










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkArchivos Españoles de Urología (Ed. impresa)
versión impresa ISSN 0004-0614
Arch. Esp. Urol. vol.62 no.5 jun. 2009
Prostatic specific antigen (PSA), pro-inflammatory cytokines, and prostatic pathology (Benign prostatic hyperplasia and cancer). Relationship with malignancy
Antígeno prostático-específico, citoquinas pro-inflamatorias y patología prostática (Hiperplasia benigna y Cáncer). Relación con la malignidad
José Ramón Cansino Alcaide1, Raul Vera San Martin2, Fermín Rodríguez de Bethencourt Codes1, Yosra Bouraoui2,3, Gonzalo Rodríguez Berriguete2, Ridha Oueslati3, Javier De la Peña Barthel1, Ricardo Paniagua Gómez-Álvarez2 and Mar Royuela Garcia2.
1Urology Departament. Hospital La Paz. Madrid. Spain.
2Departamento Biología Celular y Genética. Universidad de Alcalá. Alcalá de Henares. Madrid. Spain.
3Unité d'Immunologie Microbiologie Environnementale et Cancérogenése á la Faculté des Science de Bizerte. Túnez.
Grants from the "Ministerio de Educación y Ciencia" (SAF2007-61928) and the "Programa de Cooperación Interuniversitaria e Investigación Científica (PCI-Mediterráneo) (A/011430/07)" (Spain).
SUMMARY
Objectives: Cancer is a complex process in which cytokines play an important role. Cytokines are low-molecular weight soluble proteins involved in cellular transmission signals and several disorders. Pro-inflammatory cytokines (IL-1, TNFa- and IL-6) are involved in prostate cancer development. The aim of this study was to relate the expression (analyzed by Western blot and immuno-histochemistry) of several pro-inflammatory cytokines (IL-1, TNF-a and IL-6) with serum levels of prostate-specific antigen (PSA) in normal (no pathological samples) as pathological samples (hyperplasia and cancer), in order to elucidate their possible role in tumor progression. We are also discussing the possible use of these cytokines as a potential therapeutic target.
Methods: This study was carried out in 5 normal, 25 benign prostatic hyperplastic (BPH) and 17 prostate cancer (PC) human prostates. Immunohistochemical and Western blot analysis were performed. Serum levels of PSA were assayed by a PSA DPC immulite assays (Diagnostics Products Corporation, Los Angeles, CA)
Results: In BPH, IL-1a, IL-6 and TNF-a were only expressed in patients with PSA serum levels of 0-4 ng/ml or 4-20 ng/ml, but not in the group >20 ng/ml. In PC these cytokines were only expressed in patients with PSA serum levels >4 ng/ml, although the expression of these cytokines was elevated when PSA levels were >20 ng/ml.
Conclusions: In PC there might be an association between high expression of pro-inflammatory cytokines (IL-1, TNFa and IL-6), elevated serum levels of PSA and cancer progression. A better understanding of the biologic mechanism of this association may improve the finding of new targets for therapy in these patients.
Key words: TNFa. IL-1. IL-6. PSA. Prostate cancer.
RESUMEN
Objetivo: El cáncer es un proceso complejo en el cual las citoquinas juegan un importante papel. Las citoquinas son proteínas solubles de bajo peso molecular, que participan en la transmisión celular y en diferentes patologías. Las citoquinas pro-inflamatorias (IL-1, TNF-a e IL-6) están muy relacionadas con el desarrollo del cáncer de próstata. El objetivo de nuestro trabajo consistió en relacionar la expresión (mediante inmunocitoquímica y Western blot) de diferentes citoquinas pro-inflamatorias (IL-1, TNF-a e IL-6) con los niveles de antígeno prostático específico (PSA) en suero, tanto en pacientes normales (sin patología prostática) como en condiciones patológicas (hiperplasia y cáncer), así como su posible papel en la progresión tumoral. Se discutirá el posible uso de estas citoquinas como diana terapéutica.
Métodos: Este estudio se ha realizado en 5 pacientes normales, 25 pacientes diagnosticados de hiperplasia benigna de próstata (HBP) y 17 pacientes de cáncer (CP). Se han realizado análisis de Western blot e inmunocitoquímica. Los niveles séricos de PSA se midieron mediante un "PSA DPC immulite assays" (Diagnostics Products Corporation, Los Angeles, CA).
