










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.103 no.5 Madrid may. 2011
https://dx.doi.org/10.4321/S1130-01082011000500012
LETTERS TO THE EDITOR
Gallstone ileus with spontaneous resolution
Íleo biliar con resolución espontánea
Key words: Gallstone ileus. Spontaneous resolution. Intestinal obstruction.
Dear Editor,
Gallstone ileus is an unusual cause of intestinal obstruction. It is caused by impaction of one or more gallstones that enter the intestinal lumen via a cholecystoenteric fistula. Gallstone ileus is sometimes a challenge clinically and delayed diagnosis could carry a significant rate of complication and mortality. Resolution of gallstone ileus by spontaneous evacuation of gallstone is extremely rare. We present a case of gallstone ileus patient with a severe comorbidity, treated with conservative treatment successfully by spontaneous evacuation of gallstone.
Case report
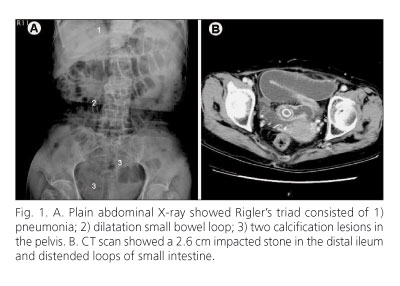
A 71-year-old woman developed nausea, abdominal fullness and intermittent colicky pain for 10 days. She had an incidentally finding of gallstones by health survey half year ago. She had medical history of a huge thyroid nodule (10 x 6 cm), hypertension, atrial fibrillation and ischemic heart disease. On presentation, her vital signs revealed temperature of 36.4 oC, pulse of 97 /min and blood pressure of 160/88 mmHg. Physical examination showed distended, mild tender abdomen and hyperactive bowel sound. The blood tests showed white blood count of 11,700/ul with 93% neutrophils and normal biochemical values as electrolytes, liver function and amylase. Abdominal X-ray showed pneumobilia, dilated small bowel loop and two calcified lesions (Fig. 1A). Computed tomography revealed pneumobilia, distended loops of small intestine without ischemic pattern, a 2.6 cm impacted stone in the distal ileum (Fig. 1B). The diagnosis of gallstone ileus was made. Evaluating the clinical condition and stone size, conservative treatment was considered to be a benefit for the high surgical risk patient. She received the nasogastric tube decompression and fluid resuscitation. Sixteen hours later, the patient got diarrhea with clinical improvement.
Discussion
Gallstone ileus is an uncommon cause with 1-3% in all mechanical small bowel obstruction (SBO), but frequently seen in elderly patients (1). Plain abdominal radiography has an important role in the assessment of SBO. Rigler triad is a classically radiographic signs of gallstone ileus, consisted of pneumobilia, bowel loop dilatation and ectopic stone. Ultrasound and computer tomography (CT) scan could apply prompt diagnosis for gallstone ileus (2). Kasahara reported a gallstone must be at least 2.5 cm to result in intestinal obstruction (3). Our experience presented CT could offer crucial evidence for the diagnosis of gallstone ileus and the accurate size of gallstone (4). In the literature, surgical exploration was done for gallstone ileus with stones sized larger than 3 cm at least. Our patient presented complicated high surgical risk due to severe comorbidity of heart, huge thyroid nodule. The successful conservative treatment was achieved by appropriate image findings, careful evaluation of stone size and clinical symptoms. Our case suggested an optional conservative management for gallstone patients with stone sized between 2.5 and 3 cm, particularly in high risk surgical condition.
Kuo-Feng Hsu1, Jyh-Cherng Yu1, Chung-Bao Hsieh1, De-Chuan Chan1,
Yuan-Min Chang1, Peng-Jen Chen2, Chih-Yung Yu3 and Guo-Shiou Liao1
1Division of General Surgery, Department of Surgery. Tri-Service General Hospital.
National Defense Medical Center. Taipei, Taiwan. Republic of China.
2Division of Hepatogastroenterology, Department of Medicine. Tri-Service General Hospital.
National Defense Medical Center. Taipei, Taiwan. Republic of China.
3Department of Radiology. Tri-Service General Hospital.
National Defense Medical Center. Taipei, Taiwan. Republic of China
References
1. Clavien PA, Richon J, Burgan S, Rohner A. Gallstone ileus. Br J Surg 1990;77:737-42. [ Links ]
2. Shrake PD, Rex DK, Lappas JC, Maglinte DD. Radiographic evaluation of suspected small bowel obstruction. Am J Gastroenterol 1991;86:175-8. [ Links ]
3. Lassandro F, Gagliardi N, Scuderi M, Pinto A, Gatta G, Mazzeo R. Gallstone ileus analysis of radiological findings in 27 patients. Eur J Radiol 2004;50:23-9. [ Links ]
4. Yu CY, Lin CC, Shyu RY, Hsieh CB, Wu HS, Tyan YS, et al. Value of CT in the diagnosis and management of gallstone ileus. World J Gastroenterol 2005;11:2142-7. [ Links ]

