










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkThe European Journal of Psychiatry
versión impresa ISSN 0213-6163
Eur. J. Psychiat. vol.19 no.4 Zaragoza oct./dic. 2005
Premorbid adjustment and previous personality in schizophrenic patients
| José Juan Rodríguez Solano, M.D.* Manuel González de Chávez, M.D.** * Psychiatry and Mental Health Service in Vallecas, Madrid |
Key words: Schizophrenia, Premorbid adjustment, Personality disorders, Vulnerability, Neurodevelopment.
ABSTRACT Psychosocial adjustment and premorbid personality are two factors that are frequently studied in order to elucidate the etiopathogenesis of schizophrenia. Premorbid adjustment alterations and personality disorders (principally those of the schizophrenia spectrum) have been considered vulnerability elements or have been linked with the early manifestations of a disease that is still underdeveloped (hypothesis of neurodevelopment).
In this paper we review the literature. We also studied the relationship between premorbid adjustment (PAS scale) and previous personality disorders (SCID-II) in a sample of 40 patients with schizophrenia (DSM-III-R, DSM-IV, CIE-10), and statistically correlated them.
The results show that premorbid adjustment correlates with avoidant, schizotypal and schizoid personality disorders: the more personality pathology found, the poorer is the premorbid psychosocial adjustment. Premorbid adjustment positively correlates with histrionic personality traits. The pathological traits of schizotypal and schizoid personalities account for up to 77% of the variance of the total premorbid adjustment in schizophrenic patients.
Conclusion: The degrees of premorbid adjustment in schizophrenia are related to the different premorbid personality disorders of schizophrenic patients, which are mainly those most genetically related with schizophrenia, that is, the spectrum of the schizophrenia.
Introduction
Considered from the point of view of the vulnerability hypothesis, the premorbid period of schizophrenia could be defined as the time in which the basic traits of vulnerability are manifested without the participation of the morbid process. This time period has been limited to that which finishes 6 months before the patient's first psychiatric hospitalization, first psychiatric contact or first evidence of characteristic florid psychotic symptoms (Cannon-Spoor et al. 1982). Premorbid adjustment can be defined (Phillips 1953) as the degree to which a subject had fulfilled the appropriate expectations for his or her sex and age before the onset of the illness. Thus, subjects with poor premorbid adjustment would be those who failed to fulfill one or more of the goals of maturation before the onset of the disorder or who, if they did reach them, would do so in a period of life later than that considered to be the most appropriate.
There is extensive literature on premorbid adjustment relating to many important aspects of schizophrenia. In a combined study, Strauss et al. (1977-a,b), Klorman et al. (1977-a,b), and Kokes et al. (1977) extensively reviewed this. Using the Elguin Prognostic Scale, the first premorbid adjustment scale, Wittman (1941) aimed to offer an objective way to differentiate the process forms of schizophrenia from the reactive ones. It was subsequently observed that the usefulness of measuring premorbid adjustment was greater than first thought. Thus, it has been demonstrated that schizophrenics with poor premorbid adjustment have a worse prognosis and evolution (Strauss & Carpenter 1972, 1974, 1977, Evans et al. 1973, Bromet et al. 1974, Strauss et al. 1977-a, Zigler et al. 1979, Cannon-Spoor et al. 1982, García-Ribera 1983, McGlashan 1984, Harrow et al. 1986, Álvarez et al. 1987, Bailer et al. 1996), non-paranoid forms of the illness (Goldstein et al. 1968, Zigler & Levine 1973, Zigler et al. 1977, Goldstein 1978), more cognitive impairments (Addington & Addington 1993), more organic alterations (Quitkin et al. 1976, Weinberger et al. 1980, Williams et al. 1985, Keefe et al. 1989, Klausner et al. 1992, Levitt et al. 1994), and more negative symptoms (Keefe et al. 1989, Fenton & McGlashan 1991, McGlashan & Fenton 1992, Kelley et al. 1992, Addington & Addington 1993, Levitt et al. 1994, Peralta et al. 1995, Bailer et al. 1996, Larsen et al. 1996).
Strauss et al. (1977-a) consider that premorbid adjustment alterations can be a manifestation of vulnerability to schizophrenia or an early clinical manifestation, that is, an early phase or prodrome of schizophrenia. The link between premorbid adjustment and vulnerability to schizophrenia is also supported by other papers (Hartmann et al. 1984, Nuechterlein & Dawson 1984, Nuechterlein et al. 1992). This possibility concurs with the neurodevelopment hypothesis of schizophrenia which proposes the existence of a non-progressive and early cerebral lesion whose origin could be both genetic and environmental. The behavioral and cognitive effects of such a lesion would gradually change as the nervous system develops and matures. In the immature brain, the functional effects would be subtle with relatively minor deficits, such as a reduction of both the affective response and sociability (poor premorbid adjustment). The psychotic symptoms become manifest only when the brain reaches functional maturity in adolescence (Murray & Lewis 1987, Weinberger 1987, Lewis 1989). Thus, the premorbid adjustment alterations would be the early, cognitive and behavioral manifestations of the lesion before the development of frank schizophrenia (Foerster et al. 1991).