Resultados: En HBP, IL-1a, IL-6 y TNF-a, solo se expresan en pacientes con niveles séricos de PSA de 0-4 ng/ml ó 4-20 ng/ml, pero no en el grupo >20 ng/ml. En cáncer, estas citoquinas se expresan en pacientes con niveles séricos de PSA >4 ng/ml, aunque la expresión de estas citoquinas se eleva considerablemente cuando los niveles de PSA son >20 ng/ml.
Conclusiones: En cáncer, podría existir una asociación entre elevada expresión de citoquinas pro-inflamatorias (IL-1, TNF-a e IL-6), elevados niveles séricos de PSA y progresión del cáncer. Un mejor conocimiento de los mecanismos biológicos de esta asociación, podrían ayudarnos a encontrar una posible diana terapéutica para los pacientes con patología prostática.
Palabras clave: TNFa. IL-1. IL-6. PSA. Cáncer de próstata.
Introduction
IL-1 family includes two bioactive ligands (IL-1a and IL-1b) (1), two types of transmembrane receptors (IL-1RI and IL-1RII) (2) and a specific receptor antagonist (IL-1Ra). The affinity of IL-1a, IL-1b and IL-1Ra to receptors IL-1RI and IL-1RII differs depending of the ligand. IL-1a and IL-1Ra present higher affinity to IL-1RI than IL-1b , while IL-1b displays higher affinity to IL-1RII (3). The expression of IL-1 family has been reported in several tumors such as prostate cancer where Ricote et al. (4) propos that IL-1 family may be involved in cell proliferation since immunoexpression of IL-1a and IL-1Ra was a characteristic feature of PC compared with normal prostate samples and BPH.
TNF-a has been proposed as tumoral promoter (5). Different studies relate TNF-a endogenous production with tumour invasion and development of metastasis (6, 7). In cancer prostate have been related the serum levels of TNF-a to the development of the disease, associating the serum levels of TNF-a, the disease development and presence of metastasis (8). The functional duality of TNF-a in tumour tissues is determined by the intracellular signs that contributed your arrival to the cellular surface and binding your membrane receptors (TNFRI and TNFRII) and to activate different transduction pathway. The expression and action of TNF-a and its receptors has been reported in several tumours such as esophageal (9), prostate (10), follicular thyroid (11), skin (12), ovarian (13) and breast (14) cancers.
Interleukin-6 (IL-6) is a multifunctional cytokine produced by several normal cell types including T lymphocytes, fibroblasts, or monocytes. This cytokine exerts its effects throughout a membrane receptor complex composed by IL-6 receptor a (IL-6Ra) and glycoprotein 130 (gp130). First, IL-6 binds to IL-6Ra, which is unable to initiate signal transduction, and this complex attracts gp130 molecules, which dimerize leading to the intracellular signal (15). In addition to an immunological role, IL-6 is involved in cell proliferation in other tissues such as bone (16), testis (spermatogenesis) (17), skin (18) and nervous system (19). It has been shown that IL-6 also stimulates the development of many tumors, including melanoma, renal cell carcinoma, ovarian carcinoma, lymphoma breast carcinoma (20) or prostate carcinoma (21).
At the present, several researches are focusing in the search for new biochemical markers capable of predicting prostate cancer and prognosis. In addition, pro-inflammatory cytokines was related to the production of PSA and progression of prostate cancer (26-28).
PSA is a marker organ-specific, with high sensibility but low specificity for the detection of cancer prostate, existing situations that provoke a temporary increase of your levels not related to tumour processes such as manipulations of the prostate gland (rectal tact or biopsies) (23) and benign diseases (hyperplasia) (24). In addition, normal levels have been observed in patients with tumour pathology. In this way, PSA is not indicative of the evolution grade of disease (25).
In the present, different groups of research work on the search of new biochemical marker capable of predicting the presence and the prediction of cancer prostate. In this way, the pro-inflammatory cytokines have related to PSA production and the progression of cancer prostate (26-28).
Presentation
The object of our study was to relate the expression of several pro-inflammatory cytokines (IL-1, IL-6 and TNF-a), athologic (BPH and PC) prostatic tissue in order to elucidate their possible role in tumor progression. We are also discussing the possible use of these cytokines as a potential therapeutic factor.
