










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkNutrición Hospitalaria
versión On-line ISSN 1699-5198versión impresa ISSN 0212-1611
Nutr. Hosp. vol.33 supl.3 Madrid 2016
https://dx.doi.org/10.20960/nh.313
Comparison of beverage consumption in adult populations from three different countries: do the international reference values allow establishing the adequacy of water and beverage intakes?
Mariela Nissensohn1,2, Daniel Fuentes Lugo3 and Lluis Serra-Majem1,2
1Research Institute of Biomedical and Health Sciences. Department of Clinical Sciences. Universidad de Las Palmas de Gran Canaria. Las Palmas, Spain.
2CIBEROBN - Biomedical Research Networking Center for Physiopathology of Obesity and Nutrition. Carlos III Health Institute. Madrid, Spain.
3Faculty of Health Sciences. Universidad Autónoma del Carmen. Ciudad del Carmen, Mexico
ABSTRACT
Introduction: Recommendations of adequate total water intake (aTWI) have been proposed by the European Food Safety Agency (EFSA) and the Institute of Medicine (IOM) of the United States of America. However, there are differences in the approach used to support them: IOM recommendation is based on average intakes observed in NHANES III (Third National Health and Nutrition Examination Survey) and EFSA recommendation on a combination of observed intakes from 13 different European countries. Despite these recommendations of aTWI, the currently available scientific evidence is not sufficient to establish a cut-off value that would prevent disease, reduce the risk for chronic diseases or improve health status.
Objective: To compare the average daily consumption of fluids (water and other beverages) in selective samples of population from Mexico, US and Spain, evaluating the quantity of fluid intake and understanding the contribution of each fluid type to the total fluid intake. We also aim to determine if they reached adequate intake (AI) values, as defined by three different criteria: IOM, EFSA and water density.
Methods: Three studies were compared: from Mexico, the National Health and Nutrition Survey conducted in 2012 (NHNS 2012); from US, the NHANES III 2005-2010 and from Spain the ANIBES study leaded in 2013. Different categories of beverages were used to establish the pattern of energy intake for each country. Only adult population was selected. TWI of each study was compared with EFSA and IOM AI recommendations, as well as applying the criterion of water density (mL/kcal).
Results: The American study obtained the higher value of total kcal/day from food and beverages (2,437 ± 13). Furthermore, the percentage of daily energy intake coming from beverages was, for American adults, 21%. Mexico was slightly behind with 19% and Spain ANIBES study registered only 12%. ANIBES showed significantly low AI values for the overall population, but even more alarming in the case of males. Only 12% of men, in contrast with 21% of women, do satisfy the EFSA criterion. The IOM criterion reaches even less with higher recommended values for daily intake. In contrast, 60% of the American population reached the recommended intake of the IOM criterion. However, available data did not allow calculating the percentage reached by the EFSA criterion. Data from the Mexican study did not permit conducting comparisons with IOM or with EFSA. However, the water density criteria (mL/kcal) was higher than 1.
Conclusion: There is a notable difference between all three populations in terms of TWI. Furthermore, within the same population, values of adequacy of TWI changed significantly when they were assessed using different criteria. More scientific evidence is required for the production of better defined water intake recommendations in the future as well as more studies focusing on beverage consumption patterns in different settings.
Key words: Adequate total water intake. ANIBES. Energy intake. Beverages. Adults.
Introduction
Adequate total water intake (aTWI) has been proposed by specific age and gender by some international authorities. However, those amounts vary widely. In 2010, the European Food Safety Agency (EFSA) (1) set the aTWI in 2.5 l/day for men and 2.0 l/day for women older than 14 years of age. In contrast, the Institute of Medicine (IOM) (2) of the United States of America set the recommended aTWI in 3.7 l/day for men and 2.7 l/day for women. In Mexico, a panel of experts convened by the Ministry of Health recommended the consumption of 0.75-2.0 l (6 to 8 average size glasses) of water per day. As for other fluids, the panel classified beverages in 6 levels, from level 1 (those that should be consumed as a major beverage, i.e., water) to level 6, the least preferred beverages that should be consumed in limited quantities. In summary, the current recommendations of the IOM, EFSA and the panel of experts agree on basic aspects. They recognize that the value of "adequate intake" (AI) is a variable event in which differences are in part due to the inter-individual variation for water needs in response to different health status, metabolism and environmental factors such as ambient temperature and humidity, as well as individual factors such as age, body size and level of physical activity (3). Furthermore, the water needs also depend partially on overall diet and the water contained in food. Both, the EFSA and the IOM established their recommendations on the same criteria of adequate hydration that include at least 1.0 l per 1,000 kcal and theoretical calculations.
