication: February, 25th 2008.
References and recomended readings (*of special interest, **of outstanding interest)
*1. Tiltman AJ. Metastatic tumors in the testis. Histopathology 1979; 3: 31-37. [ Links ]
2. Bothing R, Rogosch KU, Mach P et al. Aktuelle Urol 2006; 37(2): 138-140. [ Links ]
3. Meacham RB, Mata JA, Espada R et al. Testicular metastases as first manifestation of colon carcinoma. J Urol 1988; 140: 621-622. [ Links ]
4. Zur RJ, Trotter SE, Baithun SI. Krukemberg tumor of the testis. Histopathology 1989; 14: 214-216. [ Links ]
5. Muir GH, Fisher C. Gastric carcinoma presenting with testicular metastasis. Br J Urol 1994; 73: 713-714. [ Links ]
**6. Blasco de Villalonga M, Llarena RI, Acha MP et al. Testicular metastases of renal adenocarcinoma. Report of a case. Arch Esp Urol 1994; 47: 281-282. [ Links ]
*7. Lauro S, Lanceta G, Brisa E et al. Contralateral solitary testis metastases antedating renal cell carcinoma: A case report and review. Anticancer Res 1998; 18: 4683-4684. [ Links ]
**8. Richardson PGG, Millward MJ, Shromankar JJ et al. Metastatic melanoma to the testis simulating primary seminoma. Br J Urol 1992; 69: 663-665. [ Links ]
*9. Gupta TD, Grabstaald H. Melanoma of the genitourinary tract. J Urol 1965; 93: 607-614. [ Links ]
10. Macdonald EJ. The epidemiology of melanoma. Ann NY Acad Sci 1963; 100: 4-17. [ Links ]