We would also add that the alterations in premorbid adjustment could be the manifestation of another disorder prior to the schizophrenia which may or may not be related to it, for example, a personality disorder. This hypothesis does not exclude the previous one. Family, adoptive and genetic studies have shown that the disorders of the spectrum (mainly schizoid and schizotypal) are genetically related to schizophrenia (Kety et al. 1968, Rosenthal et al. 1971, Kendler et al. 1981, Kendler & Gruenberg 1982, 1984, Baron et al. 1983, Gunderson & Siever 1985, Torgensen 1985, Nestadt et al. 1994, Kendler & Walsh 1995). In addition, other authors (Arieti 1974, M. Bleuler 1978, Hogg et al. 1990, Solano & Chávez 2000) have found premorbid personality disorders that differ from those of the spectrum and whose relationship with the schizophrenia is not a genetic one but rather one of a different type.
Several studies have suggested a connection between poor premorbid adjustment and schizoid and schizotypal personalities (Kretschmer 1925, Wittman 1941, Quitkin et al. 1976, Kokes et al. 1977, Zubin et al. 1983, Nuechterlein & Dawson 1984, McGlashan 1986, Fenton & McGlashan 1989, Dalkin et al. 1994). However, very few authors have studied the connection between premorbid adjustment and previous personality experimentally (Jorgensen & Parnas 1990, Foerster et al. 1991). In our study, we have attempted to determine whether there is any correlation between premorbid adjustment and previous personality disorders of subjects with schizophrenia and, if this correlation does exist, to see which personality disorders it is related to and to study the degree to which premorbid adjustment depends on those pathological personality traits.
Method
Subjects
Forty schizophrenic outpatients were consecutively selected from different area I Health Service Centers in Madrid (Spain). All of them fulfilled the DSM-III-R, DSM-IV and ICD-10 schizophrenia criteria. The inclusion requirements were the following: 1) to facilitate the diagnosis of the personality disorder, the patient had to be at least 18 years old, 2) for the respective diagnosis of adjustment and personality to be reliable, the maximum evolution period of the disease was limited to 10 years, 3) the acute phase of the patients had to be in remittance and there had to be no important overall impairment which could interfere with the interviews, 4) and finally, there had to be family collaboration. Only two patients refused to participate in the study. Five patients were not included due to significant overall impairment. Information was obtained from family members in all of the 40 patients chosen. All of the patients gave their informed consent to participate in the study.
The mean age of the 40 patients was 29+6 years and 22 of them (55%) were male and 28 (70%) single. The mean evolution time of their schizophrenia was 5+4 years. All the patients were receiving out-patient treatment at the time of the evaluation, but they had an average of 1.4+1.6 hospitalizations. Their schizophrenia was paranoid in 75% of the cases. Although this ratio of paranoia is high, it is quite representative of the total group of schizophrenics in our environment.
Material
Schizophrenia was diagnosed according to DSM-III-R criteria using the Structured Clinical Interview for DSM-III-R (SCID) by Spitzer et al. (1990a). In a later review, we verified that they also fulfilled the DSM-IV and ICD-10 schizophrenia diagnostic criteria.
The Premorbid Adjustment Scale (PAS) of Cannon-Spoor et al. (1982) was used to measure premorbid adjustment. This measurement scale was developed to be used in research. It was designed to evaluate the degree of development reached in the different periods of the subject's life before the onset of schizophrenia. Therefore, the PAS evaluation is not focused on the onset of the illness, but rather on the development of the maturation process in different periods of life. The different areas of life (social, sociosexual, school, work and autonomy) were also analyzed separately.
To study the personality disorders, we used the structured clinical interview for DSM-III-R, personality disorders (SCID-II version 1.0) by Spitzer et al. (1990b). This is a structured interview used to diagnose the full range of personality disorders of DSM-III-R. Based on the prototypical characteristics and the polythetic nature of the personality disorder criteria of DSM-III-R, we used a dimensional measure. This refers to the number or proportion of criteria that a subject fulfills from all the criteria of each personality disorder. It will range from 0% (subjects who do not fulfill any criteria) to 100% (patients who fulfill all the criteria defining a personality disorder). This system provides a quantitative measurement scale that can detect empirical relationships better than the qualitative results (all-or-none) inherent to the categorical systems.
Procedure
Once the cases were chosen, we applied the measurement instruments in the following order: 1. Clinical-diagnostic evaluation (SCID); 2. Premorbid adjustment (PAS); 3. Personality disorders (SCID-II). In every case, separate interviews were carried out with the patients and family members. The interviews with family members helped to increase the reliability of the retrospective data provided by the patients. When the answers of both the patient and the informing family member did not coincide, the evaluator weighed the validity of each source using his own clinical criterion and also counted on the collaboration of the patient's usual psychiatrist. To make sure that the data on premorbid adjustment and personality were not a consequence of the symptoms of the schizophrenic disorder, we emphasized that they always had to concentrate on their usual behavior before the onset of the psychotic symptoms.
