










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.102 no.8 Madrid ago. 2010
Are hepatocellular carcinoma surveillance programs effective at improving the therapeutic options?
Eficacia de los programas de cribado de hepatocarcinoma: ¿mejoran las opciones terapéuticas de estos pacientes?
E. Zapata1, L. Zubiaurre1, A. Castiella1, P. Salvador2, M. García Bengoechea2, P. Esandi2, A. Arriola2, A. Beguiristain3, I. Ruiz3, G. Garmendia4, R. Orcolaga4 and J. M. Alústiza5
1Deparment of Gastroenterology. Hospital de Mendaro.
Departments of 2Digestive Diseases, 3General Surgery and 4Radiodiagnosis. Hospital Donostia.
5OSATEK Donostia-San Sebastián, Guipúzcoa, Spain
ABSTRACT
Aim: to evaluate whether the current surveillance programs (ultrasonography and alpha-fetoprotein testing every six months) are successful in detecting patients in the early stages.
Material and methods: the health records of all patients diagnosed with hepatocellular carcinoma in Donostia Hospital between 2003 and 2005 were reviewed retrospectively. Eighty-five patients (11 women and 74 men) were included in the study and demographic data, risk factors and clinical data were obtained. Patients were split into two groups according to whether or not they had been included in a surveillance program.
Results: seventy per cent of patients of the surveillance group is diagnosed in early stage opposite to 26.7% of patients in no surveillance group (p < 0.05). Thirteen patients cannot receive curative treatment in spite of the diagnosis in early stage (9 in the surveillance group and 4 in the no surveillance group. The global sensibility of the surveillance program in our series is 95%.
Conclusions: current hepatocellular carcinoma surveillance programs, which comprise six-monthly ultrasonography and alpha-fetoprotein tests, are highly sensitive and effective. These programs result in the detection of hepatocellular carcinoma in its early-stages, when potentially curative treatment may be offered.
Key words: Hepatocellular carcinoma. Surveillance. Ultrasonography. Abdominal echography. Alpha-fetoprotein.
RESUMEN
Objetivo: determinar si la utilización en nuestro medio del programa de cribado de HCC establecido -alfa-fetoproteína (AFP) y ecografia semestral- en pacientes con hepatopatía crónica permite detectar pacientes en estadios precoces de la enfermedad.
Material y métodos: Diseño experimental: estudio retrospectivo. Criterios diagnósticos de HCC: 2 o más técnicas de imagen con lesión hipervascular mayor de 2 cm o 1 técnica de imagen con lesión hipervascular mayor de 2 cm asociado a AFP mayor de 400 ng/ml. Pacientes: 85 pacientes diagnosticados de HCC en el Hospital Donostia entre los años 2003 y 2005. Datos analizados: información demográfica (sexo, edad), factores de riesgo (alcohol, virus de hepatitis, hemocromatosis, otras enfermedades asociadas), e información clínica (etiología de la hepatopatía, estadio de Child-Pugh, determinación de AFP, hallazgos radiológicos, criterios de resecabilidad, tratamiento recibido, evolución). Se divide la muestra en dos grupos según hubieran seguido o no un programa de cribado.
Resultados: el 70% de los pacientes del grupo de cribado se diagnostican en estadio precoz frente al 26,7% del grupo de no cribado (p < 0,05). Trece pacientes no pueden recibir tratamiento curativo a pesar del diagnóstico en fase precoz (9 en el grupo de cribado y 4 en el de no cribado). La sensibilidad global del cribado en nuestra serie es del 95%.
Conclusiones: en nuestro medio, el programa de cribado de hepatocarcinoma es eficaz en términos de aplicación de tratamientos curativos.
Palabras clave: Hepatocarcinoma. Cribado. Hepatopatía crónica. Ecografía abdominal. Alfa-fetoproteína.
