










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO  Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.96 no.3 Madrid mar. 2004
| ORIGINAL PAPERS |
Complications of endoscopic retrograde cholangiopancreatography.
A study in a small ERCP unit
J. García-Cano Lizcano, J. A. González Martín, J. Morillas Ariño and A. Pérez Sola
Service of Digestive Diseases. Hospital Virgen de la Luz. Cuenca, Spain
ABSTRACT
Backgrounds and aim: endoscopic retrograde cholangiopancreatography (ERCP) is an established procedure to drain the biliary and pancreatic ducts. Nevertheless, there are complications which seem to be more common in centers performing less than 200 ERCPs per year. Sometimes, however, due to the distribution of health resources, it is necessary to perform this technique in centers with a smaller number of procedures. We present the experience of ERCP-related complications in a small unit.
Material and methods: this is a retrospective study on prospective data recorded during six years (1997-2002). In this period, two endoscopists working together performed 507 ERCPs, which yields an approximately average of 84 procedures per year.
Results: in 507 ERCPs performed during this period of time, 55 complications arose (10.85%), and four patients died (0.79%) as a consequence of the procedure. There were 28 pancreatitis (5.5%), eight post-sphincterotomy bleeding events (1.6%), seven bilioduodenal perforations (1.4%), eight sepsis episodes of biliary origin (1.6%), and other 4 different complications. There were 418 (82.4%) successful ERCPs -either diagnostic or therapeutic-, which gave rise to 46 (11%) complications. There were 89 (17.6%) failed diagnostic or therapeutic ERCPs, which gave rise to 9 (10.11%) complications (p = 0.8 between both groups). Thirty five (7%) ERCPs were exclusively diagnostic and caused 6 (17%) complications. The 187 procedures performed for coledocho-lithiasis originated 14 (7.4%) complications, and represented the group with the lowest morbidity rate (p = 0.04).
Conclusions: the complications rate in our center is within the range of reported figures. ERCPs performed for choledoco-lithiasis was associated with the lowest complications rate. The risk-benefit ratio in the anticipated, purely diagnostic ERCP must be carefully weighed due to its morbidity.
Key words: ERCP complications.
García-Cano Lizcano J, González Martín JA, Morillas Ariño J, Pérez Sola A. Complications of endoscopic retrograde cholangiopancreatography. A study in a small ERCP unit. Rev Esp Enferm Dig 2004; 96: 163-173.
Recibido: 20-01-03.
Aceptado: 03-09-03.
Correspondencia: J. García-Cano Lizcano. Residencial Los Alfares, bloque 4, 6º D. 16002 Cuenca. e-mail: jgarciacano@teleline.es
INTRODUCTION
Endoscopic retrograde cholangiopancreatography (ERCP) is a very effective procedure to drain both the biliary and pancreatic ducts (1). Nowadays, available methods to image the pancreatobiliary system, specially magnetic resonance cholangiopancratography (MRCP), have turned ERCP into an eminently therapeutic procedure.
Gaining access to the bile and pancreatic ducts, sphincterotomy, choledocholithiasis extraction, and biliary and pancreatic stent insertion are the more difficult procedures in digestive endoscopy (2).
The complexity of the procedure entails a morbidity that seems to be higher in centers performing few explorations. Though no unanimously accepted criteria exist, minimal standards have been fixed in 200 ERCPs per year (3), more than one sphincterotomy every week (4), or at least 40 sphincterotomies per year for each endoscopist (5).
Nevertheless, the distribution and access of patients to health resources can generate the need to perform this technique in hospitals in which a limited volume of procedures is annually expected. We present our experience regarding ERCP-related complications in a small unit.
MATERIAL AND METHODS
During a 6-year period (1997-2002) two endoscopists (JGL and JGM), working together, performed 507 ERCPs. This means an approximate average of 84 procedures per year. In alternate explorations, each of them acted as first or main endoscopist, while the other helped him as second endoscopist.