However, there are slight differences in the approach used to support them: IOM set AI based on average intakes observed in NHANES III (Third National Health and Nutrition Examination Survey). They clarify that physical activity and ambient temperature increase water loss and require compensation drinking. Therefore, it uses an osmotic equilibrium criterion to formulate the recommended amounts. In contrast, EFSA based their AI recommendations on a combination of observed intakes in population groups with desirable osmolarity values of urine of 500 mOsmol/l and desirable water volumes per energy unit consumed. The intake data were obtained from observational national surveys in healthy populations in 13 different European countries. They recommended that the AIs only apply in moderate environmental temperatures and at moderate physical activity levels (4).
In 2004, the IOM published the daily reference values of nutrients, including the amount of "water, potassium, sodium, chloride, and sulfate" (2). The suggested intake profile was for an adult male with an average intake of 2,200 kcal/day. All beverages represent 12.5% of the total daily energy intake. Fluid intake was 3.9 l, from which 48% of them would be water, 20% unsweetened drinks (coffee and tea) and 32% milk, juice and other calorie beverages.
In Mexico, the obesity epidemic and the observation of the high increase of sugar sweet beverages intake led to establish an expert panel (5) which, in 2008, developed a set of recommendations on beverage intake for a healthy life including portion size recommendations for each beverage category and healthy consumption patterns for men and women: the Beverage Guidance System. The main conclusion of this panel was that water is the best option and first recommendation for ideal beverage. They also support the World Health Organization recommendation that no more than 10% of the daily calorie intake should come from beverages (6,7).
Even though a TWI has been established, methods to estimate daily ingestion and adequacy of water and other fluids at a population level remain insufficient in the literature. The scientific evidence available is not enough to establish a level of TWI that would prevent disease, reduce the risk for chronic diseases or even improve health status. As a result, there is no clear association between maximum or minimum limits of water consumption that might produce a health benefit by diminishing a specific risk. A proper assessment of water and other beverages intake is important in relation to public health for many reasons, including the need to promote the adoption of healthy life styles in order to avoid the growing epidemic of chronic diseases, many of which are related to unhealthy habits of consumption of different foods and beverages (6,7).
The objective of this paper was to compare the average daily consumption of fluids (water and other beverages) in selective samples of Mexican, US and Spain population, evaluating in each case the quantity of fluid intake and understanding the contribution of each fluid type to the total fluid intake in order to draw conclusions about the adequacy of drinking habits (8). Furthermore, we examined if those populations reached AI values defined by the IOM, the EFSA or by the criterion of water density, a ratio between TWI (ml from food and beverages) and energy intake (kcal). This criterion suggests that water intake is inadequate when the ratio is lower than 1.
Methods
CHARACTERISTICS OF THE THREE STUDIES COMPARED
1. From Mexico, the National Health and Nutrition Survey in 2012 (NHNS 2012) analyzed current patterns of beverage intake in adults and children. The NHNS 2012 was a nationally representative, cross-sectional, multistage, stratified survey whose main objective was to characterize the health and nutritional status of the Mexican population (9). It was conducted from October 2011 to May 2012 on a total of 10,343 individuals. Dietary intake was collected by trained interviewers using a single 24-h recall from both weekdays and weekend days (9,10). Respondents reported all foods and beverages consumed in the previous 24-h time period. Each interviewer was provided with a manual with photos of commonly consumed foods, a food scale, measuring cups, and serving spoons of various sizes to help in estimating the amount of food or beverages (in grams or milliliters) reported by each participant. Beverages were first grouped into 10 broad groups: a) water; b) agua fresca (beverages mixing water with small amounts of fresh natural fruits); c) coffee/tea; d) soda; e) fruit and vegetable beverages; f) milk and milk-based beverages; g) atole (cornstarch beverage); h) sports and energy drinks; i) alcoholic beverages; and j) other beverages. Sodas were further divided into "caloric" and "low calorie" groups. Other beverages, such as coffee/tea with milk and/or added sugars, were classified as caloric or low calorie using their energy density. Finally, all beverages were classified into 17 specific groups that represent all beverages consumed by the Mexican population.