It was verified that the variables followed a normal distribution, which made it possible to perform the following parametric statistical studies: Student's "t" test for comparison of means, Pearson's correlation between the variables, and stepwise multiple linear regression to estimate the premorbid adjustment variance produced by the different personality disorders.
Results
Premorbid adjustment
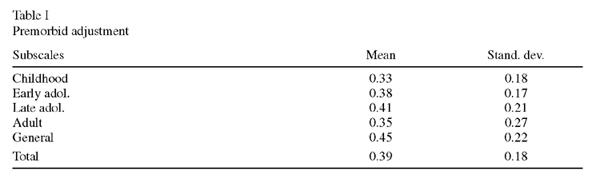
The mean premorbid adjustment for each one of the subscales is shown in Table I. On a continuous scale, the scores ranged from 0, corresponding to the best adjustment, to 1, which refers to the worst premorbid adjustment of the subjects. The best premorbid result is that occurring in childhood, with a progressive worsening during adolescence.
Previous personality
Of the 40 patients included in the study, 34 of them (85%) had at least one personality disorder. The most frequent premorbid personality disorders were: avoidant personality disorder (32.5%), schizoid personality disorder (27.5%), paranoid personality disorder (20%), dependent personality disorder (20%) and schizotypal personality disorder (12.5%). Greater details on premorbid personality disorders in schizophrenia are given by us in another paper (Solano & Chávez 2000). The mean rates shown in Table II were found when we analyzed the dimensional data of the personality disorders. These data are the mean percentage of the total number of criteria for each personality disorder fulfilled by the group of patients.

Premorbid adjustment and previous personality
The total premorbid adjustment (0.23 + 0.09) was significantly worse (p<0.05 Student's "t" test) in those patients who had had any previous personality disorder than it was in schizophrenics with no premorbid personality disorders (0.41 + 0.18).
Table III shows the correlations between premorbid adjustment and previous personality. Premorbid psychosocial adjustments in all the subscales, childhood, early adolescence, late adolescence, adulthood and general, are significantly correlated to the avoidant, schizotypal and schizoid pathologies. That is, the greater the number of personality disorders criteria that the patient has, the worse the premorbid psychosocial functioning.
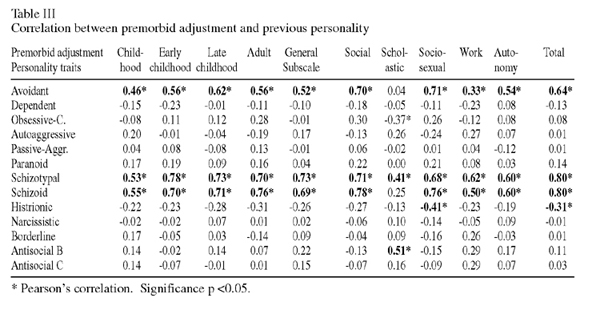
According to categories, we see how the social premorbid adjustment and the number of traits of the avoidant, schizotypal and schizoid P.D. are well correlated. That is, the worst social premorbid adjustment is found in those patients with more avoidant, schizotypal and schizoid pathology. Scholastic premorbid adjustment is also related to obsessive-compulsive pathology of the personality, which means that as the number of pathological traits of this kind increases, there is a trend towards better adjustment in this area. An association also exists with behavioral disorder in childhood, as the higher the number of antisocial B criterion traits, the worse is adjustment to school. Premorbid sociosexual functioning is significantly correlated with avoidant, schizotypal and schizoid traits, that is, social sexual function was worse in those subjects having the most pathology of these kinds. There is a correlation with the histrionic pathology, that is, the greater the existence of histrionic pathology of the personality, the better the sociosexual premorbid adjustment. The premorbid adjustment to work and autonomy also have significant correlations with the avoidant, schizotypal and schizoid P.D.
Regarding the total premorbid adjustment, we observed that those patients who have the most avoidant, schizotypal and schizoid personality traits are the ones who have the worst total premorbid adjustment. However, the greater the number of histrionic traits, the better the overall premorbid adjustment.
In our study, we could not find any association between premorbid adjustment and the traits of the dependent, self-defeating, passive-aggressive, paranoid, narcissistic, borderline and antisocial C personalities in the sample as a whole.
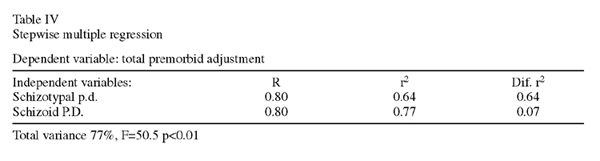
We also performed a stepwise multiple regression analysis. We considered premorbid adjustment as a dependent variable and each of the pathologies of the personality with a significant correlation as an independent variable. The analysis was performed to determine the capacity of the different P.D. to predict premorbid adjustment. With this procedure we added each one of the personality disorders one at a time to be used as predictor variables in order to discover their contribution to premorbid adjustment. We only included those variables which made a significant difference in the rate of determination (r2) that is, those that meant a significantly higher predictor capacity than that given by the previous variables. Thus, the pathological traits of schizotypal and schizoid personalities account for up to 77% of the variance of the total premorbid adjustment in schizophrenic patients (Table IV). All of the avoidant and histrionic personalities, which also correlate with total premorbid adjustment, do not add any more predictive value than that provided by the schizotypal and schizoid personalities.