Introduction
Hepatocellular carcinoma (HCC) is the most common primary malignant tumour of the liver and the fifth most frequent malignant tumour in the world (third in terms of mortality) (1). The incidence in patients with cirrhosis is 3 to 5% and it is the main cause of mortality for this patient group (2). It is more common among men than women and the incidence increases progressively with age. There are many risk factors for HCC and they act in combination, thus encouraging the clinical and genetic heterogeneous characteristic of this neoplasm. Generally patients remain asymptomatic until the tumour is in an advanced stage.
HCC treatment depends on the stage of the tumour, the degree of liver dysfunction and the clinical characteristics of the tumour (3). Three treatments are currently considered to have curative potential: surgical excision, liver transplant and percutaneous ablation (4). In order for any of these treatment options to be feasible, however, the HCC must be diagnosed at an early stage (up to three nodules under 3 cm diameter or one nodule under 5 cm) and fulfil certain criteria relating to the stability and slow progression of the underlying liver pathology. This restriction on therapeutic options makes it all the more necessary to set up surveillance programs that allow patients to be diagnosed in early stages.
HCC fulfils the necessary requirements for establishing a surveillance program: it is a frequently occurring neoplasm (the fifth most common in the world), with high morbidity and mortality rates; the target population is easy to identify (patients with cirrhosis) and the diagnostic tools are readily available (ultrasound and/or alpha-fetoprotein). While HCC surveillance programs are controversial, most international societies -European Association for the Study of the Liver, EASL (5), American Associaation for the Study of Liver Diseases, AASLD (6)- recommend their use in patients with high risk of developing the condition. A large number of studies have demonstrated that the use of such programs leads to an increase in the application of curative treatments and therefore survival rates (3,7-15).
The aim of the present study is to determine whether the use of the standard HCC surveillance program, which comprises six-monthly ultrasonography and alpha-fetoprotein (AFP) testing in patients with chronic liver disease, is successful in detecting patients in early stages of HCC, who would be candidates for potentially curative treatment.
Methods
The health records of patients diagnosed with HCC in Donostia Hospital (a tertiary reference hospital in Gipuzkoa Province, Basque Country, Spain) between 2003 and 2005 were reviewed retrospectively. The criteria used for diagnosis were those established by the EASL (two or more imaging techniques showing a hypervascular lesion greater than 2 cm diameter or one imaging technique showing a hypervascular lesion greater than 2 cm diameter in combination with serum AFP level higher than 400 ng/ml).
Information was obtained about the 85 patients who fulfilled the inclusion criteria, including demographic data (sex and age), risk factors (alcohol, hepatitis virus, hemochromatosis and other associated illnesses) and clinical data (cause of the liver disease, Child-Pugh classification, AFP test, X-ray findings, operability, treatment received, progress).
The sample was split into two groups depending on whether or not patients had been part of an HCC surveillance program, this being understood as a monitoring strategy comprising six-monthly ultrasonography and AFP tests. The AFP level considered as abnormal was 7 IU/ml and above, which is the standard value used in our hospital.
The two groups were compared in terms of demographic and clinical characteristics, using Student's t-test for comparison of continuous variables and the chi-square test for quantitative variables, taking statistical significance as p < 0.05.
Early-stage HCC was defined as a stage in which therapeutic treatment may be offered, in other words, three nodules less than 3 cm diameter or a single nodule less than 5 cm. The two groups were compared for the percentage of patients diagnosed in this stage.
Results
From 2003 to 2005, 85 patients were diagnosed with HCC in Donostia Hospital, comprising 74 men and 18 women, with a mean age of 63. The most common cause of liver disease was alcohol (38 patients, 44.7%), followed by viral hepatitis (32 patients, 37.64%), mixed cause (alcohol and virus) (8 patients, 9.4%), hemochromatosis (3 patients, 3.5%) and "other" (4 patients, 4.7%). With regard to the Child-Pugh classification for severity of liver disease at the time of diagnosis, 43 patients (50.6%) were identified as class A, 19 (22.3%) as class B and 22 patients (25.9%) as class C. Forty of these patients (47.1%) were in an early detection HCC surveillance program involving six-monthly ultrasound and AFP tests, while 45 patients (52.9%) were diagnosed incidentally or due to their presenting advanced symptoms of HCC. The demographic characteristics and Child-Pugh classifications for both groups are displayed in table I, where statistically significant differences can be observed with regard to aetiology (virus being the most common cause in the surveillance group compared to alcohol in the non-surveillance group) and stage of the liver disease (in the surveillance group, the majority of diagnosed patients were Child-Pugh class A, compared with the non-surveillance group, in which the majority of patients were class B or C at the time of HCC diagnosis).