Patients were under conscious sedation with meperidine and diazepam or midazolam, administered by endoscopists themselves. Overall, the same team of nurses and endoscopy assistants was present at each exploration. Heart rate and oxygen blood saturation were monitored during ERCP. Oxygen was administered to patients by means of a nasal cannula. ERCPs were performed in a room with fluoroscopy facilities within the radiology department. All patients gave their informed consent for the procedure after receiving adequate medical information.
Therapeutic duodenoscopes with a working channel of 4.2 mm were used. Vater's papilla cannulation, sphincterotomy, dilatation, stent insertion, and other ERCP maneuvers were performed as previously described (6-8). When cannulation failed after using standard cannulae or sphincterotomes, a tapered-tip sphincterotome loaded with a 0.025 in guidewire proved very useful (9), and was used before performing a precut.
A diagnostic failure was considered when the desired duct could not be cannulated. Therapeutic failure was defined as the lack of effective endoscopic treatment (in general, an adequate duct drainage when necessary). Procedures for choledocolithiasis that could not be completed were not considered a therapeutic failure, if a stent was inserted to maintain a temporary drainage.
Odditis was diagnosed by means of the available clinical, analytical, and cholangiographic data.
All ERCPs were performed on an in-patient regime. Patients remained at hospital at least for the night after the procedure. In the following days, the occurrence of complications was ruled out. Complications were graded according to a 1991 consensus (10).
Data relative to procedures and complications were gathered in a prospective way, though the global analysis was performed in a retrospective way. Statistical analyses were carried out by using the Rsigma software program. A p value below 0.05 was considered significant.
RESULTS
Five hundred and seven ERCPs were performed. There were 55 (10.85%) complications in 52 patients (Table I). There were 28 (5.5%) acute pancreatitis cases, most of them graded as mild to moderate. Only four of them needed admission to an Intensive Care Unit (ICU). There was no mortality related to pancreatitis.
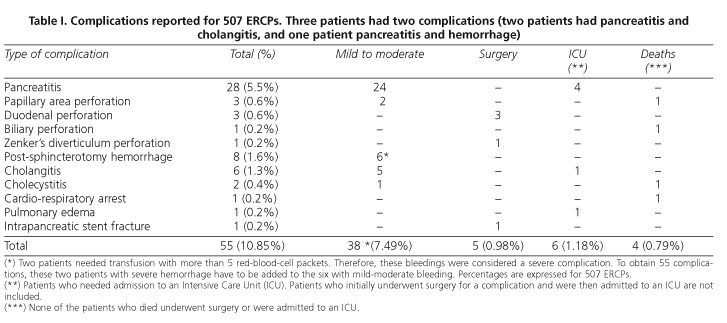
Eight (1.6%) post-sphincterotomy hemorrhages occurred. All of them needed endoscopic sclerotherapy on the bleeding source and blood transfusion. Two patients needed 5 or more unit of packed red blood cells, and these complications were accordingly graded as severe. Neither surgery nor therapeutic angiography were needed.
A duodenal perforation took place far from the papillary area in three patients (0.6%). The first one happened in the afferent loop of a Billroth II gastrectomy. The second perforation developed in a stenosed and deformed peptic duodenal bulb. The third one was secondary to a 15 cm-long biliary plastic stent previously inserted to treat a benign stricture, which perforated the duodenum. All patients underwent surgery and no mortality occurred as a consequence of the perforation.
In three women perforation took place within the papillary area (0.6%). A false route developed in a patient when trying to recannulate the bile duct after a sphincterotomy had been performed. A guidewire had not been left in place, and a retroperitoneal contrast injection occurred. In another patient, a perforation was induced by a large sphincterotomy in the setting of an intradiverticular papilla. These two patients recovered satisfactorily with medical treatment. The third of these perforations took place in an elderly patient with cholangitis. This perforation followed a precut and the patient died.
A patient with a complex hilar neoplasm presented with a biliary perforation probably related to dilatation, before stent insertion. The patient developed an abdominal abscess. His general condition adviced that no type of aggressive treatment be attempted, and the patient died a few days later. Therefore, bilioduodenal perforations were 7 (1.4%) in all.
