










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkAnales de Psicología
versión On-line ISSN 1695-2294versión impresa ISSN 0212-9728
Anal. Psicol. vol.31 no.2 Murcia may. 2015
https://dx.doi.org/10.6018/analesps.31.2.172151
Walking as physical exercise in Fibromyalgia: An elicitation study from the Theory of Planned Behavior
Andar como forma de ejercicio físico en la Fibromialgia: un estudio de identificación de creencias desde la Teoría de la Acción Planeada
María-Ángeles Pastor1, Sofía López-Roig1, Yolanda Sanz1, Cecilia Peñacoba2, Margarita Cigarán2, Lilian Velasco2, Ana Lledó y Carmen Écija2
1 Departamento de Psicología de la Salud. Universidad Miguel Hernández.
2 Departamento de Medicina y Cirugía, Psicología, Medicina Preventiva y Salud Pública e Inmunología y Microbiología Médica. Universidad Rey Juan Carlos de Madrid
ABSTRACT
This study is the first phase of the formative research recommended in the Theory of Planned Behavior for the development of an intervention. Our aims are to identify modal beliefs about the performance of an exercise pattern in people with fibromyalgia, to test the items designed for direct evaluation of the predictive constructs and to explore their relationships with the behavior. We assessed 46 women with fibromyalgia. Content analysis showed more positive than negative consequences related to the performance of exercise guidelines (behavioral beliefs). Families and friends are the important referents (normative beliefs) and we identified facilitating and inhibiting factors in the performance of exercise behavior related to aspects of fibromyalgia (control beliefs) such as pain, fatigue and emotional state. The subjective norm scale showed the lowest internal consistency (α= .78). The results confirmed the sedentary lifestyle of the participants (previous behavior: Mean=3.67; rank=1-7) although they also suggested that participants intended to perform the behavior (Mean=5.67). The relationships between constructs are coherent with the theory, and support the relevance of applying it to the selected behavior and population.
Key words: Walking; beliefs; fibromyalgia; theory of planned behavior; formative research; elicitation study.
RESUMEN
Este estudio corresponde a la primera fase de investigacion formativa recomendada en la teoria de la Accion Planeada para desarrollar una intervencion. Nuestros objetivos son identificar las creencias modales sobre la realizacion de una pauta de ejercicio en personas con fibromialgia, probar los items para la evaluacion directa de los constructos predictivos y explorar sus relaciones con la conducta. Evaluamos a 46 mujeres con fibromialgia. El analisis de contenido mostro un mayor numero de consecuencias positivas que negativas asociadas a la ejecucion de la pauta de ejercicio (creencias comportamentales); la familia y los amigos son los referentes importantes (creencias normativas) y se detectaron factores facilitadores e inhibidores de la ejecucion de la conducta de ejercicio, relacionados con aspectos de la fibromialgia (creencias de control) como el dolor, la fatiga y el estado de animo. El indice de consistencia interna mas bajo fue el de la escala de norma subjetiva (α= .78). Los resultados confirman el sedentarismo de la muestra (conducta previa: Media=3.67; rango=1-7) aunque tambien sugieren que estas personas tienen intencion de realizar la conducta (Media= 5.67). Las relaciones obtenidas entre los constructos son las esperadas desde la teoria, apoyando la pertinencia de aplicarla en la conducta y poblacion seleccionada.
Palabras clave: Andar; creencias; fibromialgia; teoria de la accion planeada; investigacion formativa; estudio de identificacion.
Introduction
Fibromyalgia is a syndrome of unknown aetiology, which is defined by generalized musculo-skeletal pain that is present for more than three months, along with tiredness, sleep disorders, anxiety and depression amongst other symptoms (Wolfe et al., 1990). In Spain the estimated prevalence in general population is of 2.37%, being more frequently in women (4.2%) than men (0.2%) (Carmona et al., 2001). In a more recent study carried out in 5 different European countries, Spanish prevalence in general population was found to be higher than in the previous mentioned study (total: 4.0%; men: 2.7%; women: 5.2%) although the gender difference remains. Nevertheless, in the latter, prevalence was estimated using a questionnaire that was answered over the phone (Branco et al., 2010). Rheumatology services estimate that the average yearly cost per fibromyalgia patient is 9982 Euros, and 35% of these costs are attributed to direct or health costs (Rivera et al., 2009). In primary care, the yearly average extra cost per patient with fibromyalgia, in comparison to patients with other chronic disorders, is of 5010 euros (Sicras-Mainar et al., 2009).
Treatment for fibromyalgia constitutes one of the most controversial aspects; this is due to the large variety of therapeutic options, their moderate efficacy, the variability in therapeutic response and the poor adherence shown by the patients (Dobkin, Sita & Sewitch, 2006; Rivera, Alegre, Nishishinyac & Heredad, 2006; Schachter, Busch, Peloso & Sheppard, 2003). Currently, there is evidence that the most efficient interventions are the ones that include physical exercise in conjunction with pharmacological treatment and cognitive-behavioural therapy (Hauser, Thieme &Turk, 2010).
Low- to moderate-intensity physical exercise, such as walking, when carried out gradual and regularly, reduces pain, tiredness, depression and other functional limitations in patients with fibromyalgia, as well as increasing perceptions of self-efficacy in managing the problem (Busch, Schachter, Overend, Peloso & Barber, 2008; Hauser, Klose et al., 2010; Richards & Scott, 2002; van Koulil et al., 2007). Performing physical activities, such as walking regularly, are a simple recommendation that can be self-managed by the patients. In opposition to other types of exercise that are managed by professionals in rehabilitation contexts or in gyms, walking depends exclusively on individual motivation that needs to be maintained for the longer term. Furthermore, it means that the patient is involved in a therapeutic task and will therefore increase self-management (Rooks et al., 2007). From an economic perspective, walking is a health tool that is inexpensive, and if the patient maintains it, is efficient even when compared to pharmacological treatment, therefore reducing socio-sanitary public spending associated to fibromyalgia (Richards & Scott, 2002). Nevertheless, some studies have shown that patients tend to present poor adherence to different exercise recommendations, even walking (Dobkin, Abrahamovicz, Fitzcharles, Dritsa & Costa, 2005; Dobkin, Da Costa et al., 2006; Meyer & Lemley, 2000; Schachter et al., 2003).