Material and metods
In this study we used: transurethral resections from 25 men (aged from 55 to 85 years) diagnosed clinically and histopathologically with benign prostate hyperplasia (BPH); radical prostatectomies from 17 men (aged from 57 to 88 years) diagnosed with prostate cancer (PC) with Gleason scores 3 to 5; and 5 men samples (aged from 20 to 38 years) obtained at autopsy (8-10 hours after death) without histories of, or reproductive, endocrine or related diseases. Each diagnosed sample was divided into three portions; one portion was immediately processed for immunohistochemistry, and the other two portions was frozen in liquid nitrogen and maintained at -80o C for Western Blotting analysis. All pathological, clinical or personal data were anonymized and separated from any personal identifiers. This study was examined and approved by the Military Hospital of Tunis (HMPIT) and Hospital of Fatouma Bourguiba of Monastir (Tunisia), and was made with the consent of the patients' relatives or their family (in autopsy cases).
In order to determine serum PSA levels before the radical prostatectomy, we uses the PSA DPC immulite assays (gifts of Diagnostics Products Corporation, Los Angeles, CA). These assays were performed according to the manufacturer's instructions. The primary antibodies (Santa Cruz Biotechnology, Ca, USA) were: goat anti-human TNF-a, rabbit anti-human IL-1a and rabbit anti-human IL-6, at 1:50 (immunohistoche-mistry) or 1:200 (Western blot) dilutions. In Western blot, mouse anti-chicken a-actin (Amersham, Madrid, Spain) was also used at the same dilution to examine the relative expression of the other proteins.
Procedure specificity was checked using negative and positive controls. For negative controls sections of different group (normal, BPH and cancer) were incubated with preimmune serum at the same immunoglobulin concentration used for each antibody or with blocking peptides (Santa Cruz Biotechnology). As positive controls, histologic sections of thymus (TNF-a and IL-6) and tonsils (IL-1a) were incubated with the same antibodies used in this study.
For each antibody a histologic quantification of immunolabeling was performed. Of each prostate, six histologic sections were selected at random. Using the X40 objective staining intensity (optic density) per unit surface area was measured with an automatic image analyzer (Motic Images Advanced version 3.2, Motic China Group Co., China). For each positively immunostained section, one negative control section was also used, and the optic density of this control section was taken away from that of the stained section. After, means ± SD for each prostatic type were calculated. The same calculation was performed in normal and cancer samples. The statistical significance between means of the different prostate samples was assessed by the Fisher exact and the one-way ANOVA test at p£0.05 (GraphPad PRISMA 3.0 computer program).
Results
Western blot
In BPH and PC, a single band (at their corresponding molecular weight) was found to IL-1a (17 kDa), TNF-a (17 kDa) and IL-6 (21 kDa) (Figure 1). In normal prostates, only TNF-a and IL-6 were detected (at their corresponding molecular weight) (Figure 1).
Average optical densities to IL-1a and IL-6 showed that in PC was more elevated than in BPH, and at the same in BPH was more elevated than in normal prostate. No variations in the average optical densities were found in TNF-a (Table I).
Immunohistochemistry
No immunoreaction was observed in negative controls incubated with pre-immune serum, or using the antibodies preabsorbed with an excess of purified antigens. Staining of thymus (IL-6 and TNF-a) or tonsil (IL-1) sections used as positive controls was always positive.
For each antibody assayed, the percentages of positive cases are shown in Table II.
No immunoreaction was found to IL-1a in normal prostate samples. In BPH patients (Figure 2A) immunostaining was positive in 50% of samples with PSA levels between 0-4 ng/ml and 60% of patients with PSA levels between 4-20 ng/ml (Table II). In PC samples (Fig. 2B), IL-1a was expressed in the groups with PSA levels between 4-20 ng/ml (75%) and PSA >20ng/ml (70% of patients).