A previously unknown Zenker's diverticulum was perforated in another patient. The diagnosis was immediately reached on observing mediastinal structures. It was also confirmed by water-soluble contrast extravasation from the esophagus. The patient underwent surgery and finally recovered after a complicated postoperative period.
Six (1.2%) patients developed cholangitis. In five of such cases, it was secondary to retained choledocholithiasis after ERCP, or to plastic biliary stents inserted in hilar tumors. They all evolved satisfactorily with medical treatment. The remaining cholangitis happened in a patient who was later diagnosed of leukemia, and needed admission to an ICU.
Two patients developed cholecystitis. One of them, a patient with a neoplasm of the head of the pancreas in whom a plastic biliary stent had been previously inserted, died. Therefore, there were 8 (1.6%) sepsis cases of biliary origin (cholangitis and cholecystitis).
An elderly patient in whom an ERCP was performed for cholangitis died after presenting a cardio-respiratory arrest on arriving at his ward after the procedure. This complication may be probably related to sedative medication during the endoscopic procedure. Another patient with ischemic heart disease developed a few hours after the endoscopic procedure congestive heart failure and pulmonary edema. He recovered after ten days in an ICU.
Finally, a 12 cm-long pancreatic stent broke within the pancreas. It had been inserted to treat a pleuro-pancreatic fistula in a patient with chronic pancreatitis. The distal part of the stent remained within Wirsung's duct after having tried to extract it once the fistula had cured. The patient needed a distal pancreatectomy following unsuccessful attempts at endoscopic extraction.
Only 17/55 complications were severe (31%), which in the whole series represents 17/507 (3.3%) severe complications. Thus, the majority were graded as mild to moderate and patients recovered with medical treatment. Four patients (0.79%) died.
All ERCP procedures were allocated to 8 groups (Table II): exclusively diagnostic procedures, therapeutic procedures, and failed procedures. It is remarkable that the 187/418 (44.7%) ERCPs performed to extract choledocholithiasis made up the group with the lowest complications rate (14/187 -7.4%-), and the only group with significantly less morbidity (p = 0.04) when compared to the rest of the series.
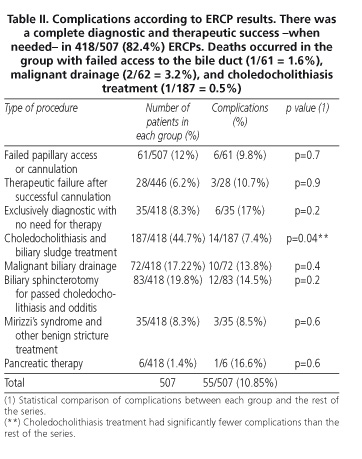
The ERCP group that needed no therapeutic measures (exclusively diagnostic) was the one that had more complications: 6/35 (17%). Nevertheless, this figure did not reach statistical significance when compared to the rest of the series.
No statistical difference was either found (p = 0.8) be-tween the 46 (11%) complications in the 418/507 (82.4%) ERCPs that were successfully diagnostic and therapeutic (when necessary), and the 9 (10.11%) complications in 89/507 (17.6%) ERCPs with diagnostic or therapeutic failure.
As a whole, a precut was used in 63/507 (12.4%) of ERCPs. There were no differences in use between the various ERCP groups. Logically, access to the bile duct was prevented in the failed ERCP group. There were 8/63 (12.7%) complications, which does not reach significance when compared to ERCPs in which precut was not used.