Walking, as a way to exercise, is a self-regulated behaviour, and therefore, is susceptible to being explained by the current psychosocial models. Physical activity has been associated to the intention to carry it out (Hagger, 2010). Theory of Planned Behaviour (TPB) (Ajzen, 1985, 1991; Ajzen & Madden, 1986; Fishbein & Ajzen, 2010) has been shown to be able to predict intentions and behaviours associated to physical exercise in general (Hagger, Chatzisarantis & Biddle, 2002; Symons-Downs & Hausenblas, 2005) and to walking in particular (Darker, French, Eves & Sniehotta, 2009; Galea & Bray, 2006; Rhodes, Brown & McIntyre, 2006). Also, it is one of the most popular psychosocial models in the literature about prediction of social behaviours (Ajzen, 2011). In opposition to other models that have also shown good predictive power about health behaviours, this is the one that is most frequently used to study walking behaviour (at least in non-clinical populations). In relation to the intentions to carry out physical exercise, the average of explained variance by the three predictive constructs of TPB is 44.5% (Hagger et al., 2002) and in relation to the intention to walk, in some studies conducted on populations with health problems, the explained variance is of 67% (Galea & Bray, 2006). Nevertheless, in spite of its predictive potential, there is little research using this theory in the context of people with health issues related to chronic pain. In the literature we have reviewed about its application in fibromyalgia, we found no studies that use it to predict the intention and the carrying out of walking behaviours. Thus, as part of a larger study which aims to increase this behaviour in people with fibromyalgia combining motivational and volitional intervention, we have chosen to work with the TPB due to its parsimony and potential in predicting intention (motivational intervention) of performing behaviours associated to physical exercise, amongst them, walking.
TPB (Figure 1) proposes that the immediate determinant of the performance of a behavior is the intention that the person has to do it (behavioural intention). Intention is determined by the attitude towards the behaviour (global assessment of the positive and negative consequences associated to carry out the behaviour), the subjective norm (social pressure perception to carry out the behaviour) and perception of control (perceiving that the behaviour is under control). The perception of control can also have a direct effect on the behaviour, not needing to be mediated by intentions.
In the recent formulation of the model (Fishbein & Ajzen, 2010), the authors consider that there are two aspects that are associated to the perception of social pressure or social norm, which they have named 'injunctive norm' and 'descriptive norm'. The first aspect involves the more classical perspective of the construct (the perception that the important referents think that the person should or should not carry out the behaviour) and the second adds the idea that observation of the behaviour of models with which the person identifies with is another way of perceived social pressure.
The attitude, the subjective norm and the perception of control are determined, respectively, by behavioural beliefs (expected consequences of carrying out behaviour along with the positive or negative assessment it), normative beliefs: injunctive (the perception that important referents want the person to carry out the behaviour along with the motivation to comply with them) and descriptive (the perception that the referents are carrying out the behaviour as well as the degree in which person identifies with the referent) and, finally, the control beliefs (facilitators and inhibitors of the accomplishment of the behaviour, along with the assessment of their facilitating or inhibiting power). Salient beliefs are the ultimate determinants of intention and behaviour, and they influence through attitude, subjective norm and control perception. Therefore, they are the target of the interventions to generate behavioural change.
To implement an intervention based on TPB, it is necessary to have two previous phases of 'formative research' (Fishbein & Ajzen, 2010). The first phase consists of undertaking a pilot study with four aims: to identify beliefs (using a qualitative study), to know the status of the sample in relation to the behaviour the intervention is aimed at, to test the items designed to measure attitude, subjective norm, control perception and intention and to test the relationships between the predictive constructs and the previous behaviour as an indicator for future behaviour (quantitative study) (Fishbein & Ajzen, 2010, pp. 326-328). Based on these results, a questionnaire is designed in the second phase, which is applied to a representative sample of the target population.
In spite of the importance that identification of beliefs has in this theory, most of the studies about physical exercise concentrate on the predictive relationships that attitude, subjective norm and control perception have on intention and behaviour, without having analysed the underlying beliefs (Darker et al, 2009; De Bruijn & Rhodes, 2011; Hagger et al., 2002; Symons-Downs & Hausenblas, 2005). In fact, some authors have called attention on the lack of studies in this area (Darker, French, Longdon, Morris & Eves, 2007; Symons-Downs & Hausenblas, 2005). When TPB is used as a reference model in order to promote behavioural change, it is imperative to develop a study to identify beliefs about the target behaviour in the population of interest. In first place, due to them being the target of the intervention, and in second place, because specificity is being assumed, and thus, variability based on the two previously mentioned elements, behaviour and population (Ajzen & Fishbein, 1980; Fishbein & Ajzen, 2010). In spite of this, in the research we have found about walking, we found few studies indentifying beliefs following the TPB model (Darker, French et al., 2007; Rhodes et al., 2006) and another where a phenomenological analysis has been performed (Darker, Larkin & French, 2007). In all three studies, participants were taken from general population. As already mentioned, we do not find any studies that apply TPB to predict walking as exercise in patients with fibromyalgia or chronic pain.
One of the most important aspects in TPB is the specification of the behavioural criterion. To achieve this, the authors suggest that there should be four elements included: action, aim, context and time. The behaviour, defined considering the previously mentioned elements, should remain without any modifications during the assessment of all constructs of the theory (the principle of behavioural compatibility). In relation to walking, one of the recommendations for fibromyalgia patients is that they should do it between 2 and 4 times a week, for about 50 minutes, in bouts of 15 to 20 minute (with a small rest between bouts to allow patients delay fatigue and continue the activity) for a minimum of 6 consecutive weeks (Gusi, Parraca, Adsuar & Olivares, 2009). Following recommendations about the prescription of exercise in fibromyalgia (Jones & Liptan, 2009; Mannerkorpi & Iversen, 2003; Meyer & Lemley, 2000) we reduced the minimum time established in the previously described recommendation. Therefore, the target behaviour for our study is, with the aim to exercise for own health care, 'to walk for at least 30 minutes, in bouts of 15 minutes, with a small rest between bouts, twice a week for a minimum of 6 consecutive weeks'.