As a result, the mean per-capita consumption of beverages among Mexican adults aged 20-59 years was 382 kcal/day. All beverages represented 19.2% of the total daily energy intake. The top 3 most consumed beverages in these age groups were plain water (74.6%), caloric soda (42.0%), and caloric coffee/tea (37.6%). In terms of calories, caloric soda, caloric coffee/tea, and agua fresca were the top three major contributors to the total daily energy intake per capita. Compared with adult women, men had a significantly higher consumption of caloric soda and alcoholic beverages. Women were higher consumers of plain water compared with men (9).
2. From the US, the National Health and Nutrition Examination Surveys (NHANES) 2005-2010 were conducted using a large and nationally representative database. Estimates of total dietary water from all sources (including plain water), from other beverages and from moisture in foods were compared to the IOM AI values. The analyses used data from three cycles of the study corresponding to years 2005-2006, 2007-2008 and 2009-2010 on a sample of 15,702 adults aged ≥ 20 years. The collection of data was assessed via two 24-h recalls for most respondents, allowing for estimation of usual intakes conducted by trained dietary interviewers in a mobile examination center while the second recall was conducted by telephone some days later (11-14).
Beverages were classified into nine broad groups: a) water (bottled or tap); b) milk (including flavored); c) fruit juice (100%); d) soda/soft drinks (regular and diet); e) fruit drinks; f) sports/energy drinks; g) coffee; h) tea; and i) alcoholic beverages. The NHANES 24-h recalls for each respondent provide information on the amount in grams of each food and beverage consumed. In the analyses of this database, results were all presented in ml of water content from selected beverages, not mean intakes by volume (e.g., ml of water in milk, not ml of milk consumed). Energy intakes from different beverages and foods were estimated for each respondent.
On average, American adults consumed 1.1 l (1,138 ml) of water as a beverage per day. Men and women consumed comparable amounts of water as a beverage. Overall, adults consumed 644 ml/d of tap water (about 56% of total water consumed as a beverage) and 502 ml/d of bottled water (44%). The principal beverage sources were plain water, soda, coffee, tea, milk, and alcohol, followed by fruit drinks and fruit juices. The contribution of plain water, soda (regular and diet), alcohol and fruit drinks to water intakes tended to decrease with age. By contrast, the contribution of coffee and tea to total water intake increased with age. Among adults aged 20-50 years the 83% of total water came from beverages, including 37% from plain water and 17% from moisture in foods. However, 42.7% of men and 40.6% of women adults failed to meet the IOM AI value for total water (3.7 l for men and 2.7 l for women). The contribution of beverages to energy intakes was 21.7% among younger adults (aged 20-50) and declined with the age. For this age group soda accounted for 5.7% of energy intakes (15).
3. From Spain, the ANIBES study was conducted using stratified multistage sampling (16,17). To guarantee better coverage and representativeness, the fieldwork was performed at 128 sampling points across Spain. The final sample comprised 2,007 individuals (1,011 men, 50.3%; 996 women, 49.7%). The fieldwork for the ANIBES study was conducted from mid-September 2013 to mid-November 2013. To equally represent all days of the week, study subjects participated during 2 weekdays and 1 weekend day. For food and beverage records, the study participants were provided with a tablet device (Samsung Galaxy Tab 2 7.0) and trained in recording information by taking photos of all food and drinks consumed during the 3 days of the study, both at home and outside home. Photos were to be taken before starting to eat and drink, and again after finishing, so as to record the actual intake. Additionally, a brief description of meals, recipes, brands, and other information was recorded using the tablet device. Participants who declared or demonstrated that they were unable to use the tablet device were offered other options, such as digital camera and paper record and/or telephone interviews. In addition to details of what and how much was eaten, for each eating/drinking event, participants recorded where they were, who they were eating with, and whether they were watching television and/or sitting at a table. After each survey day, participants recorded if their intake was representative for that day (or the reason why if it was not), and details of any dietary supplements taken. The survey also contained a series of questions about participants' customary eating habits (e.g., the type of milk or fat spread usually consumed) to facilitate further coding. Food records were returned from the field in real time, to be coded by trained coders who were supervised by dieticians. An ad hoc central server software/database was developed for this purpose, to work in parallel with the codification and verification processes. A food photographic atlas was used to assist in assigning gram weights to portion sizes (16,17). Beverages were combined into eight categories for further analysis: a) hot beverages included hot tea and coffee (iced teas in cans or bottles were considered as caloric soft drinks); b) milk (all types of milk without separation by fat percentage); c) fruit and vegetable juices (including nectars and juice-milk blends); d) caloric soft drinks (including sports drinks such as isotonic drinks with mineral salts and caffeinated energy drinks, among others); e) diet soft drinks (with non-sugar sweeteners); f) alcoholic drinks, including two groups: low alcohol grade (mostly beer, wine, and cider) and high alcohol grade; g) water (including tap water and bottled water); and h) other beverages (including soy-based beverages and non-alcoholic beer, among others) (18).