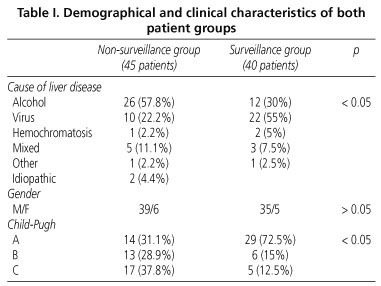
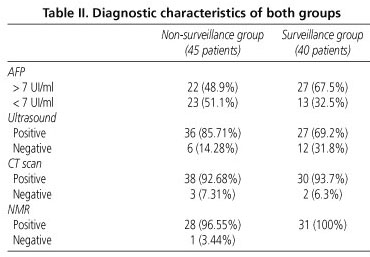
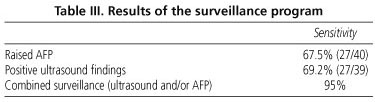
In the patient group that was under surveillance, the most common cause was virus (55%), followed by alcohol (30%) (Table I). Of the patients in this group, 72.5% were Child-Pugh class A at the time of HCC diagnosis, 15% were class B and 12.5%, class C. During the surveillance program, 27 patients (67.5%) were found to have high AFP levels and 27 (69.2%) had ultrasound diagnosis of a tumour (Table II). The sensitivity of the surveillance program (one of the two tests positive, or both) was 95% (Table III).
In the patient group that was not under surveillance, the most common cause was alcohol (57.8%), followed by virus (22.2%). The distribution according to Child-Pugh categories was as follows: 28.9% of patients were identified as class A, 31.1% as class B and 37.8%, class C (Table I).
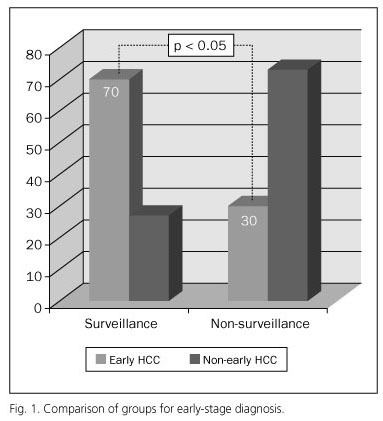
With regard to early HCC diagnosis, 70% (28 patients) of the surveillance group were diagnosed at an early stage compared to 26.7% (12 patients) of the group that was not under surveillance. This difference is statistically significant (p < 0.05). Of those patients in the surveillance group who were diagnosed according to the criteria as early-stage HCC, nine were unable to receive curative treatment due to a variety of reasons: portal hypertension (6 patients), liver failure (1 patient) or the underlying pathology (2 patients). In the non-surveillance group, 4 out of the 12 patients diagnosed at an early stage did not receive potentially curative treatment because they presented with portal hypertension. On removing from the statistical analysis those patients for whom curative treatment was not a suitable option, due to the advanced stage of their liver disease (Child-Pugh class C), 71% of the remaining surveillance group patients were diagnosed in an early stage and were possible candidates for potentially curative treatment, compared to 29% of the non-surveillance group. This difference is statistically significant (p < 0.05).
Discussion
The aim of this investigation is to analyse wether current HCC surveillance programs are effective in detecting patients in a sufficiently early stage of the disease as to be able to offer them potentially curative treatment.