The current study is the first stage of the formative research as indicated by TPB and developed with a pilot study. Our aims are: 1. To identify the behavioural, normative and control beliefs about the carrying out of the chosen behaviour ('elicitation study'). 2. To analyse the items created to directly assess the attitude, subjective norm, perception of control and the behavioural intention, 3. To explore the relations between the constructs and 4. To get better knowledge of the situation of the sample in relation to the chosen behaviour.
Method
Participants
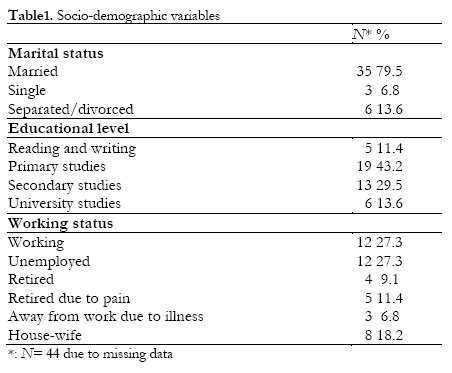
We contacted 50 women from four fibromyalgia associations from Alicante, Elche, Madrid and Talavera de la Reina. 46 of the women attended the assessment groups (92%). Average age was 54.2 year (SD= 8.9; CI 95% [54.21, 51.47]) and average score on pain intensity was 6.7 (SD= 1.3; CI 95% [6.28-7.08]). Most of them were married or lived with a partner (79.5%), had primary studies (44.2%) and working status was quite variable (Table 1).
47.8% (n= 22) of the participants did not walk and the rest do it incorrectly, according to our specifications (Gusi et al., 2009): once a week (n= 3; 6.5%), not regularly (n= 9; 19.6%), with a break after 15 minutes (n= 1; 2.2%) and with no breaks (n= 3; 6.5%). Eight people (17.4%) had changed their walking habits in the past three months (see procedure) and did walk correctly. We decided to maintain them in the study due to the intra-individual variability in the fibromyalgia presentation of symptoms. The 75% reported having received medical recommendations to walk.
Variables and instruments
Pain intensity: We assessed for highest, lowest and average pain intensity for the week before assessment, as well as the pain intensity during assessment. All four items were answered using a scale of 11 points (0=no pain; 10=the highest pain you can imagine). This scale has shown good psychometric properties in patients with fibromyalgia (Marttn-Aragon et al., 1999; Lledó et al., 2010). Internal consistency for this sample was alpha= .77.
Exercise: Using five multiple answer items, we asked about the number of days the person was walking as exercise, the amount of time this was done continually, the time dedicated to the activity each time it was carried out and the rests taken. The answers available included the different elements of the walking behaviour we aimed to study. Finally, using a dichotomic response, we asked about the existence or not of medical recommendation to exercise. This scale was only used to identify eligible participants (see procedure).
TPB: beliefs
So as to identify the beliefs about the carrying out of the behaviour we designed eight questions with open answers following the recommendations of the authors (Fishbein & Ajzen, 2010). Questions used are presented in Appendix 1, pp 7-10.
Behavioural beliefs: We designed questions about the advantages and disadvantages of carrying out the behaviour and also another general question ("Is there any consequence that comes to mind when you think about ...?").
Normative beliefs: We designed three questions for each norm, seeking information about the person's important referents, either because they believed that they would support or not the behaviour being carried out (injunctive norm; i.e.: "What people or groups would be in favour of you walking...?") or either because they thought they would do the behaviour if they were in their place (descriptive norm; i.e.: What people or groups would walk if they had the same problem as you ...?").
Control beliefs: We created two questions to identify the perceived facilitators and inhibitors in relation to the carrying out of the behaviour (what things would help ...? What things would make it harder...?).
All questions could be answered on a maximum of six lines, but if necessary the respondents could continue their answers on the back of the page.
TPB: previous behaviour, intention, attitude, subjective norm, perception of control
All five of the following variables were assessed using the average scores on each of the scales. They were all answered on a seven point scale, in which the extremes (1-7) varied depending on the content of the item (Appendix 1). Internal consistency data for the scales are reported in the results section.
Behaviour: Using four items we assessed previous behaviour (i.e.: "In the past month and a half how often have you walked at least...?'). Higher scores indicate higher performance of the behaviour.
Behavioural intention: We designed five items (i.e.:"I intend to walk at least...") so as to assess the intentions. In spite of the controversy between behavioural expectation, intention and disposition to act, we considered the different formulations as ways to measure a single construct (Fishbein, 2008; Fishbein & Ajzen, 2010). A higher score indicates a stronger intention to walk in the terms we had specified.
Attitude towards the behaviour: We designed nine pairs of bipolar adjectives that considered instrumental (i.e.: "Good-Bad") and experiential aspects (i.e.: "Nice-nasty") about the attitudinal assessment of the behaviour. We recoded the necessary answers so that a higher score indicated a favourable attitude.
Subjective Norm: Using three items we assessed injunctive norm (i.e.: "Most people whose opinions I appreciate think that I should walk." ) and with three additional ones we assessed descriptive norms (i.e.: "Most people with this health problem walk." ). We obtained three average scores, one for each type of norm and one for the total. In all three, a higher score indicated a stronger perceived social pressure.
Perceived behavioural control: This scale included a larger number of items (n=11) because, as well as the ones associated to the global assessment of perceived control (i.e.: "Walking depends completely on myself..."), we also included others that assessed self-efficacy perception, considering the possible inhibiting factors that are associated to fibromyalgia that could be influencing real control, such as fatigue, pain or mood (i.e.: ""In spite of my pain, if I really want to, I can walk ..."). With this we attempted to get a better picture of control in relation to the behaviour. A higher score indicated a stronger control perception.