Discussion
The main methodological weakness found in this study is that the data was retrospective, so that patients and their family members could have been biased in their assessment of premorbid personality and adjustment due to the development of the illness. Moreover, the sample was somewhat biased towards patients whose illnesses had a longer duration since these patients were more likely to be in contact with the service than those who may well have recovered after a single episode of illness. However, this study also has certain advantages, as we used standardized definitions of personality disorders and structured instruments to assess premorbid adjustment and personality disorders. In addition, we used the information provided by family members to corroborate the data obtained in all cases.
Our results regarding premorbid adjustment are similar to those found by other authors using the same scale (Cannon-Spoor et al. 1982, Haas & Sweeney 1992, Schanda et al. 1992, McCreadie et al. 1994, Larsen et al. 1996).
The results correlating adjustment and premorbid personality that we found are verified by several authors. Zubin et al. (1983), in a review of several papers, found that premorbid adjustment in schizophrenic patients with schizoid premorbid personality was worse than in those who did not have this type of personality. McGlashan (1986) demonstrated a significantly worse premorbid adjustment in schizophrenics with associated premorbid schizotypal personality disorder than those not having this personality disorder. Seguí et al. (1986) related poor premorbid adjustment to previous schizoid and schizotypal personality disorders. These authors state that the social network is a support system that favors better premorbid adjustment, protects against disease and softens the effect of stress factors. If the most important trait in the subject's personality disorder is social isolation, this would favor poor premorbid adjustment and thus, greater vulnerability. Malmberg et al. (1998) found that those patients who had the most difficulty in maintaining close personal relationships were the most vulnerable to develop schizophrenia. Using a methodology which was very similar to that used in our study, Foerster et al. (1991) demonstrated a clear correlation between poor premorbid adjustment and previous schizoid and schizotypal P.D. in schizophrenic patients. Castle et al. (1993) found that schizophrenia in young males diagnosed with very stringently defined criteria is associated with premorbid maladjustment and the existence of personality disorders. They suggest that these premorbid disorders indicate a severe form of schizophrenia that they call the neurodevelopmental form. McCreadie et al. (1994), find more schizoid and schizotypical traits and greater premorbid deterioration in schizophrenic patients than in their siblings. As we do, they find a statistically significant association between social premorbid adjustment and schizoid and schizotypal personality disorders. They emphasize the concept of "Neurodevelopmental schizophrenia" as a different form of the disease. These would be patients who show evidence of an alteration in development manifested as a personality disorder and in their childhood and adolescent social functioning. This malfunctioning in childhood and adolescence can be an early manifestation of the disease itself, or of a previous lesion that promotes the development of the disease and its symptoms. All the premorbid alterations of schizophrenic patients could be, as suggested by Jablensky (1998) and Jones (1998), the result of a single underlying factor, for example, a neurocognitive alteration or early cerebral insult that worsens with neurodevelopment. With this hypothesis, it is assumed that the causes of the disorder act early in life, a long time before the onset of the disease. Young people who suffer schizophrenia, far from maturing socially with greater involvement and trust in others, already begin to suffer deterioration in their childhood and adolescence, which is manifested by premorbid adjustment alterations. After late adolescence, the form of presentation would be like a frank schizoid or schizotypal personality disorder which would end up developing into schizophrenia. In fact, as Goldberg & Schmidt (2001) show, the degree of shyness and a low level of sociability in childhood and adolescence are precursors of a permanent social dysfunction in the adult schizophrenic. Willinger et al. (2001) verify that the premorbid variables, among which the alterations of premorbid adjustment and schizotypal and schizoid personalities are included, are manifestations of a neurodevelopmental disorder that will eventually be manifested as a schizophrenic disorder.
Jorgensen & Parnas (1990) found data that correlated premorbid adjustment and previous personality disorders that greatly differed from our findings. In their study, they found that poor premorbid adjustment was associated with the presence of previous histrionic and antisocial personality traits. The obsessive-compulsive P.D. was related to good premorbid adjustment and avoidant and schizoid P.D. had no relationship at all to premorbid adjustment. These differences are probably due to the different methodologies used, basically those used to measure the personality disorders.
