










 Servicios personalizados
Servicios personalizados
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por email Citado por SciELO
Citado por SciELO  Citado por Google
Citado por Google  Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google 
 Permalink
PermalinkINTRODUCTION
Currently, non-communicable diseases (NCD) kill 40 million people each year, equivalent to 70% of all deaths globally 1. Cardiovascular disease (CVD) accounts for most NCD deaths and is considered as a serious global public health problem 1,2.
Coronary artery bypass grafting (CABG) is one of the most common cardiac surgical procedures for CVD patients 3. CABG is accepted as the standard treatment for ischemic coronary disease in many patient subgroups. It is widely reported that oxidative stress increases in patients undergoing cardiovascular surgery and can cause postoperative complications 3,4,5.
Malondialdehyde (MDA) is an indicator that is commonly used to assess oxidative stress. MDA is a product of lipid peroxidation, a process induced by free radicals, and it can be estimated by measuring thiobarbituric acid reactive substances (TBARS; nmol/l). This method is one of the best and most frequently used in basic and clinic research 6.
In this context, nutrition serves an important function in the immunological system because it plays a role in fighting oxidative stress. Vitamin A and zinc are among the micronutrients that perform this function.
Studies have shown the important role that vitamin A plays in preventing and/or delaying the atherogenesis process; it prevents LDL oxidation and the oxidative lesion of endothelium and decreases cytotoxicity of high-dose oxidized low-density lipoprotein 7,8. In addition, Ochoa et al. 4 reported a significant decrease in vitamin A serum concentration after cardiovascular surgery, implying that the decreased antioxidant defenses in these patients may increase the incidence of postoperative complications and mortality.
Zinc deficiency is an important factor that can affect the blood concentrations of vitamin A because zinc plays a role in the metabolism of this vitamin, particularly in its transportation 9,10.
The principal mechanisms behind this dependence are related to the regulatory role of zinc in vitamin A transport, which is mediated by protein synthesis and the oxidative conversion of retinol to retinaldehyde. This conversion requires the action of the zinc-dependent retinol dehydrogenase enzyme 8. Thus, zinc deficiency may contribute to vitamin A deficiency 11, and interfere with the intestinal absorption of retinol even in the presence of adequate liver reserves of vitamin A 12. Zinc is required for the synthesis and hepatic secretion of retinol binding protein (RBP) 10. In cases of zinc deficiency, the RBP synthesis may be impaired, which triggers a secondary vitamin A deficiency 12.
Some studies of retinol supplementation in patients suffering from cardiopathy have presented conflicting results. However, such studies do not assess the relationship between vitamin A supplementation and zinc nutritional status 13,14. Considering that the use of vitamin A supplementation needs to be accompanied by the evaluation of the nutritional status of zinc, the present study was carried out.
MATERIALS AND METHODS
This study is a controlled trial that enrolled 90 patients with a primary diagnosis of angina pectoris (using the criteria of the Canadian Cardiovascular Society15)) who underwent coronary artery bypass grafting in a Rio de Janeiro public hospital. The study was approved by the local ethics committee (CAAE 0005.0.185.185-07), and all of the participants signed informed consent forms.
To achieve 80% statistical power and a significance level of 5% (p < 0.05), the sample size was calculated as 30 patients for each group. The patients were assigned to one of two groups (2 x 1). The control group patients (G1 = 60) received a standard diet in accordance with the usual practices of the hospital. For 21 days, the individuals in the vitamin A intervention group (G2 = 30) received a daily supplementation of 5,000 IU of vitamin A in the form of retinol palmitate. These two groups were divided into two additional subgroups: patients with adequate zinc concentrations and patients with inadequate zinc concentrations.
Supplementation, delivered in the form of a capsule, began immediately after the blood was collected at baseline (T0), before surgery. The patients in both groups were observed for 21 days, and additional blood was collected at the 3rd day after surgery (T1) and the 21st day after surgery (T2).
The inclusion criteria were as follows: a) admission for elective coronary artery bypass grafting surgery; b) age ≥ 20 years old 16; and c) formal authorization was given to participate in the study. Considering that hypoalbuminemia is associated with a worse postoperative prognosis, the patients who had serum albumin ≤ 3.5 g/dl were automatically excluded from the study.