Procedure
This study is part of a larger one that aims to design an intervention using TPB to increase unsupervised physical exercise (walking) in people with fibromyalgia. The current study is the first stage of the formative research of TPB, and was developed using a pilot study in the population at whom the intervention is aimed. The eligible population (n=582) was previously selected amongst the total population associated (n=2438) according to our selection criteria: female, between the ages of 18 and 70, that fulfils the London-4 criteria (White, Harth, Speechley & 0stbye, 1999; Branco et al., 2010) and that does not walk for exercise despite being able to do so (there is no comorbid problem that hinders the ability to walk or they have been medically recommended to do so) or in spite of walking they do not fulfil some of the criteria established in the behaviour selected for the study.
In TPB the recommended number of participants for a pilot study of this type is between 25 (Francis et al., 2004; Godin & Kok, 1996) and 30 people (Fishbein & Ajzen, 2010); as our sample belonged to four different associations, we selected 10 people randomly from three of them and 20 from the largest (Madrid), over the phone to meet. Therefore we included a total of 50 women that fulfilled the criteria mentioned above to be part as they were from the eligible population.
During the assessment session they all signed informed consent forms, including an authorization to film their group discussions. First, the participants answered their questionnaires individually and later, in a group, they discussed their answers to the open questions. In this manner, as Fishbein & Ajzen (2010) recommend, we were able to identify individual beliefs and we avoided having some people influence other's response's accessibility and creation. Furthermore, in the group discussion, we reinforced the assistance by exchanging their opinions on the matter and we used the transcripts to increase understanding of certain ambiguous answers given on the individual response sheets.
Creation and application of the instrument
The questionnaire contained two sections: one with 35 items designed to assess the predictive constructs and the other with 8 open answer questions to identify beliefs (Appendix 1). In relation to this second section, we followed the recommendations set by Fishbein & Ajzen (2010) so first we presented the questions to identify behavioural beliefs, followed by the normative and control beliefs; this was because it has been shown that there is no effect of order on the number and type of beliefs identified (Darker, French et al., 2007).
As for the other questions, two researchers from the Alicante team, who are well versed in the theory and its applications in health, designed a total of 35 items following the recommendations and indications in the available literature (Ajzen, 2006; Francis et al., 2004; Fishbein & Ajzen, 2010).
Following this, the questions were revised by the rest of the team in Madrid (all of whom have ample clinical and research experience in fibromyalgia) and in a group session all suggestions were put together. All four researchers that assessed the items had access to a written abstract about research in TPB authored by the head researcher as well as access to the content of the constructs. Their task was to assess if the items that had been suggested correctly reflected the corresponding construct, if the writing was understandable and if the scale provided to answer was adequate. As a result, the writing on some of the items was modified, so as to be simplified, and the coding for some answers also changed, it was changed from -3 to +3 to a scale from 1 to 7, due to the difficulties encountered by the researchers involved in other studies with fibromyalgia when using the former format. No items were deleted.
In summary, the questionnaire designed in this phase, contained 8 questions with open-format answers to identify beliefs and 35 questions to assess previous behaviour, intention, attitude, subjective norm and control perception.
Content analysis for identification of beliefs
We selected the modal beliefs (beliefs most frequent in a population) using a content and frequency analysis of each. We maintained the separation between associations up to the moment of the final selection of beliefs that were going to be part of the final questionnaire (result of this study). In this way, we could identify the specificity or not of the belief, and as we will present, use it as a deciding criterion. The sequence of the analysis was as follows:
1. Literal transcription of the answers to the open questions of the questionnaire and the recordings.
2. Grouping and registration of frequencies of answers with similar content but with different grammatical formulations, considering also their valence (i.e.: '...I would return less tired...', '...I would return more tired...', 'I would be more exhausted'). When the answers with opposing valence were voiced by the same individual we decided to count them in only once in the most numerous group of valence of the answers.
3. Grouping and recording the frequency of answers with related content (i.e.: 'my mood would improve', 'I would feel happier', 'my psychological health would improve'). We counted the frequency of each group (adding up of the number of individual beliefs that form it), maintaining the frequency of each valence separate and tagging the group with a phrase that represents the individual beliefs that were contained in it. To do this, we considered the grammatical formulation of valence most frequently used in the block and we attempted to recreate the language used by the participants in the session.
4. Selection of the modal beliefs that will be included in the final questionnaire following a frequency criterion (25% of the sample: n=11). With beliefs below this number, we considered a second criterion of clinical and theoretical relevance, based on our knowledge of fibromyalgia and supported by the transcripts of the discussion groups; based on this criterion, the belief also had to be present in at least three of the associations included.
Three researchers organized and revised the information following these steps; after this, the material was sent to the rest of the team to identify their degree of agreement (100%).
Statistical analysis for the study of the items that assess the remaining constructs
We performed an item analysis by studying the floor effect (percentage of response below 5%) and ceiling effect (percentage of response above 95%), we applied this to the groups of extreme response values for each item; we also analysed the discriminating validity and internal consistency of the scales (Fishbein & Ajzen, 2010). We deleted the items that reduced internal consistency of the corresponding scale; after this, with the items of the scales that assess the constructs at a predictive level (behavioural attitude, subjective norm and perception of control) we studied the correlations between the items that remained in the scale with the total corrected score for each and as well as with the other scales that assess the mentioned constructs. Those items that had higher significant correlations with the total score on a scale which they did not belong were removed. In this last analysis we did not consider the scales for intention or behaviour as these are constructs that are to be predicted by the others, and according to the theory, it is expected to find high significant correlations with them. Although the theory also admits certain relations between the three constructs above mentioned, these are not expected to be high. Finally, we explored the relations between the constructs of the theory (except the beliefs). Using SPSS version 21, we performed the descriptive, internal consistency (Cronbach's Alpha) and relations analysis (Pearson's correlation).
Results
Identification of beliefs
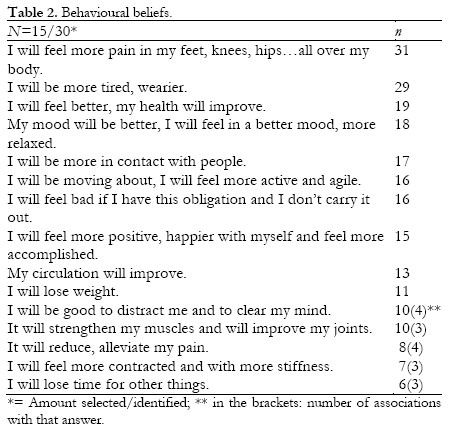
Behavioural Beliefs
Four people from one association found no advantages to carrying out the behaviour and 11 from different associations only found advantages. The average number of beliefs obtained per person was 5.8 (SD= 2.95; ranging from 1-12; Median= 6; Mode= 7). Out of the 30 beliefs identified we selected 15, following the criterion described in the previous section (Table 2).
