










Mi SciELO
 Servicios personalizados
Servicios personalizadosServicios Personalizados
Revista
Articulo
 Inglés (pdf)
Inglés (pdf)
 Articulo en XML
Articulo en XML Referencias del artículo
Referencias del artículo
 Enviar articulo por email
Enviar articulo por emailIndicadores
-
 Citado por SciELO
Citado por SciELO -
 Accesos
Accesos
Links relacionados
-
 Citado por Google
Citado por Google -
 Similares en
SciELO
Similares en
SciELO -
 Similares en Google
Similares en Google
Compartir

 Permalink
PermalinkRevista Española de Enfermedades Digestivas
versión impresa ISSN 1130-0108
Rev. esp. enferm. dig. vol.106 no.7 Madrid jul./ago. 2014
PICTURES IN DIGESTIVE PATHOLOGY
Pancreatic dysontogenetic cysts
Quistes disontogénicos pancreáticos
Eduardo Rodrigues-Pinto1, Pedro Pereira1, Rui Cunha2 and Guilherme Macedo1
1Gastroenterology Department and 2Radiology Department. Centro Hospitalar São João. Porto, Portugal
Case report
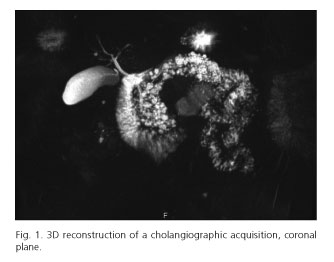
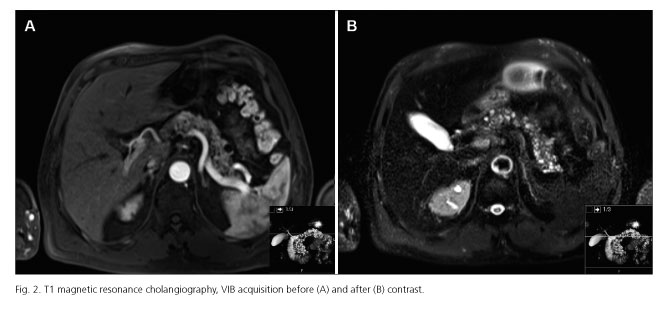
A male patient, 57-years-old, was submitted to abdominal imaging for study of urinary complaints. He had no complaints suggestive of pancreatic disease, no history of smoking, alcohol consumption or family history of pancreatic diseases. Abdominal imaging revealed multiple hypodense lesions mainly on the body and tail of the pancreas, consistent with cystic pancreatic formations (Figs. 1 and 2) with associated parenchymatous calcifications without Wirsung dilatation or solid nodular lesions suggestive of malignancy. He also had multiple renal cysts. Remaining exams revealed no other changes. Pancreatic cysts are present in 2.4-13.5 % of patients without known pancreatic disease (1). Accurate categorization is important since some of them have malignant potential and should be resected. Pancreatic cysts are broadly classified as congenital-developmental cysts, retention cysts, duplication cysts, pseudocysts, neoplastic cysts and parasitic cysts (2). An important differential diagnosis is branch duct intraductal papillary mucinous neoplasm (IPMN). It is accepted that true cysts occur as a result of developmental anomalies related to the sequestration of primitive pancreatic ducts. In the presenting case, there was no previous history of pancreatitis or other pancreatic diseases, the patient was asymptomatic and also had renal involvement by cysts. His pancreatic cysts were multiple, small and diffusely involve the body and tail of pancreas. IPMNs are an important differential diagnosis, due to prognosis implications; however, Wirsung had a normal calibre, with no dilatation. Dysontogenetic pancreatic cysts are a very rare entity that may occur singly or in association with renal cysts, liver, central nervous system or retinal abnormalities (3). Currently there are no well-defined diagnostic criteria for dysontogenetic pancreatic cysts. Therefore it is important to always consider differential diagnosis, namely IPMNs, due to different needs of follow-up.
References
1. de Jong K, Nio CY, Mearadji B, Phoa SS, Engelbrecht MR, Dijkgraaf MG, et al. Disappointing interobserver agreement among radiologists for a classifying diagnosis of pancreatic cysts using magnetic resonance imaging. Pancreas 2012;41:278-82. [ Links ]
2. Rowe MI, O'Neill JA Jr, Grosfeld JL, Fonkalsrud EW, Coran AG, editors. Essentials of pediatric surgery. Disorders of the pancreas. Louis MO: MosbyYear Book; 1995. p. 663-74. [ Links ]
3. Nygaard KK, Walters W. Polycystic disease of the pancreas (Dysontogenetic cysts): Report of a case with partial pancreatectomy. Ann Surg 1937;106:49-53. [ Links ]