It can be questioned whether the association between psychosocial adjustment and personality disorder is specific to schizophrenic patients. Since personality disorders are often manifested as interpersonal problems, it is not surprising to discover that the subjects who suffer them have more premorbid adjustment alterations than those that have no personality disorders, independently of whether they suffer a disorder of the associated axis I. It has been shown that suffering a personality disorder leads to poor psychosocial functioning (Zigler et al. 1979, Drake & Vaillant 1985, Casey & Tyrer 1986, Bernstein et al. 1993, Thaker et al. 2001). This has been demonstrated in patients with affective disorders: the subjects having the worst premorbid adjustment are those who have a previous borderline P. D. (Fiester et al. 1990). In obsessive-compulsive disorders, the existence of a personality disorder is also related to poorer psychosocial adjustment (Steketee 1990). Based on our results, we conclude that although poor premorbid adjustment has generally been linked to the existence of any type of personality disorder, in schizophrenia it is really related to one of the personality disorder groups that occur prior to the onset of the illness. It is precisely those personality disorders that are more closely related genetically to schizophrenia that cause the worse premorbid adjustment. In accordance with Cuesta et al. (1999), schizoid and schizotypal premorbid personalities can increase vulnerability to schizophrenia. It is likely that vulnerability increases as the genetic load becomes greater. However, Carpenter (personal communication) considers that these personalities are not vulnerability factors, but rather that they are manifestations of the disease.
Together with the spectrum disorders (schizoid and schizotypal), we have found that avoidant personality disorder is also correlated with premorbid adjustment alterations. This could be explained by the fact that the three disorders (schizotypal, schizoid and avoidant) are considered to be elements of the same pathological continuum (Livesly et al. 1983). On the other hand, it stands out that we have not found that paranoid personality traits, which are also representative of the schizophrenic spectrum, are correlated to premorbid adjustment.
It is also important that not all the pathological traits of all the personalities point in the same direction of premorbid adjustment. For example, the traits of the histrionic and obsessive-compulsive P.D. mean, although weakly, better adjustment in some areas. As Zubin et al. (1983) suggested, certain personality disorders may be considered as variables that act to prevent the disease.
Acknowledgements
We thank Alanen Y.O., Böker W., Carpenter W.T., David A.S. and Räkköläinen V. for their help and suggestions on this manuscript.
References
Addington J, Addington D. Premorbid Functioning, Cognitive Functioning, Symptoms and Outcome in Schizophrenia. J Psychiatr Neurosci 1993; 18(1): 18-23. [ Links ]
Alvarez E, García Ribera C, Torrens M, Udina C, Guillamat R, Casas M. Premorbid Adjustment Scale As a Prognostic Predictor For Schizophrenia. Br J Psychiatr 1987; 150: 411. [ Links ]
Arieti S. Interpretation of Schizophrenia. 2nd ed. New York: Basic Books Edit; 1974. [ Links ]
Bailer J, Bräuer W, Rey ER. Premorbid Adjustment as Predictor of Outcome in Schizophrenia: Results of a Prospective Study. Acta Psychiatr Scand 1996; 93: 368-377. [ Links ]
Baron M, Gruen R, Asnis L, Kane J. Familial Relatedness Of Schizophrenia and Schizotypal States. Am J Psychiatr 1983; 140: 1437-1442. [ Links ]
Bernstein DP, Cohen P, Velez N, Schwab-Stone M, Siever LJ, Shinsato L. Prevalence and Stability of the DSM-III-R Personality Disorders in a Community-Based Survey of Adolescents. Am J Psychiatr 1993; 150: 1237-1243. [ Links ]
Bleuler M. The Schizophrenics Disorders. Long-term Patient and Family Studies. London: Yale University Press; 1978. [ Links ]
Bromet E, Harrow M, Karl S. Premorbid Functioning and Outcome in Schizophrenics and Nonschizophrenics. Arch Gen Psychiatr 1974; 30: 203-207. [ Links ]
Cannon-Spoor E, Potkin SG, Wyatt RJ. Measurement of Premorbid Adjustment in Chronic Schizophrenia. Schizophr Bull 1982; 8: 470-484. [ Links ]