The clinical guidelines from the main scientific societies -EASL (5), AASLD (6)- recommend the use of surveillance in patients at risk of developing HCC. The available scientific evidence also supports the use of such programs. One recent study carried out in China (8) in a population suffering from chronic viral hepatitis who had also been diagnosed with HCC, showed that patients included in a surveillance program were diagnosed with smaller tumours (4.2 vs. 7.7 cm) and in lesser number (2.6 vs. 3.8) than those that were diagnosed incidentally or as a result of their symptoms, and that these differences were statistically significant. The surveillance program also resulted in a significantly greater survival rate (88 vs. 26 weeks), due to the increased number of patents who were candidates for surgical treatment or ablation techniques. Similar results were found by Tanaka and colleagues (9) in a Japanese investigation involving 384 patients with chronic liver disease caused by hepatitis C and diagnosed with HCC, 182 of whom had been included in a surveillance program and who were compared with the remainder, who had not. They report that at the time of diagnosis, the tumours were significantly smaller (19 vs. 35 mm) in the surveillance group, with a greater incidence of single tumours (67 vs. 46%) and a higher survival rate (46 vs. 32%). Another randomised study comparing a surveillance and non-surveillance group, demonstrated benefits in terms of the number of patients infected with hepatitis B who were suitable for potentially curative treatment, independent of the presence of cirrhosis (10). Another randomised, controlled clinical study carried out in China (11), also showed that patients included in a surveillance program had a greater probability of being diagnosed in early stages and of receiving potentially curative treatments, with a 37% reduction in mortality in these patients. A population-based cohort study in Italy (12) found that patients with cirrhosis caused by hepatitis C who were included in a surveillance program had 29% greater probability of being treated by liver resection, 28% greater probability of being treated with percutaneous ethanol injection and 60% greater probability of prolonging their survival.
While surveillance programs are not yet well established, it is suggested that they be set at six-month intervals, given that the available data shows that this is the best way of detecting tumours smaller than 3 cm. The available tools are AFP testing -sensitivity 39-64%, specificity 76-90%, positive predictive value (PPV) 9-32%) and ultrasonography (sensitivity 71%, specificity 93%, PPV 14%- (13). A recent systematic review of the literature (14) identified six-monthly ultrasound combined with AFP testing as the most recommendable surveillance strategy, given that it triples the number of early-stage diagnoses and therefore the probability of patients receiving potentially curative treatment.
In the present series, the overall sensitivity of the surveillance program was 95%, which suggests that six-monthly ultrasonography and AFP testing identify the majority of affected patients.
If the aim of surveillance programs is to detect HCC in stages in which potentially curative treatment may be offered, these programs should be reserved for those patients who are capable of receiving such treatment. For this reason, patients with underlying pathologies that prevent definitive treatment or patients with advanced liver disease (Child-Pugh class C) should be excluded. In the present series, 70% of patients in the surveillance program were diagnosed in an early stage, compared to 26.7% of those not in the program (p < 0.05), although approximately one third of these patients could not receive potentially curative treatment due to their underlying pathology or the advanced stage of their liver disease. If those patients unable to receive curative treatment are removed from the statistical analysis, a significant difference remains between the two groups. Recently, Pascual et al. (15) published a prospective study containing evidence that HCC surveillance programs increase patient survival, but not of those in the most advanced stages of the illness. They obtained a significantly greater survival rate in patients diagnosed with HCC who were in a surveillance program (27 months) compared to those who were diagnosed outside of any such program (6 months), identifying the following as independent predictive factors of an increase in survival: Child-Pugh class A and the fact of being diagnosed within a surveillance program.
The main limitations of the present investigation are its nature as a retrospective study and the small number of patients analysed. It would be interesting to carry out prospective studies that would allow the long-term results of current surveillance programs to be evaluated with greater reliability, especially with regard to patient survival.
In conclusion, this investigation has demonstrated the effectiveness of current HCC surveillance programs in identifying candidates for potentially curative treatments. While HCC is a tumour that meets the necessary requirements for establishing surveillance programs among risk groups, prospective studies are needed in order to demonstrate the effectiveness of these programs in terms of survival and their cost-effectiveness, as well as studies determining the best available tools. As new, improved diagnostic methods and therapeutic options are developed, these surveillance programs will doubtless need to become even more sensitive and specialised, in order to detect the greatest possible number of patients who are able to benefit from these new possibilities.
