










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.104 no.8 Madrid ago. 2012
https://dx.doi.org/10.4321/S1130-01082012000800011
LETTERS TO THE EDITOR
Recurrent acute pancreatitis as clinical presentation of hydatid disease of the liver
Pancreatitis aguda de repetición como presentación clínica de hidatidosis hepática
Key words: Hydatid disease of the liver. Hydatid cyst. Pancreatitis.
Palabras clave: Hidatidosis hepática. Quiste hidatídico. Pancreatitis.
Dear Editor,
Echinococcosis is a parasitic zoonoses transmitted by dogs in which humans are intermediary hosts. It is caused by parasites of the genus Echinococcus. In the United States and Europe most infections occur in immigrants from endemic areas, including South America, the Mediterranean region and many areas of China. In humans, 50-75% of hydatid cysts occur in the liver and usually are solitary cysts (72%) (1).
Case report
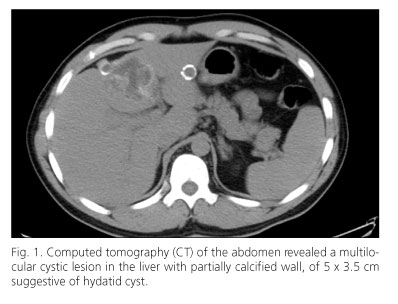
A 37 year-old male native of Morocco, was admitted into the hospital because of intense right upper quadrant pain, irradiated to his back, without other symptoms. The patient reported previous episodes of intense epigastric pain for 6-7 years. Laboratory data showed: amylase 1,544 U/L, total bilirubin 6.9 mg/dL, aspartate aminotransferase 92 U/L, alanine aminotransferase 201 U/L, alkaline phosphatase 289 U/L, gamma glutaryl transpeptidase 304 U/L and C-reactive protein 2.1. He was diagnosed with acute pancreatitis. Abdominal ultrasound scan revealed multiple septated cystic images in the liver with a honeycomb appearance, suggestive of hydatidosis; a normal gallbladder and bile ducts were also found. The study was completed with a computed tomography of abdomen identifying a multilocular cystic lesion, with a partially calcified wall, located in liver segments II-III of 5 x 3.5 cm. Another lesion of similar characteristics was located in segment IV of 7.5 x 6 x 5.5 cm in close contact with the gallbladder, causing pressure or mass effect on its upper surface, without dilatation of bile ducts. These findings were compatible with hydatid cysts (Fig. 1). The pancreas was enlarged and hyperechoic particularly at the body, without peripancreatic exudates. Hydatid serology (indirect hemagglutination) was positive (1/2,560). The patient was treated with albendazole: 400 mg every 12 hours and the episode was solved without complications and he was included on waiting list for cholecystectomy and resection of hydatid cysts. He suffered three episodes of acute acalculous mild pancreatitis while he was waiting for surgery. Finally, the patient underwent cholecystectomy and right hepatectomy without complications, remaining asymptomatic since then.
Discussion
Hydatid disease of the liver frequently produces no symptoms for many years (2). In 9-25% of cases, hydatid cyst can rupture into the biliary tree causing transient or complete obstruction of the bile duct (3) with jaundice, cholangitis and occasionally acute pancreatitis. The rupture of hydatid cysts into the billiary tree might cause severe anaphylaxis, impairing patient survival.
Ideal treatment is still controversial, although the recommended approach is surgery, especially when complications exist, there are other therapeutic options, such as medical therapy and puncture, aspiration, instillation and re-aspiration of the cyst (PAIR), widely extended in uncomplicated cysts. The choice of treatment depends on several factors: number and location of the cysts, surgeon experience, and presence of complications (4). Albendazole is the most effective antihelminthic drug and should be used in most cases combined with surgical treatment, and as primary therapy for patients with severe comorbidities, very small or asymptomatic cysts, multiple cysts or of difficult surgical access. It is also used in patients who refuse surgery (5,6).
María José Rodríguez-Sicilia, Cristina González-Artacho, María José Cabello-Tapia,
Paloma de-la-Torre-Rubio and Javier de-Teresa-Galván
Department of Gastroenterology. Hospital Virgen de las Nieves. Granada, Spain
References
1. Akcan A, Sozuer E, Akyildiz H, Ozturk A, Atalay A, Yilmaz Z. Predisposing factors and surgical outcome of complicated liver hydatid cysts. World J Gastroenterol 2010;16:3040-8. [ Links ]
2. Frider B, Larrieu E, Odriozola M. Long-term outcome of asymptomatic liver hydatidosis. J Hepatol 1999;30:228. [ Links ]
3. Bedirli A, Sakrak O, Sozuer EM, Kerek M, Ince O. Surgical management of spontaneous intrabiliary rupture of hydatid liver cysts. Surg Today 2002;32:594-7. [ Links ]
4. Ramia JM, de la Plaza R, Casares M, Ramiro C, Veguillas P, Quiñones J, et al. Profile of patients with hepatic hydatid disease not treated surgically. Rev Esp Enferm Dig 2011;103(9):448-52. [ Links ]
5. Nahmias J, Goldsmith R, Soibelman M, el-On J. Three-to-7-year follow-up after albendazole treatment of 68 patients with cystic echinococcosis (hydatid disease). Ann Trop Med Parasitol 1994;88:295-304. [ Links ]
6. Stojkovic M, Zwahlen M, Teggi A, Vutova K, Cretu CM, Virdone R, et al. Treatment response of cystic echinococcosis to benzimidazoles: a systematic review. Trop Dis 2009;3:524. [ Links ]