Casey PR, Tyrer P. Personality. Functioning and Symptomatology. J Psychiatr Res 1986; 20: 363-374. [ Links ]
Castle DJ, Wessely S, Murray RM. Sex and Schizophrenia: Effects of Diagnostic Stringency, and Associations with and Premorbid Variables. Br J Psychiatr 1993; 162: 658-664. [ Links ]
Cuesta MJ, Peralta V, Caro F. Premorbid Personality in Psychoses. Schizophr Bull 1999; 25(4): 801-811. [ Links ]
Dalkin T, Murphy P, Glazebrook C, Medley I, Harrison G. Premorbid Personality in First-Onset Psychosis. Br J Psychiatr 1994; 164: 202-207. [ Links ]
Drake RE, Vaillant GE. A Validity Study of Axis II of DSM III. Am J Psychiatr 1985; 142: 553-558. [ Links ]
Evans JR, Goldstein MJ, Rodnick EH. Premorbid Adjustment, Paranoid Diagnosis, and Remission: Acute Schizophrenics Treated in a Community Mental Health Center. Arch Gen Psychiatr 1973; 28: 666-672. [ Links ]
Fenton WS, McGlashan TM. Risk of Schizophrenia in Character Disordered Patients. Am J Psychiatr 1989; 146(10): 1280-1284. [ Links ]
Fenton WS, McGlashan TM. Natural History of Schizophrenia Subtypes. II Positive and Negative Symptoms and Long-Term Course. Arch Gen Psychiatr 1991; 48: 978-986. [ Links ]
Fiester SJ, Ellison JM, Docherty JP, Shea T. Comorbidity of Personality Disorders: Two for the Price of Three. In: Adler DA, ed. Treating Personality Disorders. San Francisco: Jossey-Bass; 1990. p. 103-114. [ Links ]
Foerster A, Lewis S, Owen M, Murray R. Premorbid Adjustment and Personality in Psychosis. Effects of Sex and Diagnosis. Br J Psychiatr 1991; 158: 171-176. [ Links ]
García Ribera C. Factores Premórbidos como Indicador Pronóstico en la Esquizofrenia. Avances en Terapéutica Psiquiátrica. Barcelona: Sociedad Catalana de Psiquiatría; 1983. [ Links ]
Goldberg JO, Schmidt LA. Shyness, Sociability and Social Dysfunction in Schizophrenia. Schizophr Res 2001; 48: 343-349. [ Links ]
Goldstein MJ. Further Data Concerning the Relation Between Premorbid Adjustment and Paranoid Symptomatology. Schizophr Bull 1978; 4(2): 236-243. [ Links ]
Goldstein MJ, Held JM, Cromwell RL. Premorbid Adjustment and Paranoid-Nonparanoid in Schizophrenia. Psycholog Bull 1968; 70: 382-386. [ Links ]
Gunderson JG, Siever LJ. Relatedness of Schizotypal to Schizophrenic Disorders: Editor Introduction. Schizophr Bull 1985; 11(4): 532-537. [ Links ]
Haas GL, Sweeney JA. Premorbid and Onset Features of First-Episode Schizophrenia. Schizophr Bull 1992;18(3): 373-386. [ Links ]
Harrow M, Westermeyer JF, Silverstein M, Strauss BS, Cohler BJ. Predictors of Outcome in Schizophrenia: the Process-Reactive Dimension. Schizophr Bull 1986; 12(2): 195-206. [ Links ]
Hartmann E, Milofsky E, Vaillant G, Olfield M, Falice R, Ducey Ch. Vulnerability to Schizophrenia. Prediction of Adult Schizophrenia Using Childhood Information. Arch Gen Psychiatr 1984; 1: 1050-1056. [ Links ]
Hogg B, Jackson HJ, Rudd RP, Edwards J. Diagnosing Personality Disorders in Recent-Onset Schizophrenia. J Nerv Ment Dis 1990; 178(3): 194-199. [ Links ]
Jablensky A. High Risk. Low Prediction: Implications for Early Intervention. Br J Psychiatry 1998; 172: 314. [ Links ]
Jones P. Who Gets Schizophrenia. Br J Psychiatr 1998; 172: 314-315. [ Links ]
Jorgensen A, Parnas J. The Copenhagen High-Risk Study: Premorbid and Clinical Dimensions of Maternal Schizophrenia. J Nerv Ment Dis 1990; 178: 370-376. [ Links ]
Keefe RSE, Mohs RS, Losconczy MF, Davidson M, Silverman JM, Horvath TB et al. Premorbid Sociosexual Functioning and Long-term Outcome in Schizophrenia. Am J Psychiatr 1989; 146: 206-211. [ Links ]
Kelley ME, Gilberston M, Mouton A, Jan Kamhen DP. Deterioration in Premorbid Functioning in Schizophrenia: A Developmental Model of Negative Symptoms in Drug-Free Patients. Am J Psychiatr 1992; 149: 1543-1548. [ Links ]
Kendler KS, Gruenberg AM. Genetic Relationship between Paranoid Personality Disorder and the 'Schizophrenia Spectrum' Disorders. Am J Psychiatr 1982; 139(9): 1185-1186. [ Links ]
Kendler KS, Gruenberg AM. An Independent Analysis of the Danish Adoption Study of Schizophrenia, VI. The Relationship between Psychiatric Disorders as Defined by DSM-III in the Relatives and Adoptees. Arch Gen Psychiatr 1984; 41: 555-564. [ Links ]