References
1. Parkin DM. Estimating the World cancer burden: GLOBOCAN 2000. Int J Cancer 2001; 94: 153-6. [ Links ]
2. Colombo M, Dr Franchis R, Del Ninno E, Sangiovanni A, De Fazio C, Tommasini M, et al. Hepatocellular carcinoma in Italian patients with cirrosis. N Engl J Med 1991; 325: 675-80. [ Links ]
3. Bolondi L, Sofía S, Siringo S, Gaiani S, Casali A, Zironi G, et al. Surveillance programme of cirrhotic patients for early diagnosis and treatment of hepatocellular carcinoma: a cost effectiveness analysis. Gut 2001; 48: 251-9. [ Links ]
4. Llovet M. Updated treatment approach to hepatocellular carcinoma. J Gastroenterol 2005; 40: 225-35. [ Links ]
5. Bruix J, Sherman M, Llovet JM, Beaugrand M, Lencioni R, Burroughs AK, et al. Clinical management on hepatocellular carcinoma. Conclusion of the Barcelona-2000. EASL conference. J Hepatol 2001; 35: 421-30. [ Links ]
6. Bruix J, Sherman M. Management of hepatocellular carcinoma. Hepatology 2005; 42: 1208-36. [ Links ]
7. Sangiovanni A, Del Ninno E, Fusoni P, De Fazio C, Ronchi G, Romeo R, et al. Increased survival of cirrhotic patients with a hepatocellular carcinoma detected during surveillance. Gastroenterology 2004; 126: 1005-14. [ Links ]
8. Wong GL, Wong VW, Tan GM, Ip KI, Lai WK, Li YW, et al. Surveillance programme for hepatocellular carcinoma improves the survival of patients with chronic viral hepatitis. Liver Int 2008; 28: 79-87. [ Links ]
9. Tanaka H, Nouso K, Kobashi H, Kobayashi Y, Nakamura S, Ohnishi Y, et al. Surveillance of hepatocellular carcinoma in patients with hepatitis C virus infection may improve patient survival. Liver Int 2006; 26(5): 543-51. [ Links ]
10. Zhang BH, Yang BH, Tang ZY. Randomized controlled trial of screen-ing for hepatocellular carcinoma. J Cancer Res Clin Oncol 2004; 130: 417-22. [ Links ]
11. Yang B, Zhang B, Xu Y, Wang W, Shen Y, Zhang A, et al. Prospective study of early detection for primary liver cancer. J Cancer Res Clin Oncol 1997; 123: 357-60. [ Links ]
12. Giannini E, Arzani l, Borro P, Botta F, Fasoli A, Risso D, et al. Does surveillance for hepatocellular carcinoma in HCV cirrhotic patients improve treatment outcome mainly due to better clinical status at diagnosis? Hepatogastroenterology 2000; 47: 1395-8. [ Links ]
13. Collier J, Sherman M. Screening for hepatocellular carcinoma. Hepatology 1998; 27: 273-8. [ Links ]
14. Thompson Coon J, Rogers G, Hewson P, Wright D, Anderson R, Cramp M, et al. Surveillance of cirrhosis for hepatocellular carcinoma: systematic review and economic analysis. Health Technology Assessment 2007; 11(34). [ Links ]
15. Pascual S, Irurzun J, Zapater P, Such J, Sempere L, Carnicer F, et al. Usefulness of surveillance programmes for early diagnosis of hepatocellular carcinoma in clinical practice. Liver Int 2008; 682-9. [ Links ]
![]() Correspondence:
Correspondence:
Eva Zapata Morcillo.
Área de Aparato Digestivo.
Hospital de Mendaro.
Barrio Mendarozabal, s/n.
20850 Mendaro. Gipúzcoa, Spain.
email: evingerzap@yahoo.es;
evamaria.zapatamorcillo@osakidetza.net
Received: 24-02-10.
Accepted: 30-04-10.