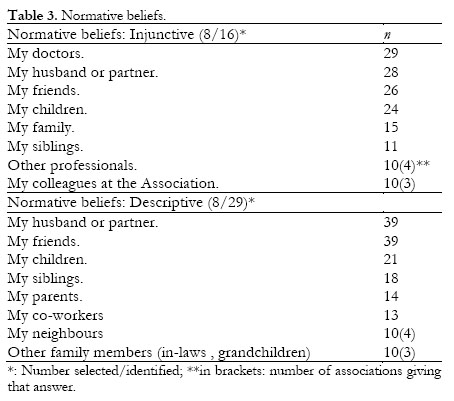
Normative Beliefs
We identified a larger number of referents in favour of the person with fibromyalgia doing the behaviour (90.4%) and that, also, the patient perceives that they would carry out the behaviour if they were in their place (74.2%). The average number of normative beliefs of both types per person was 8.63 (SD= 3.76; ranging from 0-16; Median= 8.5; Mode: 8). We selected 8 referents for each type of normative belief (Table 3).
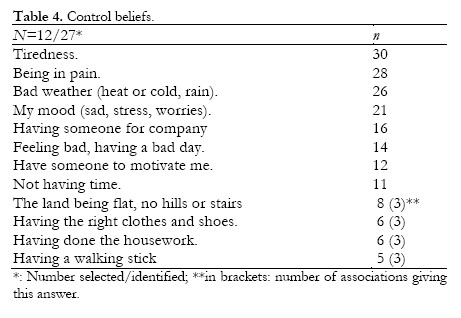
Control Beliefs
The average number of beliefs obtained per person was 4.84 (SD= 2.48; ranging from 0-12; Median= 5; Mode= 5). 50% of the answers selected were behavioural facilitators (Table 4).
Item Analysis
We found only one floor effect for one item in the injunctive norm scale ('Most of the people important to me think...') where response frequencies to alternatives 1 and 2 added up to 4.6%.
The items on the behaviour scale had answers on all 7 response options, 6 in the case of the subjective norm, control and intention and 5 for attitude. We obtained certain asymmetry for two items on the intention scale ('I will make an effort to walk...'=-1.6 and 'I am prepared to walk...'=-1.5), one for control (It depends completely on me ...'=-1.5) and three for subjective norm (the largest asymmetry: 'Thepeople whose opinions I appreciate think that I should...'=-1.7). We found asymmetry in all attitude items, with the largest being for the 'Harmful-Beneficial' pair (-2.2).
Except for intention and subjective norm (descriptive), in the other scales internal consistency increased deleting one item (Table 5). Values oscillated between alpha=.78 (subjective norm) and alpha=.94 (injunctive norm and perception of control). All correlation coefficients of item-total were above .50, except for the deleted items (except in the case of item 3 from the injunctive norm: r=.57).
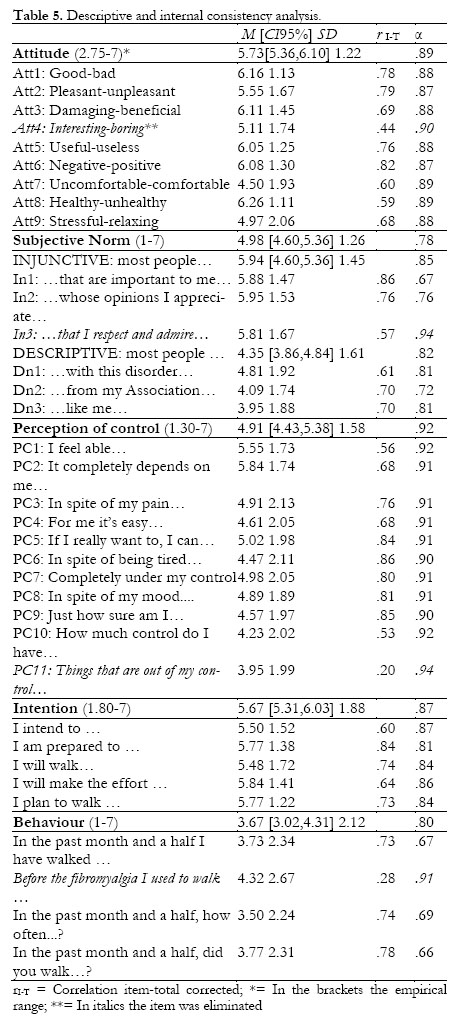
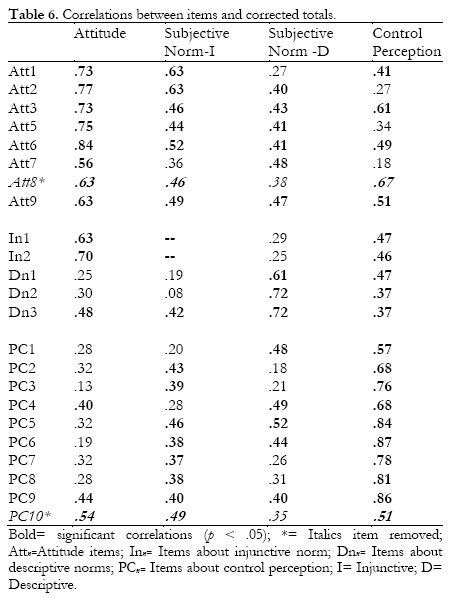
In the correlation analysis of the items with the total corrected score (eliminating the item) we expected higher correlations with the score on the scale the item belongs to. We deleted the item 'Healthy-Unhealthy' from attitude and 'How much control do you have over walking...?' from the perception of control, because they presented higher correlations with total scores of control and attitude scales, respectively (Table 6). Internal consistency of the scales remained within the initial values.