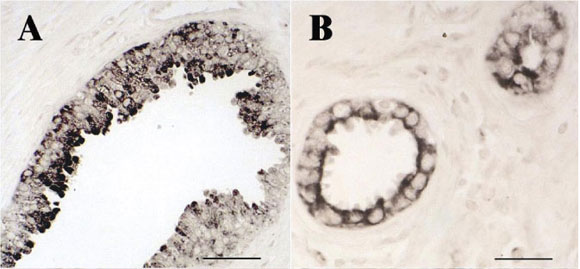
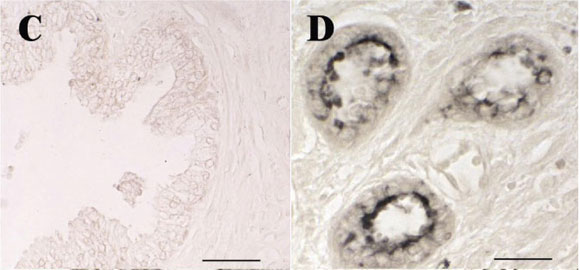
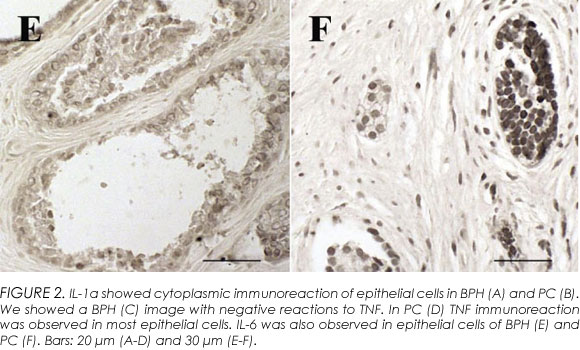
Immunoreaction to TNF-a (Figure 3A-B) was found in NP (40%), BPH (40%) and PC (35.2%) patients (Table II). In BPH (Figure 2C) the percentage of patients' positives samples decrease when increase PSA levels. In PC (Figure 2D), immunoreaction to TNF-a was only positive in two PSA levels groups (PSA levels between 4-20 ng/ml and >20 ng/ml).
In normal prostates, all samples were positives to IL-6. In BPH (Fig. 2E) patients, immunoreaction to IL-6 was positive in the two groups: 0-4 ng/ml (68% of patients) and 4-20 ng/ml of PSA (76.5% of patients). Positive IL-6 immunostaining was seen in 76.5% of PC (Figure 2F, Table II).
Discussion
Catalona et al. (30) established a reference range of 0-4 ng/ml to define normal PSA levels, with a range of 4-10 ng/ml increase the probability of cancer, and levels above 10 ng/ml have a high probability of prostate cancer. Although other studies suggested that PSA levels of 10 ng/ml has little correlation with cancer prostate (31). In this manuscript we present PSA levels above 20ng/ml as the group with elevate probability of cancer patients.
In the present study, IL-1a (not detected in normal prostates) was expressed in 56% of BPH and 70% of PC patients. Similar results have been obtained by our group in previous studies (4), suggesting that IL-1a in epithelial cells seems to be involved in increased cell proliferation associated with BPH and Cancer. In patients with elevated expressions of IL-1a had also elevated PSA levels (PSA>20ng/ml). These finding suggest that in both BPH and PC, high expressions of IL-1a in epithelial cells may be related to cell proliferation and high PSA levels.
In a melanoma cell line (A375), Lázár-Molnár et al. (32) found that endogenous IL-1a production was associated with resistance to exogenous anti-proliferative stimuli and also to the increase in the constitutive production of IL-6 in autocrine manner. Previous results from our laboratory revealed increased IL-6 expression in cancer prostate epithelial cells (22). Since the increase in IL-6 has been associated with bad prognosis in prostate cancer (33-34), the evaluation of IL-1a as IL-6 inductor might be important to assess malignancy. Similar results have been described in breast carcinoma, where expression of IL-6 was enhanced and associated with proliferation cellular markers (20).
The effect of IL-6 on prostate cancer cells is contradictory. Some reports suggested that IL-6 could promote prostate cancer cell growth (35-36), whereas other studies could repress prostate cancer cell growth (26). In our study, we found expression of IL-6 in BPH and PC samples but also that high expression of IL-6 was associated with IL-1a (64.7% samples) and high PSA levels (>20 ng/ml).
TNF-a has shown contradictory effects. Lejeune y cols. (37) observed that local administration of TNF-a in high doses destroyed selectively the tumour blood vessel of the tumor and therefore his great anticarcinogenic power in melanoma. Nevertheless, different studies suggest that endogenous TNF-a is involved in the growth of tumoral cells and in the interactions with the stroma, increasing the tumour invasion and the development of metastasis (7, 8). In our cancer patients, we found that high expressions of IL-6 were associated with TNF-a (35.2% samples) but also with high PSA levels (>20 ng/ml).
In agreement with our results, we suggest that in BPH, the high expression of pro-inflammatory cytokines might be associated with high production of PSA. In CP, the high expression of these cytokines and the high levels of PSA might be involved in the change of polarity of the epithelial cells as well as the quantity of basal cells. At the same time, these cytokines might be involved indirectly in the increase of circulatory levels of PSA.