DISCUSSION
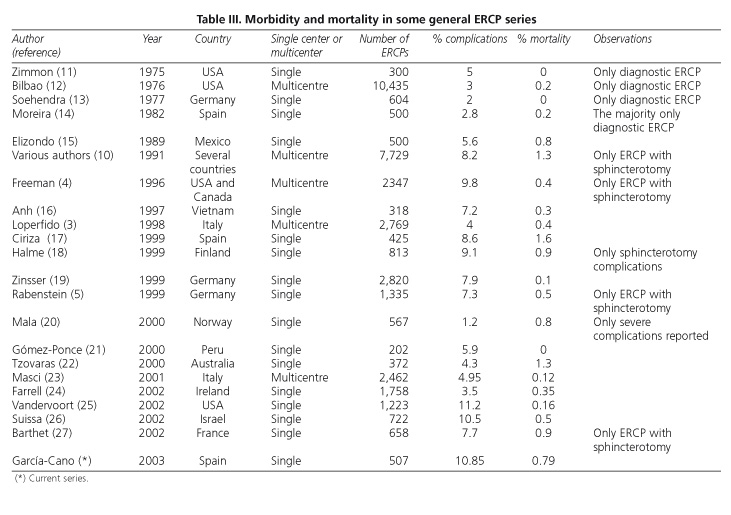
ERCP is the most difficult technique in digestive endoscopy. Complications occur approximately in 10% of cases, and mortality is about 1% (2). This is the range within which figures from a great number of published series lay (Table III). Overall, data from our study, with 10.85% of complications and a mortality of 0.79%, fit also in previously reported figures.
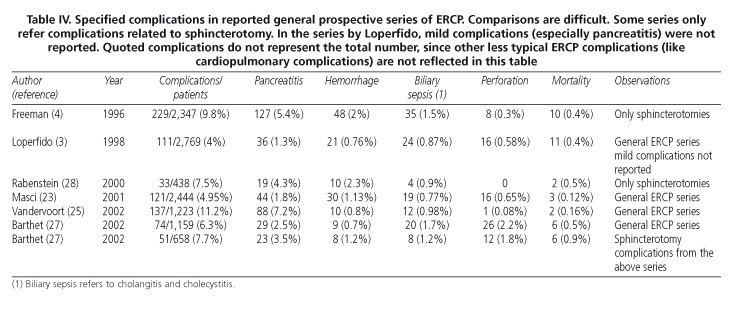
The four typical complications of ERCP are: acute pancreatitis, post-sphincterotomy bleeding, sepsis of biliary origin (cholangitis and cholecystitis), and perforation, either of the papillary area for sphincterotomy, or duodenal (far from the papillary area) for endoscopy or biliary stents. In our study, we found a pancreatitis rate of 5.5%, a hemorrhage rate of 1.6%, a rate of of bilioduodenal perforation of 1.4%, and a rate of biliary sepsis of 1.6%. These figures are also comparable to those in other studies (Table IV). There are, in addition, other rarer and less typical adverse effects of ERCP. In our case, there was a Zenker's diverticulum perforation, intrapancreatic fracture of a plastic stent, cardio-respiratory arrest -probably related to sedation- and pulmonary edema a few hours after ERCP. We considered this complication to be related to the endoscopic intervention since myocardial blood flow reduction has been described during ERCP (29).
Anyhow, the real percentage of complications is probably higher than that in published series. The great majority of studies define ERCP complications according to a 1991 consensus (10). According to these criteria, and with regard to post-sphincterotomy hemorrhage, for instance, this begins as a mild complication when hemoglobin drops more than 2 grams. Bleeding during the endoscopic procedure, with no hemogram decreases, is not considered a complication. Nevertheless, if hemostatic measures must be taken to stop a hemorrhage episode, ERCP complexity can increase enormously, even though this is not reflected as a complication.
With regard to acute pancreatitis, the usual definition is an at least three-fold increase of serum amylase for more than 24 hours, together with abdominal pain, which needs hospitalization. If ERCP is performed on an outpatient regime and the published series is retrospective, patients may complaint with mild abdominal pain at home, which really corresponds to a mild pancreatitis. This attack will remains undiagnosed and, therefore, unreported. Baillie reported (30) that the rate of ERCP complications at his center increased by 50% after a prospective study was performed by means of a telephonic survey within 30 days following the procedure. Acute pancreatitis was the most frequent complication discovered.
Besides, prospective multicentre series -like that of Masci (23)- find fewer complications when compared to single-centre serie -as that of Vandervoort (25) for instance. Probably, in multicentre series some mild complications may be missed out. Otherwise, these are most frequently reported in all series.