Kendler KS, Walsh D. Schizotypal Personality Disorder in Parents and the Risk for Schizophrenia in Siblings. Schizophr Bull 1995; 21(1): 47-52. [ Links ]
Kendler KS, Gruenberg AM, Strauss JS. An Independent Analysis of the Copenhagen Sample of the Danish Adoption Study of Schizophrenia, II. The Relationship between Schizotypal Personality Disorder and Schizophrenia. Arch Gen Psychiatr 1981; 38: 982-984. [ Links ]
Kety SS, Rosenthal D, Wender PH, Schulsinger F. The Types and Prevalence of Mental Illness in the Biological and Adoptive Families of Adopted Schizophrenics. J Psychiatr Res 1968; 6 Sup. 1: s345-s362. [ Links ]
Klausner JD. Sweeney JA, Deck MDF, Kelly AB. Clinical Correlates of Cerebral Ventricular Enlargement in Schizophrenia. Further Evidence for Frontal Lobe Disease. J Nerv Ment Dis 1992; 180(7): 407-412. [ Links ]
Klorman R, Strauss JS, Kokes RF. Premorbid Adjustment in Schizophrenia. Part III. The Relationship of Demographic and Diagnostic Factors to Measures of Premorbid Adjustment in Schizophrenia. Schizophr Bull 1977a; 3(2): 214-225. [ Links ]
Klorman R, Strauss JS, Kokes RF. Premorbid Adjustment in Schizophrenia. Part IV. Some Biological Approaches to Research on Premorbid Functioning in Schizophrenia. Schizophr Bull 1977b; 3(2): 226-239. [ Links ]
Kokes RF, Strauss JS, Klorman R. Premorbid Adjustment in Schizophrenia. Part II. Measuring Premorbid Adjustment: the Instruments and Their Development. Schizoph Bull 1977; 3(2): 186-213. [ Links ]
Kretschmer E. Physique and Character. London: Kegan Paul, Trench and Trubner; 1925. [ Links ]
Larsen TK, McGlashan TH, Johannessen JO, Vibe-Hansen L. First-Episode Schizophrenia: II Premorbid Patterns by Gender. Schizophr Bull 1996; 22(2): 257-269. [ Links ]
Levitt JJ, Shenton ME, Mccarley RW, Faux SF, Ludwig AS. Premorbid Adjustment in Schizophrenia: Implications for Psychosocial and Ventricular Pathology. Schizophr Res 1994; 12(2): 159-168. [ Links ]
Lewis SW. Congenital Risk Factors for Schizophrenia [Editorial]. Psychol Med 1989; 19: 5-13. [ Links ]
Livesley WJ, West M, Tanney A. Historical Comment on DSM-III Schizoid and Avoidant Personality Disorder. Am J Psychiatr 1985; 142: 1344-1347. [ Links ]
Malmberg A, Lewis G, David A, Allebeck P. Premorbid Adjustment and Personality in People with Schizophrenia. Br J Psychiatr 1998; 172: 308-313. [ Links ]
McCreadie RG, Connolly MA, Williamson DJ, Athawes RW, Tilak D. The Nithsdale Schizophrenia Surveys. XII. ´Neurodevelopmental´ Schizophrenia: a Search for Clinical Correlates and Putative Aetiological Factors. Br J Psychiatr 1994; 165(3): 340-346. [ Links ]
McGlashan TH. The Chestnut Lodge Follow-up Study. II: Long-Term Outcome of Schizophrenia and the Affective Disorders. Arch Gen Psychiatr 1984; 41: 586-601. [ Links ]
McGlashan TH. The Prediction of Outcome in Chronic Schizophrenia. IV: The Chestnut Lodge Follow-up Study. Arch Gen Psychiatr 1986; 46: 167-176. [ Links ]
McGlashan TH, Fenton WS. The Positive-Negative Distinction in Schizophrenia Review of Natural History Validators. Arch Gen Psychiatr 1992; 49: 63-72. [ Links ]
Murray RM, Lewis SW. Is Schizophrenia a Neurodevelopmental Disorder? Br Med J 1987; 295: 681-682. [ Links ]
Nestad G, Hanfelt J, Liang KY, Lamacz M, Wolyniec P, Pulver AE. An Evaluation of the Structure of Schizophrenia Spectrum Personality Disorders. J Pers Disord 1994; 8(4): 288-298. [ Links ]
Nuechterlein KH, Dawson M. A Heuristic Vulnerability Stress Model of Schizophrenic Episodes. Schizophr Bull 1984; 10: 300-312. [ Links ]
Nuechterlein KM, Dawson M, Gitlin M, Ventura J, Goldtein MJ, Snyder KS et al. Developmental Processes in Schizophrenic Disorders: Longitudinal Studies of Vulnerability and Stress. Schizophr Bull 1992; 18(3): 387-425. [ Links ]
Peralta V, Cuesta MJ, De Leon J. Positive and Negative symptoms/syndromes in Schizophrenia: Reliability and Validity of different diagnostic systems. Psychol Med 1995; 25: 43-50. [ Links ]
Phillips L. Case History Data and Prognosis in Schizophrenia. J Nerv Ment Dis 1953; 117: 515-525. [ Links ]
Quitkin F, Rifkin A, Klein DF. Neurological Soft Signs in Schizophrenia and Character Disorders: Organicity in Schizophrenia with Premorbid Asociality and Emotionally Unstable Character Disorders. Arch Gen Psychiatr 1976; 33: 845-853. [ Links ]