Conclusions
In CP was an association between the high expression of pro-inflammatory cytokines (TNF-a, IL-6, IL-1), inflammation, elevated PSA serum levels and tumor progression. Inhibition of IL-1, IL-6 and TNF-a might be a possible target for PC treatment. A better understanding of the biologic mechanism and role played by the elevation of circulating PSA related to the tissue expression of these cytokines may improve clinical management and provide new targets for therapy in these patients.
 Correspondence:
Correspondence:
J. R. Cansino Alcalde
General Varela, 32 -4o B
28020 Madrid. (Spain)
urocansino@yahoo.es
Accepted: October 12th, 2008
References and recomended readings (*of special interest, **of outstanding interest)
*1. Dinarello C A. The interleukin-1 family: 10 years of discovery. FASEB J, 1994; 8: 1314. [ Links ]
2. Sims J E, Dower S K. Interleukin-1 receptors. Eur. Cytokine Netw, 1994; 5: 539. [ Links ]
3. Boraschi D, Bossu P, Macchia G, et al. A. Structure-function relationship in the IL-1 family. Front. Biosci., 1: d270, 1996. [ Links ]
**4. Ricote M, Garcia-Tuñon I, Bethencourt F R, et al. Interleukin-1 (IL-1alpha and IL-1beta) and its receptors (IL-1RI, IL-1RII, and IL-1Ra) in prostate carcinoma". Cancer, 2004; 100: 1388. [ Links ]
5. Balkwill F. Tumor necrosis factor or tumor promoting factor? Cytokine Growth. Factor Rev, 2002; 13: 135. [ Links ]
6. Beutler B A. The role of tumor necrosis factor in health and disease. J. Rheumatol. Suppl, 1999; 57: 16. [ Links ]
7. Kollias G, Douni E, Kassiotis G, et al. On the role of tumor necrosis factor and receptors in models of multiorgan failure, rheumatoid arthritis, multiple sclerosis and inflammatory bowel disease. Immunol. Rev, 1999; 169: 175. [ Links ]
**8. Michalaki V, Syrigos K, Charles P, et al. Serum levels of IL-6 and TNF-alpha correlate with clinicopathological features and patient survival in patients with prostate cancer. Br. J. Cancer, 2004; 90: 2312. [ Links ]
9. Hubel K, Mansmann G, Schafer H et al. Increase of anti-inflammatory cytokines in patients with esophageal cancer after perioperative treatment with G-CSF. Cytokine, 2000; 12: 1797. [ Links ]
**10. De Miguel M P, Royuela M, Bethencourt F R, et al. Immunoexpression of tumour necrosis factor-alpha and its receptors 1 and 2 correlates with proliferation/apoptosis equilibrium in normal, hyperplasic and carcinomatous human prostate. Cytokine, 2000; 12: 535. [ Links ]
11. Zubelewicz B, Muc-Wierzgon M, Wierzgon J. Genetic disregulation of gene coding tumor necrosis factor alpha receptors (TNF alpha Rs) in follicular thyroid cancer preliminary report. J. Biol. Regul. Homeost. Agents, 2002; 16: 98. [ Links ]
12. Scott K A, Arnott C H, Robinson S C, et al. TNF-alpha regulates epithelial expression of MMP-9 and integrin alphavbeta6 during tumour promotion. A role for TNF-alpha in keratinocyte migration? Oncogene, 2004; 23: 6954. [ Links ]
13. Rzymski P, Opala T, Wilczak M, et al. Serum tumor necrosis factor alpha receptors p55/p75 ratio and ovarian cancer detection. Int. J. Gynaecol. Obstet, 2005; 88: 292. [ Links ]
**14. García-Tuñon I, Ricote M, Ruiz A, et al. Role of tumor necrosis factor-alpha and its receptors in human benign breast lesions and tumors (in situ and infiltrative). Cancer Sci, 2006; 97: 1044. [ Links ]
**15. Heinrich P C, Behrmann I, Mueller-Newen G, et al. Interleukin 6-type cytokine signaling throught the gp130/jak/stat pathways. Biochem. J, 1998; 334: 297. [ Links ]
16. Kurihara N, Bertolini D, Suda T, et al. IL-6 stimulates osteoclast-like multinucleated cell formation in long term human marrow cultures by inducing IL-1 release. J. Immunol, 1990: 144: 4226. [ Links ]
17. Hacovirta H, Syed B, Jegou B, et al. Function of Interleukin-6 as an inhibitor of meiotic DNA synthesis in the rat seminiferous epithelium". Mol. Cell. Endocrynol, 1995; 108: 193. [ Links ]