On average, the TWI for adults' age range 18 to 64 years was 1.72 l/day for men and 1.61 l/day for women. Neither men nor women consumed sufficient amounts of water, according to EFSA AI reference values. Men consumed approximately 31% less than the AI and women nearly 20% less. The relative contribution to total EI from beverages was 12.5% for both, men and women. Furthermore, 68% of the TWI came from beverages and 32%, from food. Water was the most frequently consumed beverage followed by milk, for both sexes. Among men, the decreasing order of consumption was alcoholic drinks, caloric soft drinks, and hot beverages, with similar percentages (11.0%, 10.7%, and 10.5%, respectively). For women, the decreasing order was hot beverages (12.5%), caloric soft drinks (8.2%), and alcohol (5.3%). Fruit and vegetable juices and diet soft drinks were consumed in lower amounts by both sexes. In general, the contribution of water intake from food increased with age. This finding is possibly due to lower consumption of fruits and vegetables, which are rich in water, for the youngest participants. Water contribution from beverages declined with age. For adults, the principal sources of total dietary water were plain water, followed by milk. Regarding alcoholic drinks, on average, consumption for men and women were 160 g/day (SE 9.05) and 71 g/day (SE 4.85), respectively. Caloric soft drinks contribution for the entire population was 2.3% of the total kcal per day. However, consumption was lower among adults than in adolescents and among women than in men (18).
Results
The different categories of beverages were used to establish the pattern of energy intake for each of the three studied countries. Only the pattern of adults was selected. TWI of each study was compared with the EFSA, and IOM AI recommendation. Furthermore, the criterion of the water density was applied (ml/kcal) in order to provide a more comprehensive estimate of the proportion in which each country fulfilled the established aTWI. This criterion is based on the energy content per unit volume. The desirable water to energy ratio is considered as other index of AI (15). The value suggested was 1.0 l per 1000 kcal of energy intake. However, this value could be increased to 1.5 l/1,000 kcal depending on the activity level and water loss. TWI for adults should be no less than 1.0 l/1,000 kcal (15).
Table I shows the dietary sources of energy (%) from subgroups of beverages in the three studies included. In order to allow comparison between all three studies, some groups of beverages should be linked (i.e., in the Mexican study, "atole" was included as "other beverages"). Among the three studies selected, the American study obtained the higher value of total kcal/day from food and beverages (2,437 ± 13). Furthermore, the proportion of energy from beverages for average American adults was 21% (also the highest value in the three studies). Mexico was closely behind with 19%. Regarding Spain, the ANIBES study registered a value of 12%, very close to the recommendations of the EFSA, IOM and the panel of experts from Mexico. Milk was the beverage with the highest caloric intake in the Spanish study. It contributed 4.9% of the calories, followed by alcoholic beverages, with 2.9% of the calories. However, in the US study the percentages from the same drinks were higher than in Spain (6.6% and 6.1%, respectively). In Mexico, sugared soft drinks contributed with 6.8% of the calories, followed by coffee and herbal teas (4.1%). Surprisingly, juices and nectars and alcoholic drinks contributed the lowest amount of calories (0.9 and 2.2%, respectively) when compared with Spain and the US.
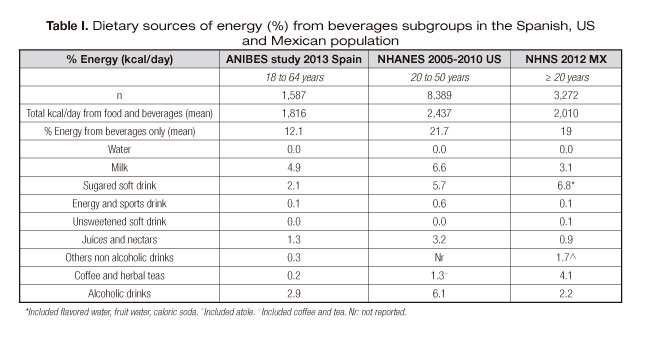
Table II shows the evaluation of adequacy between TWI value of each included study and the aTWI values provided by EFSA, IOM and the ratio ml/kcal. In the ANIBES study from Spain, only 12% of men and 21% of women fulfilled the EFSA recommendation of aTWI (data not shown) (18). Men reached only 69% of the 2.5 l/day recommended, which translates as a deficit of 0.78 l/day (or 31% below the daily recommendation). Women reached an 80% of the recommended aTWI of 2.0 l/day, meaning they had a deficit of 0.4 l/day (20% below the daily recommendation).