Rodríguez-Solano JJ, González de Chávez M. Premorbid Personality Disorders in Schizophrenia. Schizophr Res 2000; 44(2): 137-144. [ Links ]
Roshental D, Wender PH, Kety SS. The Adopted Way Offspring of Schizophrenics. Am J Psychiatr 1971; 128: 307-311. [ Links ]
Schanda H, Foldes P, Topitz A, Fliedl R, Knecht G. Premorbid Adjustment of Schizophrenic Criminal Offenders. Acta Psychiatr Scand 1992; 86: 121-126. [ Links ]
Segui J, Humbert MS, Salvador L, Malet D, Judar I. Ajuste Social del Enfermo Esquizofrénico. Revista del Departamento de Psiquiatría de la Facultad de Medicina de Barcelona 1986; 13(4): 175-187. [ Links ]
Spitzer RL, Williams JBW, Gibbon M, First MB. Structured Clinical Interview for DSM-III-R (SCID). Washington, DC: American Psychiatric Press; 1990-a. [ Links ]
Spitzer RL, Williams JBW, Gibbon M, First MB. Structured Clinical Interview for DSM-III-R Personality Disorders (SCID-II) Version 1.0. Washington, DC: American Psychiatric Press; 1990-b. [ Links ]
Steketee G. Personality Traits and Disorders in Obsessive-Compulsives. J Anxiety Dis 1990; 4: 351-364. [ Links ]
Strauss JS, Carpenter WT. The Prediction of Outcome in Schizophrenia, I: Characteristics of Outcome. Arch Gen Psychiatr 1972; 27: 739-746. [ Links ]
Strauss JS, Carpenter WT. The Prediction of Outcome in Schizophrenia: II Relationships Between Predictor and Outcome Variables: A Report from the WHO International Pilot Study of Schizophrenia. Arch Gen Psychiatr 1974; 31: 37-42. [ Links ]
Strauss JS, Carpenter WT. Prediction of Outcome in Schizophrenia: III Five Years Outcome and its Predictors. Arch Gen Psychiatr 1977; 34: 159-163. [ Links ]
Strauss JS, Klorman R, Kokes RF. Premorbid Adjustment in Schizophrenia. Part V. The Implications of Findings for Understanding, Research, and Application. Schizophr Bull 1977a; 3(2): 240-244. [ Links ]
Strauss JS, Kokes RF, Klorman R, Sacksteder JL. Premorbid Adjustment in Schizophrenia: Concepts Measures and Implications Part I. The Concept of Premorbid Adjustment. Schizophr Bull 1977b; 3(2): 182-185. [ Links ]
Thaker G, Adami H, Gold J. Functional Deterioration in Individuals with Schizophrenia Spectrum Personality Symptoms. J Pers Disord 2001; 15(3): 229-234. [ Links ]
Torgersen S. Relationship of Schizotypal Personality Disorder to Schizophrenia: Genetics. Schizophr Bull 1985; 11(4): 554-563. [ Links ]
Weinberger DR. Implications of Normal Brains Development for the Pathogenesis of Schizophrenia. Arch Gen Psychiatr 1987; 44: 660-669. [ Links ]
Weinberger DR, Cannon-Spoor HE, Potkin SG, Wyatt RJ. Poor Premorbid Adjustment and C.T. Span Anomalies in Chronic Schizophrenia. Am J Psychiatr 1980; 137: 1410-1415. [ Links ]
Willians AO, Reveley MA, Kolakonska T, Ardern M, Mandelbrote BM. Schizophrenia with Good and Poor Outcome II: Cerebral Ventricular Size and its Clinical Significance. Br J Psychiatr 1985; 146: 239-246. [ Links ]
Willinger U, Heiden AM, Meszaros K, Formann AK, Aschauer HN. Neurodevelopmental Schizophrenia: Obstetric Complications, Birth Weight, Premorbid Social Withdrawal and Learning Disabilities. Neuropsychobiology 2001; 43(3): 163-169. [ Links ]
Wittman MP. A Scale for Measuring Prognosis in Schizophrenic Patients. Elguin Paper 1941; 4: 20-33. [ Links ]
Zigler E, Levine J. Premorbid Adjustment and Paranoid Nonparanoid Status in Schizophrenia. A Further Investigation. J Abnormal Psychologie 1973; 82: 189-199. [ Links ]
Zigler E, Levine J, Zigler B. Premorbid Social Competence and Paranoid-nonparanoid Status in Female Schizophrenic Patients. J Nerv Ment Dis 1977; 164: 333-339. [ Links ]
Zigler E, Glick M, Marsh A. Premorbid Social Competency and Outcome Among Schizophrenic and Nonschizophrenic Patients. J Nerv Ment Dis 1979; 167: 478-483. [ Links ]
Zubin J, Magaziner J, Steinhauer SR. The Metamorphosis of Schizophrenia: From Chronicity to Vulnerability. Psycholog Med 1983; 13: 551-571. [ Links ]
Adress of correspondence:
Dr. D. José Juan Rodríguez Solano
Servicio de Salud Mental de Vallecas
Calle Peña Gorbea, 4
28018 Madrid
Telf.: 91 477 87 47
Fax.: 91 477 91 37
E-mail: rodriguez.solano@wanadoo.es
SPAIN