18. Krueguer J, Krane J, Carter D, et al. Role of growth factors, cytokines, and their receptors in the pathogenesis of psoriasis. J. Invest. Dermatol, 1990; 94: 135s. [ Links ]
19. Hama T, Miyamoto M, Tsuki H, et al. Interleukin-6 is a neurotrophic factor for promoting the survival of cultured basal forebrain cholinergic neurons fron postnatal rats. Neurosci. Lett, 1989; 104: 340. [ Links ]
**20. García-Tuñon I, Ricote M, Ruiz A, et al. IL-6, its receptors and its relationship with bcl-2 and bax proteins in infiltrating and in situ human breast carcinoma. Histopathology, 2005; 47: 82. [ Links ]
**21. Keller E T, Wanagat J, Ershler W B. Molecular and cellular biology of interleuklin-6 and its receptor. Front. Biosci, 1996; 1: 340. [ Links ]
**22. Royuela M, Ricote M, Parsons M S, et al. Immunohistochemical analysis of IL-6 family of cytokines and their receptors in benign, hyperplastic and malignant human prostate. J. Pathol, 2004; 202: 41. [ Links ]
23. Polascik T J, Oesterling J E, Partin A W. Prostate specific antigen: a decade of discovery - what we have learned and where we are going. J. Urol, 1999; 162: 293. [ Links ]
*24. Bozeman C B, Carver B S, Eastham J A, et al. Treatment of chronic prostatitis lowers serum prostate specific antigen. J. Urol, 2002; 167: 1723. [ Links ]
**25. Roddam A W, Duffy M J, Hamdy F C, et al. NHS Prostate Cancer Risk Management Programme. Use of prostate-specific antigen (PSA) isoforms for the detection of prostate cancer in men with a PSA level of 2-10 ng/ml: systematic review and meta-analysis. Eur. Urol, 2005; 48: 386. [ Links ]
26. Spitto M T, Chang T D. STAT3 mediates IL-6-induced growth inhibition in the human prostate cancer line LNCaP. Prostate, 2000; 42: 88. [ Links ]
**27. Schalken J A. Molecular and cellular prostate biology: origin of prostate-specific antigen expression and implications for benign prostatic hyper-plasia. B.J.U. Int, 2004; 93: 5. [ Links ]
*28. Lin D L, Whitney M C, Yao Z, et al. Interleukin-6 induced androgen responsiveness in prostate cancer cells through upregulation of androgen receptor expression. Clin. Cancer Res, 2001; 7: 1773. [ Links ]
29. Hsu S M, Soban E. Colour modification of diaminobenzidine (DAB) precipitation by metallic ions and its application to double immunohistochemistry. J. Histochem. Cytochem, 1982; 30: 1079. [ Links ]
**30. Catalona W J, Smith D S, Ratliff T L, et al. Measurement of prostate-specific antigen in serum as a screening test for prostate cancer. N. Engl. J. Med, 1991; 324: 1156. [ Links ]
**31. Stamey T A. Preoperative serum prostate-specific antigen (PSA) below 10 microg/l predicts neither the presence of prostate cancer nor the rate of postoperative PSA failure. Clin. Chem, 2001; 47: 631. [ Links ]
32. Lazar-Molnar E, Hegyesi H, Toth S, et al. Autocrine and pararine regulation by cytokines and growth factors in melanoma. Cytokine, 2000; 12: 547. [ Links ]
*33. Twillie D A, Eisenberger M A, Carducci M A, et al. Interleukin-6: a candidate mediator of human prostate cancer morbidity. Urology, 1995; 45: 542. [ Links ]
*34. Shariat S F, Andrews B, Kattan M.W, et al. Plasma levels of interleukin-6 and its soluble receptor are associated with prostate cancer progression and metastasis. Urology, 2001; 58: 1008. [ Links ]
35. Mora L B, Buettner R, Seigne J, et al. Constitutive activation of Stat3 in human prostate tumors and cell lines: direct inhibition of Stat3 signaling induces apoptosis of prostate cancer cells. Cancer Res, 2002; 62: 6659. [ Links ]
36. Liu X H, Kirschenbaum A, Lu M, et al. Prostaglandin E(2) stimulates prostatic intraepithelial neoplasia cell growth through activation of the interleukin-6/ GP130/ STAT-3 signaling pathways. Biochim. Biophys. Res. Commun, 2002; 290: 249. [ Links ]
*37. Lejeune F J, Liénard D, Matter M, et al. Efficiency of recombinant human TNF in human cancer therapy. Cancer Immun, 2006; 6: 6. [ Links ]