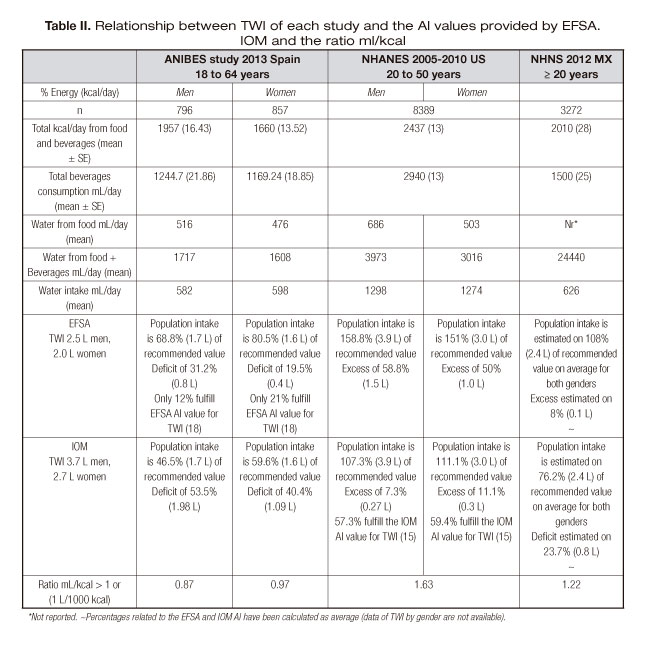
When IOM recommended values are taken into account, the percentages of both, men and women, in the Spanish population become even lower. Men reached only 46.5% of the recommended value of 3.7 l/day and women 60% of 2.7 l/day.
The ratio obtained between ml/kcal ingested was 0.87 for men and 0.97 for women, both values below 1, which is considered as insufficient intake.
In the NHANES study, the situation was literally the opposite to that of the Spanish study: 42.7% of men and 40% of women failed to meet the IOM aTWI (data not shown) (15). However, men reached an overall average of 159% of the 2.5 l/day that EFSA recommended as aTWI, which translates as an excess of 59% or 1.47 l/day over the daily recommendation. For women the excess was 1.0 l/day for the EFSA 2.0L recommendation.
Regarding IOM, there was also a surplus, but in this case, the amount was lower. For men, only a 7% excess (0.27 l/day) and for women the excess was only of 0.3 l/day.
The ratio obtained in this study was 1.63 for both genders. The value obtained was above the cut-point 1.
In the Mexican study, we were not able to make calculations separating men and women. Nonetheless, when considering a TWI of 2.4 l/day, on average the EFSA recommendation was nearly reached, but the IOM recommendation was not. Both sexes reached a 76% of this recommended aTWI, meaning they had a deficit of 0.8 l/day. The ratio obtained in this study was 1.22 for both genders.
In line with previous reports on beverage consumption in Mexico (19,20), the results of the selected study indicate that caloric sugar-sweet beverages (SSB) have been the top source of calories derived from beverages in the Mexican population. This current pattern of beverage consumption is also similar to the United States' beverage patterns. However, since the highest peak in SSB intake in 2001-2002 there has been an important decline in caloric beverage consumption in both, the United States and Mexico (21,22). A great advantage of the NHNS 2012 is that this survey collected very detailed information on plain water consumption. However, this study had several limitations. It is a cross-sectional observational dataset, and the analysis used self-reported intake data, which may be affected by measurement error. Furthermore, the estimates were based on a single 24-h dietary recall; therefore, it may not reflect usual intake or represent the general beverage consumption patterns for the respondents. Despite these limitations, these datasets are the most comprehensive nationally representative data for studying dietary intake in the Mexican population in the last decade (9).
Regarding the US study, the analyses had some limitations. The NHANES data are based on self-reports and are subject to random and systematic reporting errors. Each of the two dietary recall days used different methods to collect the data, which may introduce bias into the estimate of water consumption (15). However, the large sample of the survey helps minimize potential biases of the study.