Another aspect that must be kept in mind when analyzing these studies is what we may call “the philosophy of self-imputed complications”. For example, in papers in which drugs are studied for the prevention of post-ERCP pancreatitis, the frequency of this complication in the control group is higher than in usual series (31).
ERCP is a very complex procedure which cannot be performed by all endoscopists (32). Not only is necessary a long learning period, but also skills already acquired should be maintained by performing the procedure in a steady and usual manner. Ideally, few endoscopists should perform more ERCPs (2). Nevertheless, as in our center, the distribution of health resources does probably require that this technique be performed in hospitals not reaching 200 ERCPs per year (33).
Constant and regular dedication by a few persons may obtain acceptable results for ERCP in a small center (34-36). In our unit, the two doctors who perform this technique are present in all procedures, in half of them acting as main endoscopists, and as assistant endoscopists in the other half. This concept, which has been clearly defined for surgical interventions, is not currently used in the endoscopic setting. We think that the complexity of endoscopic pancreatobiliary interventionism is such that, besides relying on a team made up of qualified nurses and endoscopy asisstants (which may often make a difference between success and failure) (37), the presence of at least two performing doctors is most advisable. Endoscopes and devices that are suitable and in good condition are another factor for success (38).
In our study, successful ERCPs had similar complications rates when compared to unsuccessful ERCPs. This is easily understandable. Fruitless, repeated attempts to cannulate the papilla induce pancreatitis, which is more serious when precut is used in an ineffective manner. Once cholangiography is performed, the inability to adequately drain an obstructed biliary tract results in cholangitis. Therefore, when an endoscopist faces an ERCP, he or she must have the highest possibility to obtain the expected results. To this end, ongoing technical improvement should be pursued in an attempt to overcome the minimal accepted success rate of 80% (39), using self-criticism (40).
Finally, the only group in our study with significantly lower morbidity was that with choledocholithiasis treatment. Similar data were reported by Freeman (4) on patients in whom laparoscopy cholecistectomy had been performed. Diagnostic ERCPs had, therefore, more complications than ERCPs in which choledochal stones were extracted. This paradox underlines the need to avoid complications in patients who less need ERCP (41). When an exclusively diagnostic procedure is foreseen (42), it is necessary to carefully weigh the risk-benefit ratio the technique may bring. Under such circumstances, MRCP is probably the most useful method to be chosen nowadays (43).
REFERENCES
1. Summerfield JA. Biliary obstruction is best managed by endoscopists. Gut 1988; 29: 741-5. [ Links ]
2. Huibregtese K. Complications of endoscopic sphincterotomy and their prevention (editorial). N Engl J Med 1996; 335: 961-3. [ Links ]
3. Loperfido S, Angelini G, Benedetti G, Chilouri F, Costan F, De Berardinis F, et al. Major early complications from diagnostic and therapeutic ERCP: a prospective multicenter study. Gastrointest Endosc 1998; 48: 501-10. [ Links ]
4. Freeman ML, Nelson DB, Sherman S, Haber GB, Herman ME, Dorsher PJ, et al. Complications of endoscopic biliary sphincterotomy. N Engl J Med 1996; 335: 909-18. [ Links ]
