










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 texto en
texto en  Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.104 no.9 Madrid sep. 2012
https://dx.doi.org/10.4321/S1130-01082012000900016
LETTERS TO THE EDITOR
Hepatocellular carcinoma in non-cirrhotic liver
Carcinoma hepatocelular sobre hígado no cirrótico
Key words: Fibrolamellar hepatocellular carcinoma. Cirrhosis.
Palabras clave: Carcinoma hepatocelular fibrolamelar. Cirrosis.
Dear Editor,
Hepatocellular carcinoma (HCC) is the most common primary malignant neoplasm of the liver, the sixth leading cause of cancer and the third leading cause of cancer death (1). It develops on cirrhotic liver in 80% of cases, appearing in a 20% on healthy livers (fibrolamellar variant) or with noncirrhotic chronic liver disease (2). We report the case of a young woman with a large liver mass without evidence of chronic liver disease.
Case report
A 29-year-old woman who presented fever and epigastric discomfort was palpable a painful hepatomegaly at the expense of the left hepatic lobe (LHL) (no other findings in the rest of the examination). An abdominal sonography showed a heterogeneous lesion of 10 cm in diameter located in the LHL, without signs of chronic liver diseases. A bolus injection of sulfur hexafluoride contrast sonograhy (SonoVue®) showed that the lesion had an enhancement in the arterial phase with progressively less-enhancing in the venous phase. This behavior was compatible with HCC.
The liver tests showed minimum pattern of cholestasis (GGT 58 UI/L [< 38], FA 198 UI/L [30-120] with normal bilirubin) and minimum increase in transaminases (GOT 41 UI/L [< 31], GPT 28 UI/L [< 34]). A chronic liver disease was rule out:
- Serology: Anti-VHC, Ag-HBs, Anti-HB core, Anti-HBs, CMV, VEB, and VIH negatives.
- Immunology: IgG, 1,060 mg/dL (725-1,900); IgA, 161 mg/dL (50-340); IgM, 241 mg/dL (45-280). ANA, AMA, anti-LKM and anti-ML negatives.
- Copper metabolism: ceruloplasmin, 53.4 mg/dL (27-50).
- Iron metabolism: Iron, 29 μg/dL (60-180); IST, 7% (15-50); ferritin, 141 ng/mL (8-140).
- Lipoprotein profile: total cholesterol, 181 mg/dL (< 200); HDL, 51 mg/dL (> 40), and triglycerides, 95 mg/dL (< 200).
- Thyroid hormones: TSH 1.46 μUI/L (0.27-4.2); T4L, 1.45 ng/dL (0.93-1.7).
- α-1 antitrypsin, 2.94 g/L (2.1-5).
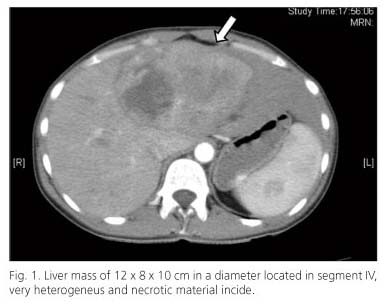
The α-feto-protein was in the normal range (1.33 ng/ml). Given these findings, it was performed a biopsy of the lesion. The result was fibrolamellar hepatocarcinoma. Metastatic disease was rule out with thoracic-abdominal scan (CT) and bone gammagraphy. The CT confirmed the heterogeneous liver mass which had a 12 x 8 x 10 cm in diameter and was located in segment IV. It was irrigated by the left hepatic artery (Fig. 1). A left hepatectomy was performed without relapse within 3 years after diagnosis.
Discussion
Fibrolamellar hepatocellular carcinoma usually occurs among young patients having distinctive clinical, histological and prognostic features (3-5). It usually presents as abdominal pain and abnormal liver biochemistry. Typically, they do not increase the α-feto-protein, showing similar features to conventional hepatocellular carcinoma in the radiologic studies. Histologically, they are formed by very eosinophilic large hepatocytes, surrounded by fibrous bands, which separating the cells in trabeculae or nodules (6). Although diagnostic is made with higher sizes than conventional HCC, curative treatments are applied in the majority of patients, with a low mortality (7,8) and a superior survival compared with cirrhotic patients (from 74 to 97% and from 38 to 86% at 1 and 3 years, respectively, in studied series) (9).
In our case, the possibility of performing an abdominal contrast sonography helped to establish the diagnosis, which was confirmed by histological and analytical studies.
Laura Casanova-Martínez, Pilar Castillo-Grau, Marta Jaquotot-Herranz,
Gloria Ruiz-Fernández, Eun Jin Han, Lucía Tortajada-Laureiro, Antonio Olveira-Sanz,
Francisco Gea-Rodríguez and José María Segura-Cabral
Department of Digestive Diseases. Hospital La Paz. Madrid, Spain
References
1. Forner A, Ayuso C, Real MI, Sastre J, Robles R, Sangro B, et al. Diagnóstico y tratamiento del carcinoma hepatocelular. Med Clin (Barc) 2009;132:272-87. [ Links ]
2. Renedo F, De la Revilla J, Calleja JL. Carcinoma hepatocelular. Medicine 2008;10:770-6. [ Links ]
3. McLarney J, Rucker P, Bender G, Goodman Z, Kashitani N, Ros P. Fibromamellar carcinoma of the liver: radiologic-pathologic correlation. RadioGraphics 1999;19:453-71. [ Links ]
4. Brancatelli G, Federle M, Grazioli L, Carr B. Hepatocellular carcinoma in noncirrhotic liver: CT, clinical, and pathologic findings in 39 U.S. residents. Radiology 2002;222:89-94. [ Links ]
5. Ichikawa T, Federle M, Grazioli L, Madariaga J, Nalesnik N, Marsh W. Fibromamellar hepatocellular carcinoma: imaging and pathologic findings in 31 recent cases. Radiology 1999;213:351-61. [ Links ]
6. Kew M. Tumores y quistes hepáticos. En: Sleisenger and Fordtran, editors. Enfermedades gastrointestinales y hepáticas. Fisiopatología, diagnóstico y tratamiento. 8aed. Philadelphia: Saunders; 2008. p. 2007-58. [ Links ]
7. Ramia JM, Villara J, Muffaka K, Medinab A, Garrotea D, Ferróna JA. Hepatocarcinoma en hígado no cirrótico. Cir Esp 2006;80:111-3. [ Links ]
8. Zeng W, Gouw A, Van den Heuvel M, Molema G, Poppema S, Van der Jagt E, et al. Hepatocellular carcinomas in cirrhotic and noncirrhotic human livers share angiogenic characteristics. Ann Surg Oncol 2010; 17:1564-71. [ Links ]
9. Núñez O, Matilla A, Merino B, Díaz A, Colón A, Botella ER, et al. Estudio descriptivo de la experiencia sobre carcinoma hepatocelular en hígado no cirrótico. Gastroenterol Hepatol 2011;34:322-8. [ Links ]