Concerning the Spain survey, the ANIBES study had several methodological strengths supporting its findings. The use of a 3-day consecutive period was continuously supported by a toll-free telephone number attended by call center-trained operators in order to answer any questions about the software, use of the device, food and beverage record, etc. This careful data collection method is more likely to capture the habitual ingestion of fluids than other methods used in previously published studies. In summary, the study included a careful design, protocol, methodology and employed the highest quality of trendy technology. We do recognize, however, that the study was also subject to few limitations. The possibility of bias in self-reported data is always present, but the large sample collected spreads across age, socio-economic level and geographic region, and greatly reduces the possibility of systematic biases across the whole sample. The study was carried out in the months that represent the transition from summer to autumn seasons (September to November). Season variability is one of the conditions to take into account when the evaluation of the hydration status is performed, so it is also the use of hydration biomarkers that would allow assessment of dietary beverage intake and hydration status without the bias of self-reported dietary intake as well as intra-individual variability (18).
Discussion
The current analysis shows that, in general, American and Mexican population had higher values of energy intake from food and beverages. Results obtained from the Spanish study show significantly low values of aTWI for the overall population, but even more alarming in the case of males. Only 12% of men, in contrast with 21% of women, do satisfy the EFSA criterion. Even less reach the IOM criterion, with higher recommended values for daily intake (3.7 l/day for men and 2.7 l/day for women).
In the American study, almost 60% of the population reaches the recommended intake of the IOM criterion. However, available data does not allow to calculate which percentage reaches the EFSA criterion, it can only be assumed as a higher percentage. Data from the Mexican study neither allows calculations for the IOM nor for the EFSA, but it must be taken into account that the ratio of TWI as ml/kcal was higher than 1 in both, the American and Mexican studies, meaning intake was adequate in broad terms.
The present study raises some questions: a) firstly, how is it possible that the studies' results show such remarkable differences between the amount of food and beverage intake? Is it the methodology used in each study the cause of the different values obtained?; b) secondly, why the recommendations of the EFSA and the IOM are so different? Below these values a person becomes dehydrated?; and finally, c) does an "ideal" pattern of daily liquid intake really exist?.
a) Dietary assessment methodologies have different limitations and advantages (23). One of the most frequent limitations is under-reporting. Even with currently available technologies which allow real-time tracking, until now, there is no single method capable of measuring with perfect accuracy the intake of any nutrient (24).In the case of water consumption there is an additional issue to take into account: it is well know that approximately 20% of the total water intake comes from food, while the remaining 80% comes from fluids. Then, it is necessary to calculate the amount of water that food and drinks contribute to daily water intake. Unfortunately, the amount of water in food is not always available at food composition tables. The focus on water intake is relatively new, and therefore, the science needed for robust methodologies are poorly developed (25). While there is no consensus on how to assess water intake in health, it is essential that surveys develop and use fluid-specific methodologies. Until recently, water intake was not always considered as important in population surveys. Undoubtedly, with increasing interest in intake of all fluids, including water, this is gradually changing so that all fluids, including tap water, are recorded. Data collection of intake and hydration status is an essential step in understanding the relationship between hydration and health. Biomarkers are increasingly being used in population surveys. Even though they are expensive and require ethical approval, biomarkers combined with intake data provide valuable information that is needed to set and evaluate public health policy (4,26).
b) If we consider that recommendations of water consumption or "adequate intake" is based on quantitative surveys of food and beverage consumption, it is easy to understand that they are not always sufficiently well suited for populations, even less if we consider different physiological states. The EFSA AI was based on the desirable values of urine osmolality and the observed intake data of population surveys from 13 European countries. On average, the intakes varied from 720 ml/day in Hungary to over 2,621 ml/day in Denmark (1). Countries of similar climate and cultural backgrounds showed very diverse TWI and patterns of the types of beverages consumed. This disparity throughout Europe cannot be explained solely by the population characteristics or the environmental differences. A great part of these differences derived from the methodology used in the studies (4,27).
The population intake data used by IOM are a single dataset that uses the same methodology. The current recommendation in the United States was established based on experimental criteria of electrolyte balance. Although they do not set a limit for daily intake, these proposed values could be excessive, so caution is advisable.
In addition, it is important to consider that both, the EFSA and IOM recommendations included water from food and beverages. In adults, food contribution to the TWI represents 20% to 30%. However, the overall percentage of water from foods varies between countries, seasons and food types or dietary patterns. Diets rich in fruits, vegetables and soups provide greater amounts of liquid than other types of diet. Furthermore, while the AI values established provide some benchmark in evaluating water intake, the proportions below this value should be interpreted cautiously. The use of biomarkers to evaluate hydration status at the population-level should be a priority (15).