We found significant correlations between previous behaviour and intentions (r = .34, p<.03) and perception of control (r = .32, p<.04). Intention was associated significantly to perception of control (r = .70, p<.000), attitude (r = .56, p < .000) and total subjective norm (r = .45, p <.002).
Discussion
This study is the first phase of a formative research as recommended by Fishbein & Ajzen (2010) to design and apply an intervention based on TPB. Thus, our aims have been to identify behavioural, normative and control beliefs about the carrying out of our target behaviour, to test the items designed for the assessment of the theoretical constructs and explore their relations, as well as to gather knowledge on the situation of our sample in regards to walking behaviour. All this has been done as an indicator of pertinence for applying the theory to this population and the selected behaviour.
As we have previously mentioned, beliefs constitute accessible information that is relevant to the behaviour that we are planning to implement and on which we will be targeted to produce behavioural change. This study identifies the most frequent in the population selected (modal beliefs). It is the first of its type in people with fibromyalgia and that, also, uses a type of exercise recommended for them. As for the behavioural beliefs, most of the perceived consequences associated with walking, according to our criteria, are positive and refer to global functioning physical and psychological aspects. Nevertheless, the two most frequently detected consequences are negative and refer to two of the main problems of fibromyalgia: pain and fatigue. We should point out that the increase of pain as a negative effect refers to different body parts where pain can be produced as a result of walking. Nevertheless, when pain relief appears as a positive consequence of walking, it refers to general fibromyalgia pain and its frequency is low. This means that with the carrying out of the recommended exercise, the people we assessed do not expect to have positive effect on the main problem of their disorder.
We obtained a majority of referents (normative beliefs) in favour of the person doing the exercise, with the most relevant being partners and friends, who appear as such in both injunctive and descriptive normative beliefs. Doctors and other professionals are only referents for injunctive norms, which is logical, and also supports content validity. Nevertheless, it is interesting that the colleagues from the association are referents only for injunctive norms. This means that the people assessed in this study, do_not believe that their colleagues, who share the same disorder, are going to carry out the behaviour, although they would be in favour of them carrying it out.
Finally, in the case of control beliefs, we have obtained a similar proportion of facilitating and inhibiting factors for the carrying out of the behaviour. As it was expected, except for external conditions such as the weather, the most frequently perceived inhibitors are related to problems of the fibromyalgia, such as fatigue, pain and mood. The most frequently found facilitators are associated to social support, but not associated to any specific referents (someone comes with me, someone motivates me).
In general terms, our results coincide with those obtained by other authors about walking in general population (Darker, French et al., 2007; Rhodes et al., 2006) or about other types of physical exercise in different populations (Symons-Downs & Hausenblas, 2005). In our study, the tendency to show a higher number of positive beliefs than negative about these behaviours is confirmed, our findings about the average number of behavioural, normative and control beliefs is similar to that found in other populations (Symons-Downs & Hausenblas, 2005). It should be highlighted that in spite of the clear differences between samples (in our case a population with a health problem) the increase in physical and psychological health is on the of most frequently pointed out positive consequences, different members of family and friends are important referents for these behaviours and not having time available or weather are elements that hinder the carrying out of the behaviour (Darker, French et al., 2007; Rhodes et al., 2006; Symons-Downs & Hausenblas, 2005). Nevertheless, the presence of pain (in different parts of the body) has been the most frequent negative behavioural belief found in our study. Also, the other most frequent inhibitors have been pain and fatigue (control beliefs). These results are in accordance with the review authored by Symons-Downs & Hausenblas (2005) where pain, physical ill-being and other physical problems were the most frequently identified behavioural and control beliefs. It should be pointed out that these authors included studies in ill populations in their study (i.e., oncological and cardiovascular problems) whilst Darker, French et al. (2007) and Rhodes et al. (2006) only included general population. Because of this, it is of great importance to identify the specific beliefs a target population has, because differences are expected based on their characteristics and experiences. In this sense, in the case of chronic pain patients, factors such as pain catastrophizing, fear of pain and coping mechanisms, which have all been associated to pain perception (Ramírez, Esteve & López, 2001) could be influencing the carrying out of the behaviour. Nevertheless, their action is always mediated through the configurations of certain beliefs about the relevant symptoms, such as pain and fatigue.
In relation to the quantitative study, a clear limitation is sample size; nevertheless, it is above the minimum size requirements needed to attain the aims of this phase (Fishbein & Ajzen, 2010; Francis et al., 2004). The items analysis results have concluded with the deletion of six of them and have proven the adequacy of the remaining. Most of them have obtained answers in all or almost all the possible options and do not present any floor or ceiling effects. Discriminant validity was adequate, with correlations with selected items with the corrected total of the scales of .50 and above the ones obtained with the scales that assess a different construct. Internal consistency was very good for all scales (Bisquerra, 1987). Although initial alpha values were high, we deleted items that increased them so as to shorten the questionnaire and reduce completion time, which is an important aspect in this population due to the presence of physical symptoms such as pain. All scales remained configured with the minimum number of items suggested by Fishbein & Ajzen (2010) with the exception of the one assessing injunctive norm, which only had two. Nevertheless, considering internal consistency data, and that the authors recommend using unitary constructs (total subjective norm, without components) for the predictive analysis, it is recommended that a single scale is created to assess subjective norm with all five items.
Other aims of this phase of the study are to assess behavioural intention, obtain preliminary estimations about their relation to previous behaviour (considering it as a measure proxy to future behaviour) and to explore the relations to the other constructs according to the theoretical proposals (Fishbein & Ajzen, 2010). In general, taking into account the average scores, these people have the intention to carry out the behaviour, their attitude is favourable and they perceive a certain amount of social pressure to do it. The lowest average scores are for perception of control and the perception that other people in their same situation do the behaviour (descriptive norm). This is relevant to perception of control as it is the construct most strongly related to the intention to walk, which is in accordance to previous studies in general population (French, Darker, Eves & Sniehotta, 2013) and clinical population (Galea & Bray, 2006). Nevertheless, in Hagger et al. (2002) review about general physical activity in populations with no health problems, attitude was the most important construct for intention. These preliminary relationships will be tested in the study population eligible for intervention. Finally, it should be pointed out that the configuration of the relations obtained in our study support its theoretical coherence; this, along with the carrying out of the selected behaviour, indicates the importance of working in fibromyalgia with the proposed theory.