The individuals with the following conditions were also excluded: malabsorption syndrome, acute and chronic infections, liver disease, kidney disease, alcoholism or acquired immunodeficiency syndrome (AIDS), as well as individuals who had taken medication or a vitamin supplement containing vitamin A or zinc in the last six months or who underwent prior revascularization surgery.
High performance liquid chromatography (HPLC-UV) was used to quantify the serum levels of retinol and β-carotene 17. In the current study, inadequate levels of serum retinol and β-carotene were defined as < 30 µg/dl and ≤ 40 µg/dl, respectively 18,19. The zinc levels were evaluated using atomic absorption spectrometry, and inadequate zinc values were defined as < 0.7 mg/l 20. The MDA levels were evaluated using spectrophotometry 21 and the HPLC-UV method 22. Body mass index (BMI) was assessed by dividing weight (kg) by height (m), squared, and using the World Health Organization (WHO) (1995) cut-off points 23.
Hypertension, dyslipidemia and/or diabetes mellitus diagnoses were obtained from the patients' medical records. The lipid profile was classified according to the Brazilian Society of Cardiology's V Brazilian Guidelines on Dyslipidemias and Atherosclerosis Prevention 24. Serum glucose levels were classified according to the standards of the American Diabetes Association 25. Blood pressure was classified according to the VII Brazilian Guidelines on Hypertension 26.
All deaths occurring during the duration of hospitalization or the first month after surgery were counted as operative mortality. The hospitalization time and the period of ICU stay were noted through visits and checking the patients' medical records.
To analyze the data, the central tendency and dispersion measurements were calculated. To assess the association between the categorical variables, a Chi-squared test was employed. To compare the continuous variables, Student's t-test was employed, as well as Spearman's correlation coefficient. The statistical analysis was conducted with the Statistical Package for the Social Sciences (SPSS version 20).
RESULTS
The sample included 90 patients who were divided into two groups by a randomized table: 60 patients in G1 and 30 patients in G2.
There were no statistically significant differences observed between the groups in terms of the general patient characteristics (Table 1).
Table I. General characteristics of the study population

*No possibility of statistical calculation.
SH: systemic hypertension; DLP: dyslipidemia; DM: diabetes mellitus.
There was no statistically significant difference in the vitamin A serum levels (retinol and β-carotene) between the groups at T0. At T1 and T2, statistically significant differences were found between the groups for both variables (Table 2).
Table II. Mean values of retinol and β-carotene serum concentrations, according to zinc nutritional status, before and after coronary artery bypass grafting