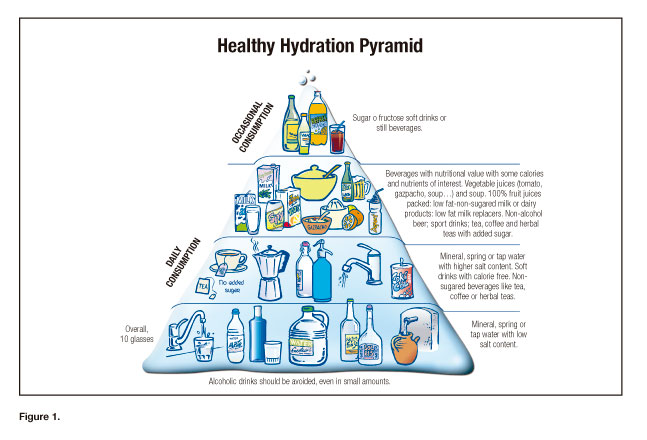
c) Overall, data Available at the literature on beverage consumption pattern is scarce. Although fluid requirements vary widely among individuals and population (2,6), the Spanish Society of Community Nutrition (SENC) (28) made a Healthy Hydration Pyramid (Fig. 1) to be used as a guide for water intake to Spanish population. It is a practical and convenient tool that sets the recommendation in a simple and didactic way. They divide beverages into five groups: group 1 included mineral water, spring water or tap water with low salt content; group 2 included mineral or tap water with higher salt content, soft drinks non sugar/non-caloric, tea or coffee without sugar; group 3 included beverages with some calorie and nutrient content of interest, natural fruit juices, vegetable juices (tomato, gazpacho) and stews, milk or low-fat dairy products with or without sugar, alcohol-free beer, sports drinks, tea or coffee with sugar; group 4 included carbonated soft drinks not sweetened with sugar or fructose; and group 5 included low graduation alcoholic drinks. Although they are not included in the pyramid, moderate consumption is allowed.
Conclusion
The difference between EFSA and IOM recommendations is considerably large in terms of TWI. Although both of them include the water contained in food and both have their strengths and weaknesses, there is a notable difference of nearly 50% between European recommended values when compared to those of the US. Therefore, it is impossible that percentages of an individual or a given group or population can meet one criteria without underachieving or, in due case, exceeding the other.
However, although there is great variability in global reference values, the recommendations for aTWI may help to establish public health policies and programs oriented to promote adoption of healthy life styles.
The human body is able to adapt to a wide variety of fluid losses, thanks to the wide ranges of urine osmolarity that the kidneys are able to achieve homeostatic regulation. However, unfortunately, so far there are not enough studies focused on the amount of water needed to prevent disease or improve health. More scientific evidence is required for the production of better defined water intake recommendations in the future as well as more studies looking at beverage consumption in different settings.
Acknowledgements
The authors would like to thank the II International and IV Spanish Hydration Congress for its support.
References
1. European Food Safety Association: EFSA Panel on Dietetic Products, Nutrition, and Allergies. Scientific opinion on dietary reference values for water. EFSA Journal 2010;8(3):1459. pp. 48. [ Links ]
2. Institute of Medicine. Dietary reference intakes for water, potassium, sodium, chloride and sulfate. Food and Nutrition Board editor. Washington, DC: The National Academies Press; 2004. [ Links ]
3. Jéquier E, Constant F. Water as an essential nutrient: The physiological basis of hydration. Eur J Clin Nutr 2012;64:115-23. [ Links ]
4. Gandy J. Water intake: Validity of population assessment and recommendations. Eur J Nutr 2015;54(Suppl. 2):11-6. [ Links ]
5. Barquera S. The Mexican experience: From public health concern toward national beverage guidelines. Nutr Today 2010;45:S18YS21. [ Links ]
6. Rivera J, Muñoz-Hernández O, Rosas-Peralta M, Aguilar-Salinas CA, Popkin BM, Willett WC. Consumo de bebidas para una vida saludable: recomendaciones para la población mexicana. Salud Publica Mex 2008;50:173-95. [ Links ]
7. WHO/FAO. Diet, nutrition and the prevention of chronic diseases. Geneva: World Health Organization; 2002. Report no. 916. [ Links ]
8. Martínez H. Fluid intake in Mexican adults; a cross-sectional study. Nutr Hosp 2014;1;29(5):1179-87. [ Links ]
9. Stern D, Piernas C, Barquera S, Rivera JA, Popkin BM. Caloric beverages were major sources of energy among children and adults in Mexico, 1999-2012. J Nutr. 2014;144(6):949-56. [ Links ]