5. Rabenstein T, Schneider HT, Nicklas M, Ruppert T, Katalinic A, Hahn EG, et al. Impact of skill and experience of the endoscopist on the outcome of endoscopic sphincterotomy techniques. Gastrointest Endosc 1999; 50: 628-36. [ Links ]
6. Jacobson IM (editor). ERCP and its applications. Phialadelphia: Lippincott-Raven, 1998. [ Links ]
7. Martin DF, Tweedle D, Haboui NY. Clinical Practice of ERCP. Londres: Churchill Livingstone, 1998. [ Links ]
8. Topazian M (guest editor). Bile duct strictures. Techniques in Gastrointestinal Endoscopy 2002; vol. 4. [ Links ]
9. García-Cano Lizcano J, González Martín JA, Morillas Ariño MJ, Pérez Sola A. The Tapertome sphincterotome reduces the need of precut to cannulate the bile duct. (in Spanish). Rev Esp Enferm Dig 2001; 93 (Supl. I): P-1. [ Links ]
10. Cotton PB, Lehman G, Vennes J, Geenen JE, Russell RC, Meyers WC, et al. Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endosc 1991; 37: 383-93. [ Links ]
11. Zimmon DS, Falkenstein DB, Riccobono C, Aaron B. Complications of endoscopic retrograde cholangiopancreatography. Analysis of 300 consecutive cases. Gastroenterology 1975; 69: 303-9. [ Links ]
12. Bilbao MK, Dotter CT, Lee TG, Katon RM. Complications of endoscopic retrograde cholangiopancreatography (ERCP). A study of 10,000 cases. Gastroenterology 1976; 70: 314-20. [ Links ]
13. Soehendra N. Technique, difficulties and results of endoscopic retrograde cholangio-pancreatography (ERCP). Chirurg 1977; 48: 98-104. [ Links ]
14. Moreira Vicente VF, Meroño García E. Nuestra experiencia con la colangiopancreatografía retrógrada endoscópica (CPRE): 1977-1980. Rev Esp Enferm Dig 1982; 61: 202-17. [ Links ]
15. Elizondo J, Gallo S, Valdovinos MA, Paez R. Evaluación retrospectiva de 500 colangiopancreatografías endocópicas realizadas en el Instituto Nacional de la Nutrición "Salvador Zubirán". Rev Gastroenterol Mex 1989; 54: 19-26. [ Links ]
16. Anh LQ. Therapeutic endoscopy of the hepatobiliary and pancreatic system: a Vietnamese experience. JSLS 1997; 1: 345-8. [ Links ]
17. Ciriza C, Dajil S, Jiménez C, Urquiza O, Karpman G, García L, et al. Análisis de la práctica de CPRE durante cinco años en el Hospital del Bierzo. Rev Esp Enferm Dig 1999; 91: 693-7. [ Links ]
18. Halme L, Doepel M, von Numers H, Edgren J, Ahonen J. Complications of diagnostic and therapeutic ERCP. Ann Chir Gynaecol 1999; 88: 127-31. [ Links ]
19. Zinsser E, Hoffmann A, Will U, Koppe P, Bosseckert H. Success and complication rates of diagnostic and therapeutic endoscopic retrograde cholangiopancreatography -a prospective study. Z Gastroenterol 1999; 37: 707-13. [ Links ]
20. Mala T, Lunde OC, Nesbakken A, Aadland E, Stiris M. Endoscopic retrograde cholangiopancreatography -a 4-year retrospective study. Tidsskr Nor Laegeforen 2000; 120: 560-2. [ Links ]
21. Gómez Ponce RL. Complicaciones tempranas de las colangiopancreatografías retrógradas endoscópicas realizadas desde enero de 1998 a diciembre de 2000 en el Hospital Nacional Daniel Alcides Carrión de "El Callao", Perú. Rev Gastroenterol Peru 2002; 22: 33-43. [ Links ]
22. Tzovaras G, Shukla P, Kow L, Mounkley D, Wilson T, Toouli J. What are the risks of diagnostic and therapeutic endoscopic retrograde cholangiopancreatography? Aust N Z J Surg 2000; 70: 778-82. [ Links ]
23. Masci E, Toti G, Mariani A, Curioni S, Lomazzi A, Dinelli M, et al. Complications of diagnostic and therapeutic ERCP: a prospective multicenter study. Am J Gastroenterol 2001; 96: 417-23. [ Links ]