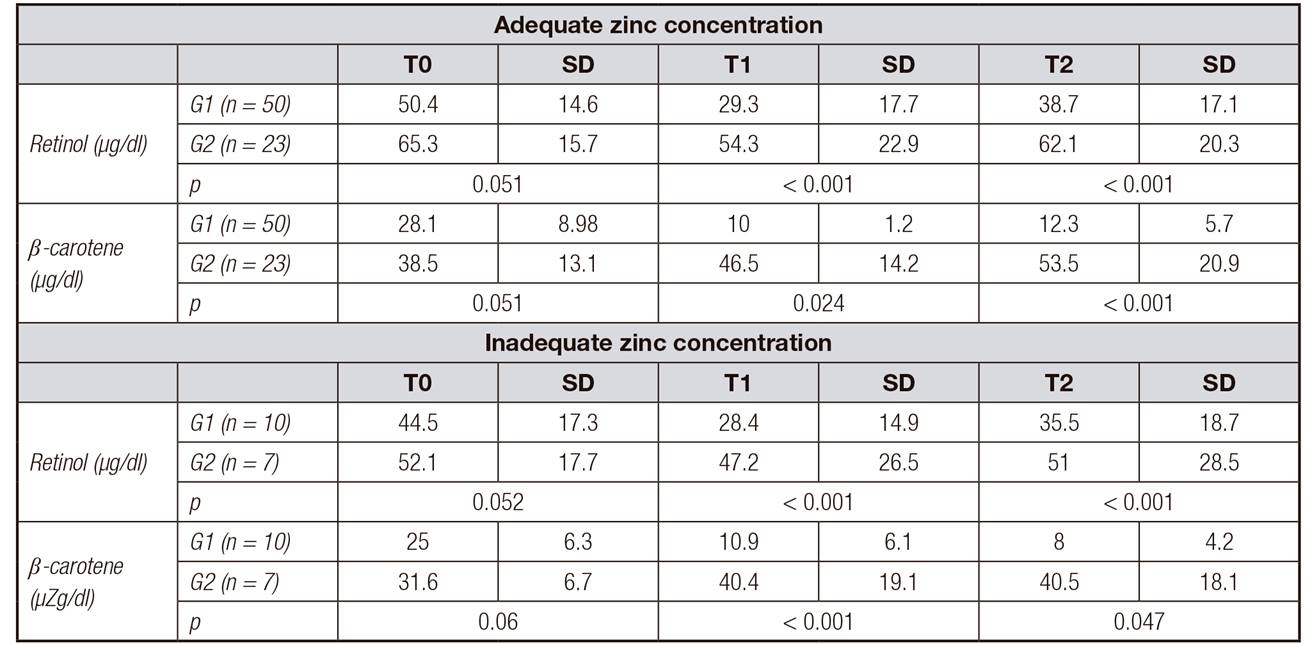
G1: control group; G2: intervention group; T0: before surgery; T1: 3rd day after surgery; T2: 21st day after surgery.
The serum retinol concentrations measured before and after the surgical procedure decreased significantly from T0 to T1 in G1 (p < 0.001) and G2 (p < 0.001). There was an increase at T2 in G1 and G2; however, these concentrations did not reach the levels initially observed at T0 for the individuals with adequate zinc concentrations in G1 or G2 (p < 0.001). The same result was also observed in the individuals who had inadequate zinc concentrations.
For both G1 and G2, zinc-deficient patients had retinol serum concentrations that were significantly lower at T1 (p < 0.001 for both groups) and T2 (p < 0.001 for both groups), compared to the patients with adequate zinc concentrations in both groups.
The β-carotene concentrations were significantly higher in G2 than in G1 in the individuals with adequate and inadequate zinc concentrations at T1 (G1 and G2, p = 0.024 and p < 0.001, respectively) and at T2 (G1 and G2, p < 0.001 and p = 0.047, respectively) (Table 2).
Comparing the zinc levels of the G2 patients, we found that the β-carotene concentrations were significantly higher in the individuals with appropriate zinc concentrations at T1 (p < 0.001) and T2 (p = 0.043), compared to the individuals with inadequate concentrations.
As shown in Table 3, the prevalence of inadequate retinol and β-carotene was lower in G2 than in G1 for the patients who had adequate and inadequate serum concentrations of zinc, although the difference was more pronounced in those with inadequate concentrations of zinc.
Table III. Prevalence of inadequate retinol and β-carotene levels in G1 and G2 before and after coronary artery bypass grafting, according to zinc nutritional status

G1: control group; G2: intervention group; T0: before surgery; T1: 3rd day after surgery; T2: 21st day after surgery.
After supplementation, a statistically significant, strong, positive correlation was found between the retinol and β-carotene concentrations (r = 0.852 and p = 0.014) in the patients who had adequate serum zinc concentrations.
After surgery, the mean MDA levels were significantly higher in the individuals who had inadequate zinc concentrations, compared to the individuals who had adequate zinc concentrations (Table 4).
No statistically significant difference was found between the MDA results obtained through HPLC-UV and the results obtained through spectrophotometry (p = 0.051).
Table IV. Mean concentrations of levels of malondialdehyde (nmol/l) according to the nutritional status of zinc in G1 and G2 before and after coronary artery bypass grafting
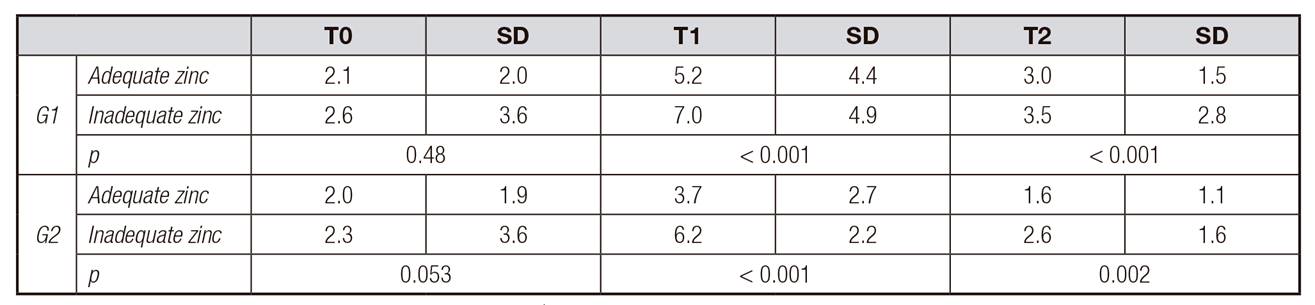
G1: control group; G2: intervention group; T0: before surgery; T1: 3rd day after surgery; T2: 21st day after surgery.