10. Grunwald GK, Seagle HM, Peters JC, Hill JO. Quantifying and separating the effects of macronutrient composition and non-macronutrients on energy density. Br J Nutr 2001;86:265-76. [ Links ]
11. Centers for Disease Control and Prevention: National Health and Nutrition Examination Survey (NHANES): MEC in-person dietary interviewers procedures manual. Available at: http://www.cdc.gov/nchs/data/nhanes/nhanes_05_06/dietary_mec.pdf. [ Links ]
12. Centers for Disease Control and Prevention: National Health and Nutrition Examination Survey (NHANES): phone follow-up dietary interviewer procedures manual. Available at: http://www.cdc.gov/nchs/data/nhanes/nhanes_05_06/DIETARY_PFU.pdf. [ Links ]
13. Centers for Disease Control and Prevention: National Health and Nutrition Examination Survey (NHANES): dietary interview component. Available at: http://www.cdc.gov/nchs/data/nhanes/nhanes_05_06/dietaryrecall_d.pdf. [ Links ]
14. Centers for Disease Control and Prevention: National Health and Nutrition Examination Survey (NHANES): 2005-2006 dietary interview documentation. Available at: http://www.cdc.gov/nchs/nhanes/nhanes2005-2006/DRXDOC_D.htm#Protocol_and_Procedure. [ Links ]
15. Drewnowski A, Rehm CD, Constant F. Water and beverage consumption among adults in the United States: Cross-sectional study using data from NHANES 2005-2010. BMC Public Health 2013;12;13:1068. [ Links ]
16. Ruiz E, Ávila JM, Castillo A, Valero T, Del Pozo S, Rodríguez P, et al. The ANIBES study on energy balance in Spain: Design, protocol and methodology. Nutrients 2015;7:970-98. [ Links ]
17. Ruiz E, Ávila JM, Valero T, Del Pozo S, Rodríguez P, Aranceta-Bartrina J, et al. Energy intake, profile, and dietary sources in the Spanish population: Findings of the ANIBES study. Nutrients 2015;12;7(6):4739-62. [ Links ]
18. Nissensohn M, Sánchez-Villegas A, Ortega RM, Aranceta-Bartrina J, Gil A, González-Gross M, et al. Beverage consumption habits and association with total water and energy intakes in the Spanish population: Findings of the ANIBES study. Nutrients 2016. In press. [ Links ]
19. Barquera S, Campirano F, Bonvecchio A, Hernández L, Rivera J, Popkin B. Caloric beverage consumption patterns in Mexican children. Nutr J 2010;9:47-56. [ Links ]
20. Barquera S, Hernández-Barrera L, Tolentino ML, Espinosa J, Ng SW, Rivera JA, et al. Energy intake from beverages is increasing among Mexican adolescents and adults. J Nutr 2008;138:2454-61. [ Links ]
21. Euromonitor International. Soft drinks. Available at: http://www.euromonitor.com/soft-drinks. [ Links ]
22. Piernas C, Ng SW, Popkin B. Trends in purchases and intake of foods and beverages containing caloric and low-calorie sweeteners over the last decade in the United States. Pediatr Obes 2013;8:294-306. [ Links ]
23. Welch A. Dietary assessment. In: Gandy J (ed.). Manual of dietetic practice. Oxford: Wiley-Blackwell; 2014. pp 61-6. [ Links ]
24. Nelson M. The validation of dietary assessment. In: Margetts B, Nelson M (eds.). Design concepts in nutritional epidemiology. Oxford: Oxford Medical Publications; 1997. pp 241-73. [ Links ]
25. Popkin BM, D'Anci KE, Rosenberg IH. Water, hydration, and health. Nutr Rev 2010;68:439-58. [ Links ]
26. Pfeiffer CM, Schleicher RL, Johnson CL, Coates PM. Assessing vitamin status in large population surveys by measuring biomarkers and dietary intake-Two case studies: Folate and vitamin D. Food Nutr Res 2012;56. [ Links ]
27. Nissensohn M, Castro-Quezada I, Serra-Majem L. Beverage and water intake of healthy adults in some European countries. Int J Food Sci Nutr 2013;64(7):801-5. [ Links ]
28. Serra-Majem L, Aranceta J. Recomendaciones para una hidratación saludable. Revista Española de Nutrición Comunitaria 2008;14(2):114-6. [ Links ]
![]() Correspondence:
Correspondence:
Mariela Nissensohn.
Research Institute of Biomedical and Health Sciences.
Department of Clinical Sciences.
Universidad de Las Palmas de Gran Canaria.
C/ Juan Carlos de Quesada.
35001 Las Palmas, Spain
e-mail: mnissensohn@acciones.ulpgc.es