In summary, the results support the application of this theory on the chosen behaviour and population. Also, we have been able to identify modal beliefs about a certain type of exercise in people with fibromyalgia that do not currently carry it out, so as to be included as items in the final questionnaire, and finally, we have proven the items and refined the scales that assess the remaining constructs. Thus, this study has allowed the creation, based on evidence, of an instrument that includes all constructs of the selected theory, so as to be applied to the chosen population.
References
1. Ajzen, I. (1985). From intentions to actions: A theory of planned behavior. En J. Kuhl & J. Beckman (Eds.), Action control: From cognitions to behavior. Berlin: Springer. [ Links ]
2. Ajzen, I. (1991). The theory of planned behavior. Organisational Behavior and Human Decision Processes, 50, 179-211. [ Links ]
3. Ajzen, I. (2006). Constructing a theory of planned behavior questionnaire. Retrieved from http://people.umass.edu/~aizen/pdf/tpb.measurement.pdf. [ Links ]
4. Ajzen, I. (2011). The theory of planned behavior: Reactions and reflections. Psychology & Health, 26, 1113-1127. [ Links ]
5. Ajzen, I., & Fishbein, M. (1980). Understanding attitudes and predicting social behavior. Englewood Cliffs, NJ: Prentice-Hall. [ Links ]
6. Ajzen, I., & Madden, T. J. (1986). Prediction of goal directed behavior: Attitudes, intentions, and perceived behavioral control. Journal of Experimental Social Psychology, 22, 453-474. [ Links ]
7. Bisquerra, R. (1987). Introducción a la estadística aplicada a la investigatión educativa. Barcelona: PPU. [ Links ]
8. Branco, J. C., Bannwarth, B., Failde, I., Abello, J., Blotman, F., Spaeth, M., ... Matucci-Cerinic, M. (2010). Prevalence of Fibromyalgia: A Survey in Five European Countries. Seminars in Arthritis and Rheumatism, 39, 448-453. [ Links ]
9. Busch, A., Schachter, C., Overend, T., Peloso, P., & Barber, K. (2008). Exercise for fibromyalgia: a systematic review. Journal of Rheumatology, 35, 1130-44. [ Links ]
10. Carmona, L., Ballina, F. J., Gabriel, R., Laffon, A., & EPISER study group (2001). The burden of musculoskeletal diseases in the general population of Spain: results from a national survey. Annals of Rheumatic Diseases, 60, 1040-1045. [ Links ]
11. Darker, C., French, D., Eves, F., & Sniehotta, F. (2009). An intervention to promote walking amongst the general population based on an 'extended' Theory of Planned Behaviour: A waiting list randomized controlled trial. Psychology & Health, 25, 71-88. [ Links ]
12. Darker, C., French, D., Longdon, S., Morris, K., & Eves, F. (2007). Are beliefs elicited biased by question order? A Theory of Planned Behaviour belief elicitation study about walking in the UK general population. British Journal of Health Psychology, 12, 93-110. [ Links ]
13. Darker, C., Larkin, M., & French, D. (2007). An exploration of walking behavior. An interpretative phenomenological approach. Social Science & Medicine, 65, 2172-2183. [ Links ]
14. De Bruijn, G. J., & Rhodes, R. E. (2011). Exploring exercise behavior, intention and habit strength relationships. Scandinavian Journal of Medicine and Sciences in Sports, 21, 482-491. [ Links ]
15. Dobkin, P., Abrahamovicz, M., Fitzcharles, M., Dritsa, M., & Da Costa, D. (2005). Maintenance of exercise in women with Fibromyalgia. Arthritis Care & Research, 53, 724-731. [ Links ]
16. Dobkin, P., Da Costa, D., Abrahamovicz, M., Dritsa, M., Berger, R. Fitzcharles, M., & Lowensteyn, L. (2006). Adherence during an Individualized Home Based 12-Week Exercise Program in Women with Fibromyalgia. Journal of Rheumatology, 33, 333-41. [ Links ]
17. Dobkin, P., Sita, A., & Sewitch, M. (2006). Predictors of adherence to treatment in women with Fibromyalgia. Clinical Journal of Pain, 22, 286-294. [ Links ]
18. Fishbein, M. (2008). A Reasoned Action Approach to health promotion. Medical Decision Making, 28: 834. Doi: 10.1177/0272989X08326092. [ Links ]
19. Fishbein, M., & Ajzen, I. (2010). Predicting and changing behavior. The Reasoned Action Approach. New York: Taylor & Francis. [ Links ]
20. Francis, J., Eccles, M., Johnston, M., Walker, A., Grimshaw, J., Foy, R., ... Bonetti, D. (2004). Constructing questionnaires based on the theory of planned behavior. A manual for health services researchers. Centre for Health Services Research. University of Newcastle. Recuperado de http://openaccess.city.ac.uk/1735/. [ Links ]
21. French, D., Darker, C., Eves, F., & Sniehotta, F. (2013). The systematic development of a brief intervention to increase walking in the general public using an "extended" theory of Planned Behavior. Journal of Physical Activity & Health, 10, 940-948. Retrieved from http://journals.humankinetics.com/journal-authors/journal-authors/david-paul-french. [ Links ]
22. Galea, M. N., & Bray, S. R. (2006). Predicting walking intentions and exercise in individuals with intermittent claudication: An application of the Theory of Planned Behavior. Rehabilitation Psychology, 51, 299-305. [ Links ]
23. Godin, G., & Kok, G. (1996). The Theory of Planned Behavior: a review of its applications to health-related behaviours. American Journal of Health Promotion, 11, 87-98. [ Links ]
