










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.101 no.7 Madrid jul. 2009
PICTURES IN DIGESTIVE PATHOLOGY
Cholangioscopy through a large balloon papillary dilation with two frontal endoscopes: therapeutic and infantile
Colangioscopia con gastroscopio terapéutico e infantil tras dilatación de la papila con balón de gran diámetro
J. Espinel and E. Pinedo1
Services of Digestive Diseases and 1Radiology. Hospital de León. Spain
Case report
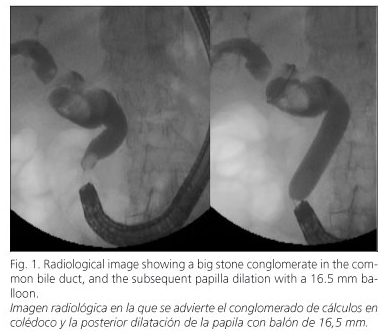
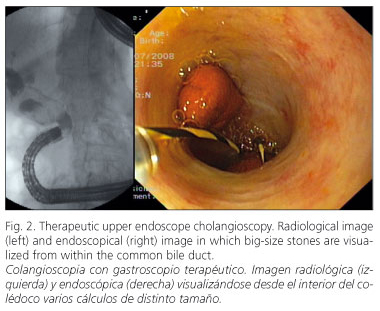
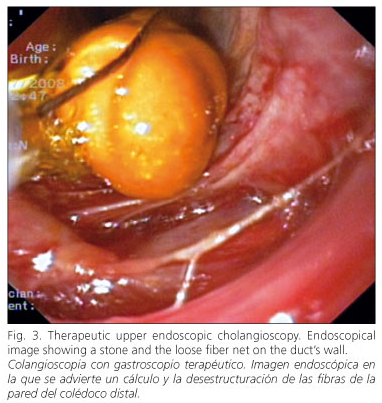
A 98-year-old woman with a medical history of cholecystectomy (12 years ago), partial gastrectomy (10 years ago), pacemaker implanted, and acute coronary syndrome was admitted to hospital for right upper quadrant colicky pain and moderate cholestasis (AST: 37 IU/L, ALT: 25 IU/L, ALP: 164 IU/L, GGT: 65 IU/L, total bilirubin: 0.7 mg/100). An abdominal ultrasound scan revealed an important dilatation of bile ducts due to choledocholithiasis. Endoscopic retrograde cholangiopancreatography (ERCP) was initiated with a therapeutic frontal endoscope. The patient had prior Billroth II surgery and a dilated common bile duct (CBD) due to multiple lithiasis. The biggest stone diameter ranged between 25 and 30 mm. This particular stone seamed to have resulted from the union of 2 or 3 smaller stones, joined together and stuck in the bile duct’s wall, immobile at the extraction maneuver. A 16.5 mm balloon dilation of Vater’s papilla was performed without previous sphincterotomy (Fig. 1). The therapeutic frontal endoscope was introduced along the distal CBD (therapeutic frontal endoscope cholangioscopy) in order to better define and mobilize the biggest stone. The images obtained were very clear (Fig. 2). Stone mobilization was not possible in spite of a Dormia basket and Fogarty balloon. By leaving the therapeutic frontal endoscope into the distal common bile duct, the disappearance of the normal aspect of the bile duct’s wall was noticed and a loose fiber wall net was visualized, announcing the possibility of breakage (Fig. 3). Subsequently, the therapeutic frontal endoscope was replaced by an infantile endoscope in order to reach the stone conglomerate without excessive pressure on the bile duct’s wall. The images obtained were less clear (infantile endoscope cholangioscopy). In spite of all this, stone removal was not possible. During the procedure, which lasted long, a retropneumoperitoneum was observed and consequently the ERCP was interrupted and a polyethylene biliary stent (10F/9 cm) was placed. The patient received conservative treatment afterwards, and left hospital a few days later.
Discussion
Treating difficult-to-extract choledocholithiasis using a large hydrostatic balloon (LHB) (12-20 mm) is an efficient and safe approach recently established in our country (1). Patients with Billroth II and choledocholithiasis are a group that may benefit from this extraction technique (2). LHB may notoriously increase the papilla’s and distal common bile duct’s diameters in order to facilitate big stone removal without lithotripsy. Results are very good, showing that almost 100% of extractions are possible without important complications (3,4). Once dilation is done, how to access the stacked stones that make difficult their capture by lithotripsy baskets remains unsolved.
Cholangioscopy is a technique that may help solve these difficult extractions (5). In our patient, this technique was done with a therapeutic and infantile frontal endoscope, which allowed reaching the distal common bile duct through the dilated papilla and obtaining good-quality images. Working inside the common bile duct was possible and comfortable.
Some problems may emerge: it may not be possible to advance through the common bile duct due to the endoscope’s length; on the other hand, progressive trauma of the wall may be exercised due to the endoscope’s caliber and force, which can result in duct perforation. Nowadays some ERCP systems are available that allow diagnostic cholangioscopy. What still remains to be solved is an improved simplified ERCP system (managed by one endoscopist) with a low cost, fitted with a big enough canal to insert an electrohydraulic lithotriptor, and able to reach, visualize, crumble, and extract big impacted stones.
References
1. Espinel J, Pinedo E, Olcoz JL. Balón hidrostático de gran diámetro en coledocolitiasis. Rev Esp Enferm Dig 2007; 99: 33-8. [ Links ]
2. Espinel J, Pinedo E, Calleja JL, Olcoz JL. Large balloon in the management of bile duct stones. Endoscopy 2007; 39(Supl. I): A372. [ Links ]
3. Espinel J, Pinedo E, Calleja JL, Abreu L. Large-diameter balloon sphincteroplasty for difficult bile stones. Endoscopy 2008; 40(Supl. I): A204. [ Links ]
4. Espinel J, Pinedo E. Dilatación de la papila de Vater con balón de gran diámetro para la extracción de coledocolitiasis. Rev Esp Enferm Dig 2008; 100(10): 632-6. [ Links ]
5. Piraka C, Shah RJ, Awadallah NS, Langer DA, Chen YK. Transpapillary cholangioscopy-directed lithotripsy in patients with difficult bile duct stones. Clin Gastroenterol Hepatol 2007; 5: 1333-8. [ Links ]