24. Farrell RJ, Mahmud N, Noonan N, Kelleher D, Keeling PW. Diagnostic and therapeutic ERCP: a large single centre's experience. Ir J Med Sci 2001; 170: 176-80. [ Links ]
25. Vandervoort J, Soetikno RM, Tham TCK, Wong RCK, Ferrari AP (Jr), Montes H, et al. Risk factors for complications after performance of ERCP.Gastrointest Endosc 2002; 56: 652-6. [ Links ]
26. Suissa A, Yassin K, Lavy A, Lachter J, Chermech I, Karavan A, et al. Outcome and early complications from ERCP: A prospective single-center study. Gastrointest Endosc 2002; 55: AB157. [ Links ]
27. Barthet M, Lesavre N, Desjeux A, Gasmi M, Berthezene P, Berdah S, et al. Complications of endoscopic sphincterotomy: results from a single tertiary referral center. Endoscopy 2002; 34: 991-7. [ Links ]
28. Rabenstein T, Schneider HT, Bulling D, Nicklas M, Katalinic A, Hahn EGP, et al. Analysis of the risk factors associated with endoscopic sphincterotomy techniques: Preliminary results of a prospective study, with emphasis on the reduced risk of acute pancreatitis with low-dose anticoagulation treatment. Endoscopy 2000; 32: 10-9. [ Links ]
29. Christensen M, Hendel HW, Rasmunssen V, Hojgaard L, Schulze S, Rosenberg J. Endoscopic Retrograde Cholangiopancreatografy causes reduced myocardial blood flow. Endoscopy 2002: 797-800. [ Links ]
30. Baillie J. Complications of ERCP, en ERCP and its applications, IM Jacobson, editor. Filadelfia: Lippincott-Raven, 1998. p. 37-54. [ Links ]
31. Andriulli A, Leandro G, Niro G, Mangia A, Festa V, Gambassi G, et al. Medical treatment can diminish pancreatic damages after ERCP: a metaanalysis. Gastrointest Endosc 2000; 51: 1-7. [ Links ]
32. Baillie J. ERCP training: for the few, not for all. Gut 1999; 45: 9-10. [ Links ]
33. Allison MC, Ramanaden DN, Fouweather MG, Knight Davis DK, Colin-Jones DG. Provision of ERCP services and training in the United Kingdom. Endoscopy 2000; 32: 693-9. [ Links ]
34. Schlup MMT, Williams SM, Barbezat GO. ERCP: a review of technical competency and workload in a small unit. Gastrointest Endosc 1997; 46: 48-52. [ Links ]
35. Yarze JC, Herlihy KJ, Chase MP, Fritz HP. ERCP experience in a community-based, private-practice setting. Am J Gastroenterol 2000; 95: 3006-7. [ Links ]
36. García-Cano Lizcano J, González Martín JA, Pérez Sola A, Morillas Ariño J. Tratamiento endoscópico de la ictericia obstructiva en un hospital de nivel II del Sistema Nacional de Salud. Gastroenterol Hepatol 2001; 24: 287-91. [ Links ]
37. Cotton PB, Williams CB. Practical Gastrointestinal Endoscopy 3rd edition. Londres: Blackwell Scientific Publications, 1990. p. 118. [ Links ]
38. Soehendra N, Binmoeller KF, Seifert H, Scheiber HW. Therapeutic Endoscopy. Color Atlas of Operative Techniques for the Gastrointestinal Tract. Thieme, Stuttgart, 1998. p. 92. [ Links ]
39. Wicks ACB, Robertson GSM, Veitch PS. Structured training and assessment in ERCP has become essential for the Calman era. Gut 1999; 45: 154-6. [ Links ]
40. Cotton PB. How many times have you done this procedure, doctor? Am J Gastroenterol 2002; 97: 522-3. [ Links ]
41. Cotton PB. ERCP is most dangerous for people who need it least. Gastrointest Endosc 2001; 54: 535-6. [ Links ]
42. Luman W, Chan ES-Y. Mathematical model for predicting biliary therapeutic endoscopic retrograde pancreatography (ERCP). Digestive and Liver Disease 2003; 35: 486-92. [ Links ]
43. Taylor AC, Little AF, Hennessy OF, Banting SW, Smith PJ, Desmond PV. Prospective assessment of magnetic resonance cholangiopancreatography for noninvasive imaging of biliary tree. Gastrointest Endosc 2002; 55: 17-22. [ Links ]