24. Gusi, N., Parraca, J., Adsuar , J. & Olivares, P. (2009). Ejercicio físico y Fibromialgia. En A. Penacho, J. Rivera, M. Pastor & N. Gusi (Eds.), Guía de ejercicios físicos para personas con Fibromialgia (pp. 39-56). Vitoria: Asociación Divulgación Fibromialgia. [ Links ]
25. Hagger, M. (2010). Current issues and new directions in Psychology and Health: Physical activity research showcasing theory into practice. Psychology & Health, 25, 1-6. [ Links ]
26. Hagger, M., Chatzisarantis, N., & Biddle, S (2002). A meta-analytic review of the theories of Reasoned Action and Planned Behavior in Physical Activity: Predictive validity and the contribution of additional variables. Journal of Sport & Exercise Psychology, 24, 3-32. [ Links ]
27. Häuser, W., Klose, P., Langhorst, J., Moradi, B., Steinbach, M., Schiltenwolf, M., & Busch, A. (2010). Efficacy of different types of aerobic exercise in fibromyalgia syndrome: a systematic review and meta-analysis of randomised controlled trials. Arthritis Research & Therapy, 10:R79. [ Links ]
28. Häuser, W., Thieme, K., & Turk, D. (2010). Guidelines on the management of fibromyalgia syndrome. A systematic review. European Journal of Pain, 14, 5-10. [ Links ]
29. Jones, K. D., & Liptan, G. L. (2009). Exercise Interventions in Fibromyalgia: Clinical applications from the Evidence. Rheumatic Disease Clinics of North America 35, 373-391. Doi:10.1016/j.rdc.2009.05.004. [ Links ]
30. Lledó, A., Pastor, M.A., Pons, N., López-Roig S., Rodríguez-Marín, J., & Bruehl, S. (2010). Control beliefs, coping and emotions: Exploring relationships to explain fibromyalgia health outcomes. International Journal of Clinical and Health Psychology, 10, 459-476. [ Links ]
31. Mannerkorpi, K., & Iversen M. D. (2003). Physical exercise in fibromyalgia and related syndromes. Best Practice Research in Clinical Rheumatoly, 17, 629-647. [ Links ]
32. Martín-Aragón, M., Pastor, M. A., Rodríguez-Marín, J., March, M. J., Lledó, A., López-Roig, S. & Terol, M. C. (1999). Percepción de autoeficacia en dolor crónico: adaptación y validación de la Chronic Pain Self-Efficacy Scale. Revista de Psicología de la Salud, 11, 53-75. [ Links ]
33. Meyer, B. B., & Lemley, K. J. (2000). Utilizing exercise to affect the symptomatology of fibromyalgia: a pilot study. Medical Sciences & Sports Exercise, 32, 1691-1697. [ Links ]
34. Ramírez, C., Esteve, R. & López, A. (2001). Neuroticismo, afrontamiento y dolor crónico. Anales de Psicología, 17, 129-137. [ Links ]
35. Rhodes, R. E., Brown, S. G., & Mclntyre, C. A. (2006). Integrating the perceived neighbourhood environment and the theory of planned behaviour when predicting walking in a Canadian adult sample. American Journal ofHealth Promotion, 21, 110-118. [ Links ]
36. Richards, S., & Scott, D. (2002). Prescribed exercise in people with fibromyalgia: parallel group randomised controlled trial. British Medical Journal, 27, 7357-185. [ Links ]
37. Rivera, J., Alegre, C., Nishishinyac, M. B. & Heredad, C.A. (2006). Evidencias terapéuticas en fibromialgia. Reumatología Clínica, 2, 34-37. [ Links ]
38. Rivera, J., Rejas, J., Esteve-Vives, J., Vallejo, M. A., & Grupo ICAF (2009). Resource utilisation and health care costs in patients diagnosed with fibromialgia in Spain. Clinical and Experimental Rheumatology, 27, S39-S45. [ Links ]
39. Rooks, D., Gautam, S., Romeling, M., Cross, M., Stratigakis, D., Evans, B., ...Katz, J. (2007). Group exercise, education, and combination self-management in women with fibromyalgia: a randomized trial. Archives of Internal Medicine, 167, 2192-2200. [ Links ]
40. Schachter, C., Busch, A., Peloso, P., & Sheppard, M. (2003). Effects of short versus long bouts of aerobic exercise in sedentary women with Fibromyalgia: A Randomized Controlled Trial. Physical Therapy, 83, 340-358. [ Links ]
41. Sicras-Mainar, A., Rejas, J., Navarro, R., Blanca, M., Morcillo, A., Larios, R., ... Villarroya, C. (2009). Treating patients with Fibromyalgia in primary care settings under routine medical practice: a claim database cost and burden of illness study. Arthritis Research & Therapy, 11 (R54). Doi:10.1186/ar2673. [ Links ]
42. Symons-Downs, D., & Hausenblas, H. (2005). Elicitation studies and the Theory of Planned Behavior: a systematic review of exercise beliefs. Psychology of Sports & Exercise, 6, 1-31. [ Links ]
43. Van Koulil, S. V., Effting, M., Kraaimaat, F. W., van Lankveld, W., van Helmond, T., Cats, H., ... Evers, A. (2007). A review of cognitive behaviour therapies and exercise programmes for Fibromyalgia patients: state of the art and future directions. Annals of Rheumatic Diseases, 66, 571-581. [ Links ]
44. White, K. P., Harth, M., Speechley, M., & Østbye, T. (1999). Testing an instrument to screen for Fibromyalgia Syndrome in general population studies: The London Fibromyalgia Epidemiology Study Screening Questionnaire. Journal of Rheumatology, 26, 880-884. [ Links ]
45. Wolfe, F., Smythe, H., Yunus, M., Bennett, R. M., Bombardier, C., Goldenberg, D. L., ... Sheon, R.P. (1990) . The American College of Rheumatology 1990 criteria for the classification of Fibromyalgia: Report of the multicenter criteria commitee. Arthritis & Rheumatism, 33, 160-172. [ Links ]
![]() Correspondence:
Correspondence:
Ma Angeles Pastor
Departamento de Psicologia de la Salud
Universidad Miguel Hernandez
Campus de San Juan
Ctra. Alicante-Valencia, Km. 8,7
03550 San Juan, Alicante (Espaha).
Email: mapastor@umh.es
Article received: 28-03-2013
Revised: 24-11-2013
Accepted: 20-05-2014