There was no statistically significant relationship found between MDA levels and vitamin A serum concentrations when we analyzed patients according to their zinc nutritional status. Note that among the patients with zinc inadequacy, 69% had both retinol and β-carotene deficiencies. The deficiencies were more common in the patients with higher circulating MDA concentrations (located at quartiles 50 and 75 immediately after the surgery), but the difference did not reach statistical significance.
Analyzing the clinical evolution, a shorter hospital stay in G2 (13.4 ± 9.4) compared to G1 (25.4 ± 17.3) was observed in patients with adequate levels of zinc (p = 0.001).
Regarding the length of stay in ICU, this difference was observed in those with adequate levels of zinc (G1 = 8.5 ± 9.9 / G2 = 4.6 ± 6.4, p = 0.047) and inadequate (G1 = 8.7 ± 10.5 / G2 = 2.7 ± 0.4, p = 0.039). Operative mortality was found to be 8.33% in G1 and 3.33% in G2.
DISCUSSION
The antioxidant role that vitamin A plays in CVD patients has been documented in the literature 27,28. However, its relationship with zinc nutritional status in these individuals has not yet been described.
Patients undergoing coronary artery bypass grafting are exposed to high oxidative stress that increases the demand for antioxidants. In addition, they suffer a period of ischemia-reperfusion that exacerbates the production of free radicals and further depletes the nutrients serving an antioxidant function 4,5.
In the current study, a significant post-surgery reduction in the retinol and β-carotene serum concentrations was observed in G1 at T1 and T2 in the patients with adequate and inadequate serum zinc concentrations. This result corroborates the study by Schindler et al. 29, who found a significant reduction in retinol concentrations 48 hours after surgery, and the study by Gu et al. 30, who found significantly lower β-carotene concentrations in the patients undergoing coronary artery bypass grafting. These studies did not assess the patients' zinc concentrations.
Although the human body has antioxidant defense mechanisms that protect tissues from the cellular damage induced by oxidative stress, stress remained high in the assessed patients, and this stress level may result in the significant depletion of antioxidant nutrients 5. This depletion may explain the mean concentrations of MDA after surgery, which were significantly higher in the individuals who had inadequate serum zinc concentrations than in the individuals who had adequate concentrations in G1 (p < 0.001) and G2 (p < 0.001) at T1 and in G1 (p < 0.001) and G2 (p = 0.002) at T2. These findings correspond with those of Bao et al. 31, who found an inverse association between concentrations of zinc and malondialdehyde in a double-blinded study. Jain et al. 32 found a positive correlation between the total antioxidant capacity and low serum zinc concentrations.
Based on the serum zinc concentrations, no correlation was observed between the concentrations of MDA and vitamin A. Because of strict homeostatic control, zinc concentrations can fluctuate above real limits, even in individuals with low body stores of this nutrient. Maintaining a relatively constant zinc concentration is essential to ensure the normal functioning of an organism. Thus, serum and plasma concentrations are often the methods that are utilized to evaluate the nutritional state of zinc in the body 20.
The data from the current study demonstrate that inadequate serum retinol and β-carotene were more common in patients with higher circulating concentrations of MDA (located at quartiles 50 and 75). Although they did not reach statistical significance, these findings match the observation of Stahl et al. 33 that carotenoids are related to the inhibition of TBARS formation, and they also corroborate Hozawa et al. 34 who, in a longitudinal study that lasted 15 years, demonstrated that carotenoids are negatively correlated with F2-isoprostanes, an oxidative stress product.
