










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.103 no.8 Madrid ago. 2011
https://dx.doi.org/10.4321/S1130-01082011000800014
LETTERS TO THE EDITOR
Splenic arterial dissection and factor V Leiden mutation causing massive spleen infarction
Disección arterial esplénica y factor V de Leiden como causa de infarto esplénico masivo
Key words: Spleen infarction. Splachnic artery dissection. Factor V Leiden.
Palabras clave: Infarto esplénico. Disección arteria esplácnica. Factor V de Leiden.
Dear Editor,
Arterial dissection is a very rare complication affecting splachnic arteries. We report here a massive spleen infarction due to a dissection of splenic artery associated to factor V Leiden mutation.
Case report
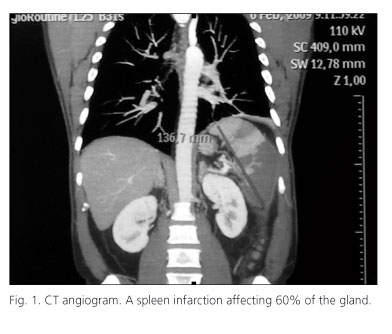
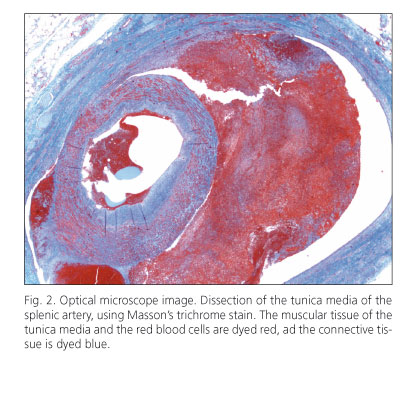
A 48 year-old man was referred to emergency ward because of pain on the left side of the abdomen and low-grade fever, triggered by moderate physical exercise. He smoked 20 cig./day but denied hypertension, diabetes or dislipidemia. Physical examination was unremarkable. Serum biochemistry showed total cholesterol 255 mg/dL, LDL cholesterol 167 mg/dL, HDL cholesterol 35 mg/dL and triglycerides 250 mg/dL. EKG, heart and abdominal ultrasound were normal. An abdominal scan showed a spleen infarction affecting 60% of the gland. A CT angiogram and a selective celiac trunk angiogram showed a reduction of the lumen of the splenic artery, suggesting dissection and mild atherosclerosis (Fig. 1). Test for prothrombotic states confirmed the G1691A factor V Leiden mutation. After being admitted to the hospital, enoxaparin was administered and the spleen was surgically removed. Pathological examination confimed both splenic infarction and arterial dissection (Fig. 2). Patient was discharged with warfarin and atorvastatin.
Discussion
Our report shows an unusual case of massive splenic infarction associated with splenic arterial dissection in a smoker and dislipemic middle-aged adult, carrier of G1691A factor V Leiden mutation. Splachnic arterial dissection is exceptional (1), mainly asymptomatic, few occasions with abdominal pain, and usually found incidentally during an X-ray examination looking for any disease (2). Splachnic arterial dissection has been associated to vascular risk factors, atherosclerosis, fibromuscular dysplasia, abdominal trauma, systemic disorders and vascular inflammation (2,3). Outcomes ranges from spontaneous cure to occlusion, aneurism or rupture (2). Non complicated cases are managed with antiplatelet or anticoagulant therapy and blood pressure control (3), but surgery is indicated when thrombosis, occlusion, rupture or ischemia develops (3-5).
In a recent review, just 1 out 24 cases with celiac trunk dissection had splenic infarction (2). The G1691A factor V Leiden confers resistance to activated protein C and increases risk for deep vein thrombosis and pulmonary embolism (6). Although an association to arterial thrombosis has not been reported, we believe the mutation of factor V Leiden found in our patient contributed to the thrombosis and massive infarction triggered by splenic arterial dissection.
In conclusion, we support that splenic artery dissection should be included in the list of conditions causing acute abdominal pain, especially among middle-aged men.
Ángela Muñoz-García1, Manuel Abarca-Costalago2, Isabel Hierro-Martín3 and Pedro Valdivielso-Felices2
Departments of 1Digestive Diseases, 2Internal Medicine and 3Pathology. Hospital Clínico Universitario Virgen de la Victoria. Málaga, Spain
References
1. Muller MF, Kim D. Spontaneous dissection of the hepatic artery. Abdom Imaging 1995;20(5):462-5. [ Links ]
2. Nordanstig J, Gerdes H, Kocys E. Spontaneous isolated dissection of the celiac trunk with rupture of the proximal splenic artery: a case report. Eur J Vasc Endovasc Surg 2009;37(2):194-7. [ Links ]
3. Takayama T, Miyata T, Shirakawa M, Nagawa H. Isolated spontaneous dissection of the splanchnic arteries. J Vasc Surg 2008;48(2):329-33. [ Links ]
4. Sparks SR, Vasquez JC, Bergan JJ, Owens EL. Failure of nonoperative management of isolated superior mesenteric artery dissection. Ann Vasc Surg 2000;14(2):105-9. [ Links ]
5. Glehen O, Feugier P, Aleksic Y, Delannoy P, Chevalier JM. Spontaneous dissection of the celiac artery. Ann Vasc Surg 2001;15(6):687-92. [ Links ]
6. Palomo I, Pereira J, Alarcon M, Pinochet C, Velez MT, Hidalgo P, et al. Factor V Leiden and prothrombin G20210A among Chilean patients with venous and arterial thrombosis. Rev Med Chil 2005;133(12):1425-33. [ Links ]