Adequate vitamin A nutritional status reduces the biotransformation of carotenoids into retinol, which demonstrates the relationship between the nutritional status of retinol and the nutritional status of carotenoids 35. β-carotene is known as the most powerful retinol precursor. The current study corroborates the findings of Mecocci et al. 35, who demonstrated that a decrease in β-carotene serum concentration corresponds to a decrease in circulating retinol, suggesting the mobilization of β-carotene for retinol conversion. This finding deserves attention, because the reduction in β-carotene serum concentration follows the increase in oxidative stress, demonstrating that this powerful sweeper of free radicals could most likely be diverted to other important functions, such as fighting oxidative stress, to maintain an adequate retinol nutritional status.
Zinc nutritional status can also affect the blood concentration of vitamin A because it damages hepatic synthesis and RBP secretion 10,11. These findings show that significantly lower retinol and β-carotene serum concentrations after surgery in individuals with zinc deficiency may indicate a relationship between zinc nutritional status and vitamin A serum concentrations, as observed in patients undergoing coronary artery bypass grafting. However, no previous studies have shown that evaluating zinc nutritional status is truly a valid measure without considering the levels of circulating RBP. Thus, the results related to vitamin A supplementation in such patients may be masked. Studies that focus on the variables that are attributable to RBP levels and other factors, such as the use of fibrates and thiazolidinediones, thyroid function, iron levels and ferritin levels, should be performed.
Moreover, there are no available data concerning the patients with profiles such as those presented here, which makes it impossible to compare the results to other studies, although this relationship is well established in the classic risk group literature 36,37.
The results showed relevant improvement in the vitamin A levels in G2 patients who had adequate serum zinc concentrations and, consequently, less oxidative stress, which can contribute to a better prognosis among these patients.
Mortality is one of the possible complications after myocardial revascularization 38, and data about this outcome can vary widely depending on the center, country and other factors 39. In our research operative mortality was found to be 8.33% in the control group and 3.33% in the supplemented group. Gomes et al. 40 evaluated Brazilian patients undergoing various types of cardiac surgeries, among them, CABG, and the overall postoperative mortality, up to seven days post-surgery, was 4%, and 2.6% for CABG, being similar to G2. The mortality rates documented in developed nations after cardiac surgeries in general are 2.1% and for CABG are 1.8% 41.
A study that assessed surgical patients found a connection between retinol deficiency and postoperative complications 42. However, this study did not address serum zinc concentrations. According to Barbosa, in a double-blind, placebo-controlled study, supplementation with antioxidants, including zinc, yielded greater protection against oxidative stress 43. We noticed a significantly shorter time in hospital among those from the supplemented group with adequate zinc levels, and with no statistically significant difference in the zinc deficient patients, suggesting that the dosage of vitamin A used was not effective in individuals with hypozincemia.
Although no study with the same characteristics than the present one was found, Shehzad et al. 44, in a randomized controlled trial, assessed 300 children hospitalized with pneumonia and observed a significantly shorter duration of hospital stay in the supplemented group (20 mg zinc/day q 12 hourly) than the placebo group (p < 0.001). In contrast, Yuan et al. 45 also evaluated hospitalized children with pneumonia (n = 96), and did not found significant reduction in the duration of hospital stay between the supplemented group and placebo.
Vitamin A supplementation was shown to have a positive effect regardless of zinc concentrations by analyzing length of stay in ICU. There was a significant difference between the groups both in patients with adequate and inadequate zinc concentrations. Visser et al. 46, in a systematic review and meta-analysis, observed that micronutrient supplementation, including zinc, was not associated with a significant difference in the length of ICU stay. Still in this context, Hasanzadeh Kiabi et al. 47 assessed 186 adults during their ICU stay and found that zinc supplementation may be associated with a significant reduction in the occurrence of ventilator-associated pneumonia in adult mechanically ventilated trauma patients.
The results of the current study showed that vitamin A supplementation had a positive impact on individuals with adequate zinc concentrations by combating oxidative stress in these patients, thus reducing the risk of postoperative complications. The findings presented here can be considered to be an important contribution to the issue addressed, and they may also generate subsidies to future studies of the postoperative management protocol for the group in question, and improve the outcomes for these patients.

